RCAF Production Pressures Compromised Culture
We look at the production pressures that affected the culture of a Royal Canadian Air Force (RCAF) training unit according to accident investigators.
The Accident Flight
On 24 January 2014 Beechcraft CT156 Harvard II (T-6A Texan II) 156102 suffered a hard landing during a student’s second practice forced landing (PFL), in a flapless configuration in strong winds. The aircraft was from 2 Canadian Forces Flying Training School (2 CFFTS), of 15 Wing at Moose Jaw, SK, part the NATO Flying Training in Canada (NFTC) Program. The Qualified Flight Instructor (QFI) took control and initiated a go-around. A chase plane confirmed that the left main landing gear (MLG) side-brace had become detached from the MLG.
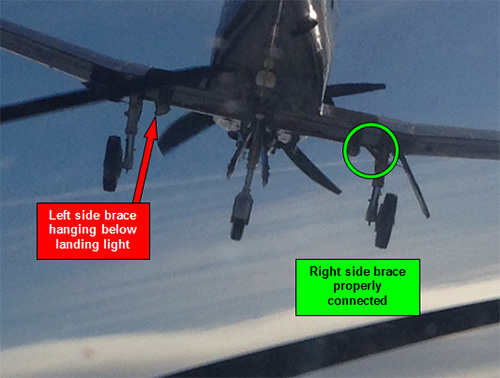
CT156 Harvard II (T-6A Texan II) CT156102 with Detached Left MLG Side-Brace (Credit: RCAF)
Unsuccessful attempts were made to attain a symmetrical gear up configuration for a possible belly landing. Consequentially, it was decided that a controlled ejection was the safest option. Both crew successfully ejected, with only minor injuries, overhead the airfield at 5400’ mean sea level (MSL) (approximately 3400’ AGL) and an indicated airspeed of 139 kts. 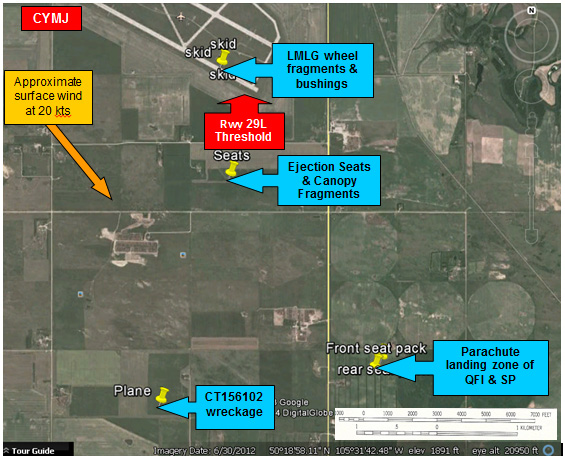 The aircraft was destroyed in the subsequent crash in farmland approximately 2 nm south of the airfield.
The aircraft was destroyed in the subsequent crash in farmland approximately 2 nm south of the airfield.

CT156 Harvard II (T-6A Texan II) CT156102 Main Wreckage Site (Credit: RCAF)
Conclusions of the Safety Investigation
The RCAF investigators say in their report (available saved as a PDF here):
Investigation by Quality Engineering Test Establishment (QETE) found sufficient evidence to conclude that this bolt failed in tension overload during the hard landing allowing the side brace which controls movement of the LMLG strut and provides a down lock to become detached.
Furthermore:
The investigation found that a need to increase pilot production at 2 CFFTS had resulted in a revised TP [Training Plan]. The new TP was put into effect coincidental with the QFI’s pilot training in 2012. The revised syllabi made significant modifications to the previous syllabi; most noteworthy was a significant reduction in the number of flying missions that could include PFL training.
The 2012 reduction of in-flight PFL training was not recognised as significant and so no risk mitigating measures such as applying more restrictive limitations to PFLs has been introduced.
The investigation concluded that the practice of completing PFLs in a flapless configuration with no formal training was contributory to this accident, as was the decrease in PFL training which likely resulted in this QFI having significantly less PFL experience following the Flying Instructor Course (FIC) than previous pipeline QFIs in 2 CFFTS.
A preventive measure (PM) was implemented following this accident which established a safety window restricting the practice of flapless PFLs. Additional PMs relating to Aviation Life Support Equipment (ALSE), the Integrated Data Acquisition Recorder (IDAR), QFI personal limits and unit culture are recommended.
While the report discusses in depth matters such as course design, training procedures and operations, data recording, safety equipment etc, we will look closely at their examination of unit culture.
Unit Culture, Production Pressures and Instructor Currency
The investigators say:
While it is difficult to assess and measure the culture of a unit, there was sufficient testimony to indicate the likelihood that the 2 CFFTS culture was unhealthy at the time of the occurrence.
