Medevac Misadventure – Inquest in the Yukon
The Coroner for Canada’s Yukon Territory has recommended a review of procedures for medical evacuations (medevacs) following the death on board an air ambulance of a 31 year-old woman from Carmacks in November 2013, CBC has reported.
In particular the wrong IV tubing was taken on the aircraft as different sizes tubes were stored in the same storage location. This is a classic human performance influencing factor that increases the risk of human error.
The key medevac recommendations are below:
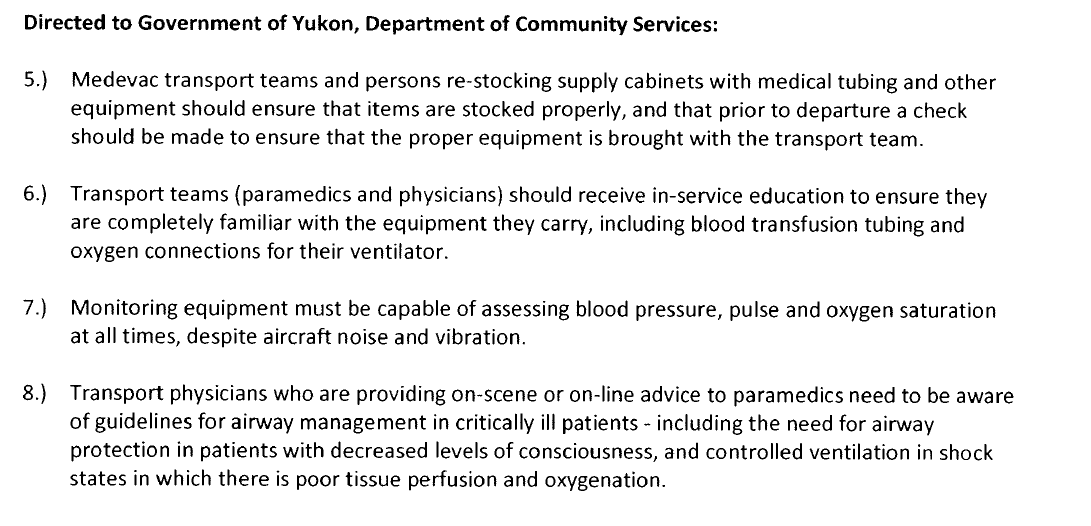
The Coroner’s full judgement is here.
Health Minister Doug Graham subsequently said:
We believe that our systems are pretty good right now, but they need some improvement so we’ve agreed with the recommendations and we’ll be following through and dealing with them as quickly as we can.
He also says there are now checklists for emergency equipment.
Medevac Misadventure – Observations
While these recommendations will be of interest to medevac providers they are also relevant to organisations, for example in the energy and resource sectors (e.g. mining, oil and gas companies), who contract for medevac support.
At one end of the spectrum this can be done through a single turnkey contract for both aircrafts and medical provision using specially fitted out air ambulance aircraft or as part of a helicopter SAR contract (as discussed by Aerossurance earlier this year). These have the benefit that aircrew and medical crew are familiar with each others procedures and requirements plus medical carry-on equipment is usually ‘kitted’ specifically for air medevacs. In other cases the aviation and medical provision is contracted separately.
At the other end of the spectrum, worst case, are scenarios where medevacs are conducted only very occasionally, on aircraft normally used for passenger duties, with medical staff who normally man normal site clinics, with minimal equipment, only gathered together at the time of the call out, that is not necessarily compatible with aircraft use, with limited medevac procedures or exercises.
If this sounds like your current arrangements, perhaps it is time to look more closely.
The hazards are not only related to patient safety. Among the highest risk scenarios are night-time call outs, where there is a long history of fatal air accidents. In offshore operations a study by the International Association of Oil and Gas Producers (OGP) Aviation Sub-Committee (ASC) Night Operations Working Group suggests the risk at night has been 5.25 times that of day operations. This is why the Night Operations Working Group introduced a specific control on a policy for emergency night flights into their bow-tie risk assessment:
Control 1.6 Emergency Night Flight Policy: An Emergency Night Flight Policy should be established in all circumstances when night flights can reasonably be expected to be requested in response to medical, weather or other emergencies. OGP Members, in consultation with the air operator, should develop, using a risk assessment methodology, a documented night medevac/emergency policy. This should be issued to both parties and have a suitable level of authorisation to request such flights. In recognition of their higher risk, night offshore emergency flights should only be requested in genuinely life-threatening situations where the risk of waiting until first light is considered to outweigh the risk of an emergency night flight. Once the cause of the emergency is over, subsequent flights, such as for re-manning, should be conducted under the Non-Emergency Night Flight Policy. Pilots should be rostered for night stand-by duty in accordance with the principles in [OGP Aircraft Management Guidelines] AMG Section 5.6.6.
The award winning Flight Safety Foundation (FSF) Basic Aviation Risk Standard (BARS) has a similar requirement.
Also: Transport Canada‘s guidance on air ambulance operations can be found here.
Topical Accidents: HEMS Night Accident and Offshore Medevac Fatality
A topical illustration of inappropriate night operations is given by the recent issue by the US National Transportation Safety Board (NTSB) of their probable cause of accident that killed the 3 crew aboard an Air Evac EMS Inc operated helicopter emergency service (HEMS) Bell 206L1 during a positioning flight at night in patch fog: “The pilot’s loss of helicopter control due to spatial disorientation when he inadvertently encountered night, instrument meteorological conditions, which resulted in the in-flight separation of the main rotor and tailboom.”

Wreckage of B206L1 N114AE (Credit: Charles Bertram, Herald Leader)
Medevac teams always need to expect the unexpected though: Earlier in the year Aerossurance also reported on a case when a patient was able to somehow fatally fall from a helicopter in the cruise.
UPDATE 12 Dec 2014: TriState CareFight, which operates air medical transport services, has been named in a lawsuit by the family of a New Mexico man who died while en route to a hospital after the transport helicopter reportedly ran out of on-board oxygen.
Other Safety Resources
- Fatal Flaws in Canadian Medevac Service Investigators uncovered mods, maintenance, training, W&B and briefing discrepancies. Highlights importance of mindful contracting for air services.
- The Tender Trap: SAR and Medevac Contract Design Aerossurance’s Andy Evans discusses how to set up clear and robust contracts for effective contracted HEMS operations.
Recent Comments