USAF UH-1N SAR Helicopter Hoist Training Accident
On 27 April 2011, a USAF Bell UH-1N, 69-6603 of the 512th Rescue Squadron, 58th Special Operations Wing, Kirtland AFB, NM was performing hoist training when it was destroyed in an accident.

Wreckage of USAF UH-1N 69-6603 at Kirtland AFB, NM (Credit: USAF)
The Accident Flight
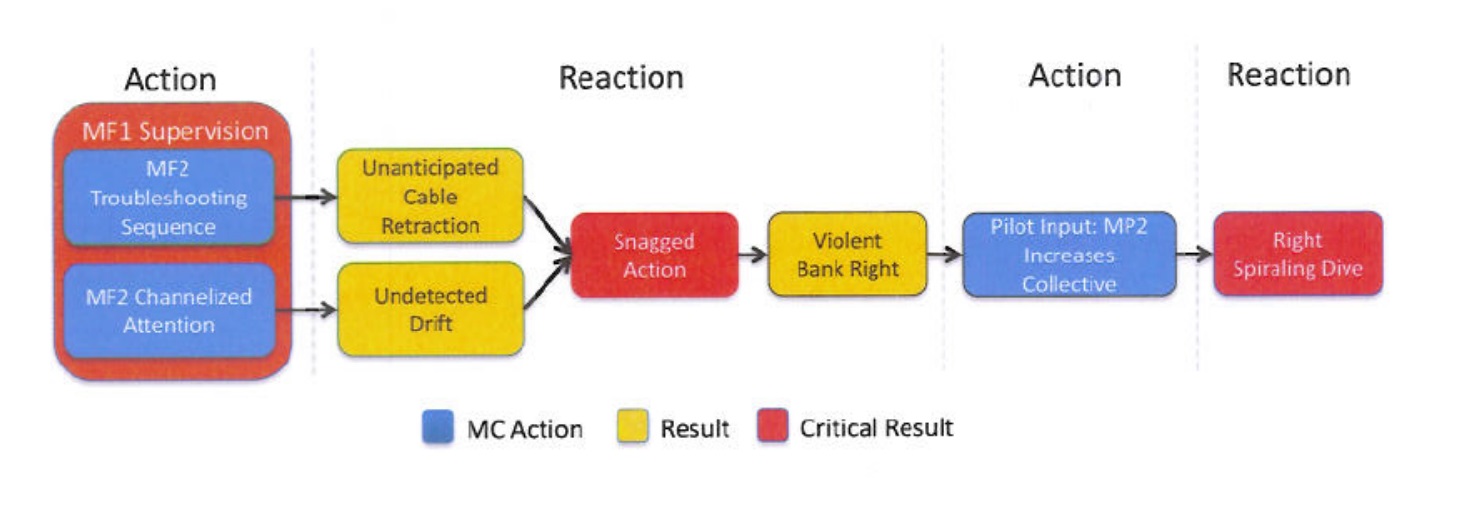
This accident was during an initial instructor flight engineer check ride. According to the USAF Accident Investigation Board (AIB) report: The training site was at 5382 feet AMSL, c 11ºC and wind was c 12 kts gusting 20 kts. The Evaluating Flight Engineer was controlling the up-limit switch on the hoist to simulated a malfunction. The student Flight Engineer tried several fault finding options. During this time an undetected aircraft drift forward and left occurred, positioning the aircraft 5 to 10 feet west of a discarded 2060 lbs (934 kg) F-111 escape capsule. The crew had used this as a landmark at ‘Site 15’ within the Kirtland range.
Once the student Flight Engineer identified the simulated malfunction was caused by activation of the up-limit switch they swiped the other Flight Engineer’s hand away from the switch. This allowed cable retraction to resume. The co-pilot however was however still making an input to the pilot’s hoist control switch, as had been requested as part of the fault finding, when the up limit switch was released. As a result, the hoist cable retracted inadvertently and a rescue device, called a ‘forest penetrator‘, on the end of the hoist cable, snagged on the capsule.

Forest Penetrator (Credit: USAF U.S. Air Force / Tech. Sgt. Erik Gudmundson)

F-111 Escape Capsule and Forest Penetrator Recovered (Credit: USAF)

Accident Site (Credit: USAF)
The pilot flying instinctively pulled up on the collective and the helicopter entered a descending right turn while tethered to the capsule and impacted sloping ground just 3-5 seconds after the snag.