The investigators say that interview evidence and results from these 2 CFFTS Flight Safety (FS) Surveys in 2012 & 2014…
…indicate that flying student missions routinely took priority over QFI proficiency missions. The surveys also highlighted concerns about QFI and student workloads, length of work days, fatigue, quality of life, low proficiency levels among QFIs, pressure to complete missions, among others.
The pressure to produce 125 graduate pilots per year appears to have been behind the cultural issues within 2 CFFTS. This pressure created a culture to prioritize student missions over SCT [Staff Continuation Training] missions – intended for pilots to maintain currency and proficiency – and played a direct role in this accident.
Production pressures are uncovered in many accident investigations. In sociologist Prof Diane Vaughan‘s seminal work The Challenger Launch Decision, one phenomena she used to explain the 1987 shuttle disaster was the concept of a ‘culture of production’. As one book review commented (emphasis added):
Vaughan’s book is not an expose of bureaucratic wrong-doing. Rather, it is a detailed analysis of how decision-making occurs in organizations, and how even rigorous internal and external monitoring will not avert disaster; indeed, the chilling conclusion she draws is that wrong decisions will be made not in spite of but because of rules and procedures. In this respect, The Challenger Launch Decision is a sobering analysis of the consequences of increasing dependence on complex technologies.
In this case:
Once this pressing mindset was set in motion, the organization did what it felt appropriate and necessary to achieve the aim. Stakeholders quickly modified and implemented revised TPs, arguably prematurely, and then the 15 Wing CoC [Chain of Command] micromanaged mission scheduling with the emphasis on prioritizing student missions…
…despite cautions from senior and experienced staff within the QFI cadre at 2 CFFTS, 15 Wing leadership remained focussed on achieving the challenging target that had been established.
The investigators highlight that the 2 CFFTS Orders states the following:
Flight Commanders are to ensure that Staff Continuation Training (SCT) is given sufficient priority to ensure that the 1 Cdn Air Div minimum flying requirements are respected. This will ensure that QFIs maintain a high level of instructional and flying proficiency…
However, this positive commitment is watered down by the second sentance concluding less assertively [emphasis added]:
…and may, on occasion, require that SCT flying have priority over Student Training.
SCT flying was also not a specific currency requirement. Furthermore…
…one interpretation of the rules was that a QFI who required an Annual Proficiency Check (APC) didn’t necessarily need to complete minimum currency requirements because the APC would essentially reset the requirements given that an APC re-qualifies a QFI whose currency has lapsed.
The investigators found that…
…senior leadership or operations personnel, would on occasion address Flight Schedulers directly to have them replace QFI currency or proficiency missions with student missions…
…repeated micromanagement, with direction to replace SCT missions with student missions, implicitly sent the message that student missions were of a higher priority than QFI proficiency.
There was resistance:
Several CFS and 2 CFFTS staff members testified having tried to make QFI currency and proficiency missions a higher priority. The 2012 & 2014 FS Surveys also highlighted concerns about proficiency taking a back seat to student mission accomplishment.
However:
Recommendations to make QFI proficiency a higher priority were not supported by the CoC within 15 Wing in that a culture had been established to prioritize student missions as a result of scheduling micromanagement by the CoC.
On the morning of the accident:
….the Flt Comd [Flight Commander] directed that only student missions be scheduled for that particular wave due to pressure within 2 CFFTS to push student missions.
The QFI [who had coordinated to fly a SCT mission, including PFLs, with an experienced QFI in that wave] was reluctant to object, cognizant of the culture to prioritize student training over QFI proficiency.
An [further] indication reflecting the high tempo of 2 CFFTS operations is the fact that the mission card for the ACH6 mission, flown the day prior, had not been written prior to the QFI being scheduled to fly the ACH7 mission. The comment regarding the lack of sufficient nose up attitude by the SP [Student Pilot] during the flapless final turn on the previous mission may have alerted the QFI to anticipate the error which resulted in the hard landing, thereby providing the QFI with a greater chance of preventing it.
In conclusion:
The investigation determined that there existed, at the time of the accident, an underlying culture that QFI proficiency was not a high priority, and that Flt Comds and schedulers acted within that culture.
The investigation recommended that:
- 2 CFFTS Orders be amended to remove the existing ambiguity [with respect to] currencies, proficiency and SCT missions
- Clearly highlight the importance of QFIs developing and maintaining a high level of proficiency.
RCAF Director of Flight Safety Comments
Training the future pilots of the RCAF is a daunting task, particularly when RCAF pilot manning levels are low and there exists limited experience within the cadre of qualified instructor pilots. 15 Wing has maintained an excellent safety record overall while achieving this aim since the introduction of NFTC. The entire staff who have contributed to the force generation of RCAF and expatriate pilots over the course of this training program are to be commended for a job well done.