UH-1 Accident Flight Path After Snag (Credit: USAF)
Two crew members attempted to activate the cable cutter but this occurred only factionally before impact.
The crew of four all suffered either minor or no injuries and the aircraft was partial-consumed in a post crash fire after they egressed. The Integrated Data Acquisition Recorder (IDAR), a type of Flight Data Recorder (FDR) and the Cockpit Voice Recorder (CVR) were both damaged. No data could be obtained from either of them.
Analysis
The normal trouble shooting sequence for up-limit switch failure has the pilot try his hoist control switch two steps after the flight engineer has already ensured the up limit switch actuator is not in the up position.
In this case the first steps of the pendant failure troubleshooting sequence were executed followed by the first step for up limit switch failure. It was not confirmed the pilot had release his hoist control.
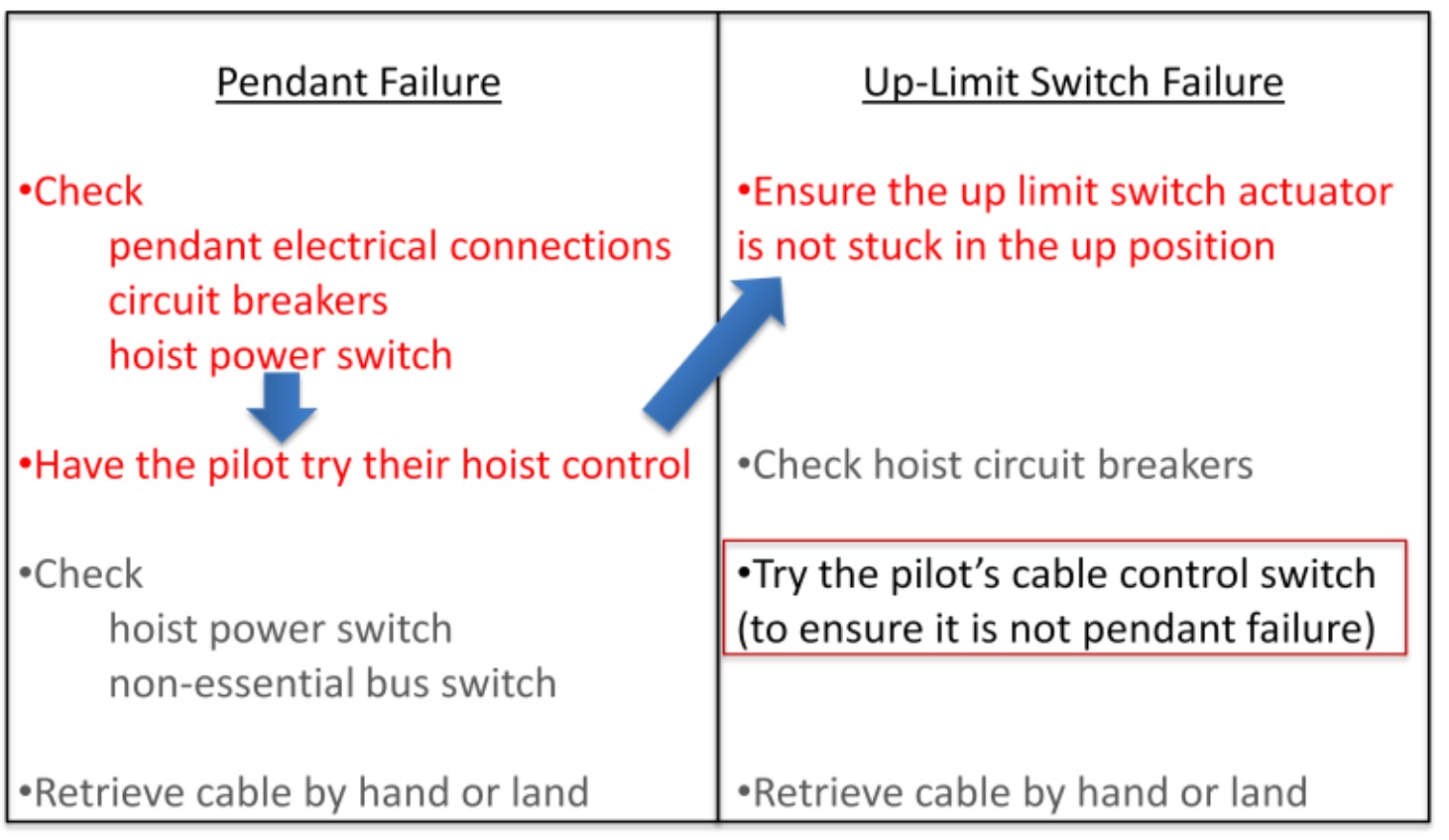
This non-standard sequence resulted in an unanticipated full rate cable retraction, as the pilots’ controls operate at full rate only (unlike the variable rate from the hoist operators pendant).
USAF AIB Human Factor’s Analysis
The investigators applied the the DoD Human Factors Analysis and Classification System (DoD-HFACS) taxonomy based on the work of Wiegmann and Shappell. They identified 7 relevant factors:
(1) SP007 Authorized Unnecessary Hazard (Level 2: Supervision)
This is a factor when “supervision authorizes a mission or mission element that is unnecessarily hazardous without sufficient cause or need”:
The F-111 capsule had been on Site 15 for over a decade. At one point aluminum sheeting covered all the openings, but several panel coverings were missing at the time of the mishap. Without these panels, the capsule was an entanglement hazard. Previous site surveys noted the F-111 capsule’s presence. Multiple members in the 512 RQS verified that the capsule was a frequently-used reference point for operations. (The valuator Flight Engineer] selected an aim point for the hoist approximately 10 to 15 feet from the capsule.
(2) PC102 Channelized Attention (Level 3: Precondition)
This is a factor when “the individual [sic] is focusing all conscious attention on a limited number of environmental cues to the exclusion of others of a subjectively equal or higher or more immediate priority, leading to an unsafe situation. This may be described as a tight focus of attention that leads to the exclusion of comprehensive situational information.”
The Flight Engineer is responsible for clearing the aircraft of obstacles on the side and rear, directing the pilots’ inputs for aircraft position and altitude, and monitoring the hoist during its operation. [The Flight Engineer undergoing the check ride] channelized his attention on troubleshooting the hoist malfunction. [The Evaluator FE] was focused on his student’s actions. Due to [their] channelized attentions, neither initially noticed the aircraft drifting or the hoist cable retracting and lifting the penetrator.
(3) PP102 Cross-Monitoring Performance (Level 3: Precondition)
This is a factor when “crew or team members failed to monitor, assist or back-up each other’s actions and decisions”.
Since [the Evaluator FE] was sitting and [not]standing over [the Student], he was unable to visually monitor the forest penetrator. This placed him in a position where he could not quickly recognize and correct the impending unsafe situation.
(4) PP112 Miscommunication (Level 3: Precondition)
This is a factor when “correctly communicated information is misunderstood, misinterpreted or disregarded.
Both Flight engineers state a “stop up” call was clearly communicated by [the Evaluator FE]. The pilots did not hear a stop up call.
(5) PP110 Mission Briefing (Level 3: Precondition)
This is a factor when “information and instructions provided to individuals, crews, or teams were insufficient, or participants failed to discuss contingencies and strategies to cope with contingencies”.
The aircraft commander did not attend the portion of the briefing that related to this exercise. The AIB highlight that while the commander “was fully aware of how to cope with those contingencies, his attendance at that brief was expected and required”.
(6) PP205 Inadequate Rest (Level 3: Precondition)
This is a factor when “the opportunity for rest was provided but the individual failed to take the opportunity to rest”.
The Student Flight Engineer was on a night schedule two days prior to the accident. “Per squadron policy, he was given one day prior to the day [flight] to shift his sleep cycle. [The Flight Engineer] did not change his sleep schedule on his day off and only slept for 5 hours the night prior”.
(7) AE101 Inadvertent Operation (Level 4: Unsafe Act)
This is a factor when an “individual’s movements inadvertently activate or deactivate equipment, controls or switches when there is no intent to operate the control or device. This action may be noticed or unnoticed by the individual”.
The AIB point to the co-pilot’s inadvertent hoist control input.
Our Observations on the HFACS Analysis
Its odd the non-standard procedure is not explicitly coded nor the factors behind the unnoticed drift or the failure to cut the cable. This demonstrates that just because an appropriate tool is used it doesn’t mean the analysis is rigorous.
VIDEO of forest penetrator hoist training
Other Safety Resources
The European Safety Promotion Network Rotorcraft (ESPN-R) has a general helicopter safety discussion group on LinkedIn and a Hoist Operation Safety Promotion LinkedIn group.
- Tail Rotor Pitch Control Loss During Hoisting: Fatal NASC Airbus Helicopters AS365N3 hoisting accident
- Fatal Fall From B429 During Helicopter Hoist Training
- Marine Pilot Transfer Winching Accident
- Swedish Special Forces SPIES and Military SMS
- Hoist Assembly Errors: SAR Personnel Dropped Into Sea
- SAR Crew With High Workload Land Wheels Up on Beach
- UPDATE 30 October 2019: ‘Crazy’ KC-10 Boom Loss: Informal Maintenance Shift Handovers and Skipped Tasks
- UPDATE 30 November 2019: Fall From Stretcher During Taiwanese SAR Mission (NASC AS365N2 NA-104)
- UPDATE 14 December 2019: Fatal Taiwanese Night SAR Hoist Mission (NASC AS365N3 NA-106)
- UPDATE 27 December 2019: Fatal Powerline Human External Cargo Flight
- UPDATE 19 April 2020: SAR Helicopter Loss of Control at Night: ATSB Report
- UPDATE 2 May 2020: Sécurité Civile EC145 SAR Wirestrike
- UPDATE 11 May 2020: European Search and Rescue (SAR) Competition Bonanza
- UPDATE 20 March 2021: SAR AW139 Dropped Object: Attachment of New Hook Weight
- UPDATE 15 May 2021: Military SAR H225M Caracal Double Hoist Fatality Accident
- UPDATE 27 November 2021: TCM’s Fall from SAR AW139 Doorway While Commencing Night Hoist Training
- UPDATE 19 February 2022: SAR Hoist Cable Snag and Facture, Followed By Release of an Unserviceable Aircraft
The European Aviation Safety Agency (EASA) is sponsoring a safety promotion activity on hoist operations.
On error management:
…and our review of The Field Guide to Understanding Human Error by Sidney Dekker presented to the Royal Aeronautical Society (RAeS): The Field Guide to Understanding Human Error – A Review
Recent Comments