There exists a delicate balance between quantity and quality when setting course standards, and that balance has cycled in both directions over the many years that the RCAF’s pilot training system has existed. Attempts to do more with less in the current context of continuous operational and financial optimum efficiencies have routinely been made, in the RCAF as well as throughout society. However, there will typically always be some level of compromise in quality if or when quantity becomes the focus. In an effort to graduate more pilots, a revised TP reduced the overall number of flying missions and thereby reduced the overall airborne experience level of NWGs from that of previous graduates.
Possibly due to the somewhat hasty implementation of the new TP, the effect of doing this was not fully considered and/or understood in the 2012 re-design of the Phase II and Phase III pilot courses. Performance standards were maintained despite the reduction in training and mitigating initiatives were not fully considered. Though surely not done intentionally, the QFI was essentially set up for this sort of occurrence to take place due to a lack of consideration for the possible effects of the reduction in PFL training during the 2012 redesign of the Harvard Phase II & III courses, exacerbated by the culture within 2 CFFTS to prioritize student missions over QFI proficiency.
This culture shift was likely very insidious and most probably not intentional. This is where the leadership, at all levels, need to be careful in the messaging of their intent as it can have undesired effects (e.g. a culture shift) and potentially introduce safety risks.
Manning and experience levels of aircrew within the RCAF are likely to continue to be low in coming years, or at the very least less than what we were used to seeing some years ago. It is imperative that the leadership consider the potential impact this may have.
RCAF commanders across each fleet of aircraft need to assess the performance of NWGs arriving at their units and address any concerns they may have with 2 Cdn Air Div. This will be particularly important in the future when pilot training transitions towards the use of even more simulation which will likely further reduce the amount of airborne flying training. The RCAF’s ability to maintain the same level of operational capabilities as when there existed a higher level of experience should continually be reassessed.
Note: our emphasis added above.
Our Observations
Its encouraging that a systemic approach has been taken rather than over-focus on judging the immediate decisions and actions prior to the accident flight as advocated by some ‘just culpability’ zealots, who market proprietary culpability decision aids (as we discussed in Leadership and Trust and in A Railroad’s Cult of Compliance). While the Director of Flight Safety gives forthright advice in his comments, perhaps disappointingly the safety investigation report makes no specific recommendations on cultural matters and how to be mindful of such cultural pressures. This is an area where Aerossurance has practical, proven experience.
Other Safety Resources
- High G Drama at Cold Lake
- Crew Bag FOD Shatters Hawk Canopy
- USMC CH-53E Readiness Crisis and Mid Air Collision Catastrophe
We highly recommend this case study: ‘Beyond SMS’ by Andy Evans (our founder) & John Parker in Flight Safety Foundation, AeroSafety World, May 2008, which discusses the importance of leadership in influencing culture. You may also be interested in these Aerossurance articles:
- How To Develop Your Organisation’s Safety Culture positive advice on the value of safety leadership and an aviation example of safety leadership development.
- How To Destroy Your Organisation’s Safety Culture a cautionary tale of how poor leadership and communications can undermine safety.
- Safety Intelligence & Safety Wisdom
- HROs and Safety Mindfulness
- Consultants & Culture: The Good, the Bad and the Ugly
As Aerossurance’s Andy Evans notes in this co-written article: Safety Performance Listening and Learning – AEROSPACE March 2017:
Organisations need to be confident that they are hearing all the safety concerns and observations of their workforce. They also need the assurance that their safety decisions are being actioned. The RAeS Human Factors Group: Engineering (HFG:E) set out to find out a way to check if organisations are truly listening and learning.
The result was a self-reflective approach to find ways to stimulate improvement.
UPDATE 7 April 2018: Investigators Criticise Cargo Carrier’s Culture & FAA Regulation After Fatal Somatogravic LOC-I. A Shorts 360 N380MQ, operated by SkyWay Enterprises as a Part 135 flight on contract to FedEx crashed in the Caribbean after the crew likely suffered a Somatogravic Illusion raising the flaps on a dark night in 2014. The lack of an FAA SMS regulation for Part 135, the operator’s poor safety culture and implications for the wider industry culture stand out in a thoughtful accident report.
UPDATE 15 April 2018: Comments were made of poor leadership and culture after a US Navy training accident with a Boeing T-45C: Leadership failures in Navy pilot training squadrons led to Tennessee T-45 crash (described further here). The Navy investigation concluded the instructor pilot was “flat-hatting”; flying and directing his student to fly too close and too fast to ground in a manner not conducted during basic flying training. The report said that such unauthorized training had become part of culture in VT-7. There was also no record the instructor had completed the requisite training in the T-45C either.
UPDATE 10 November 2018: Korean T-50 Accident at Singapore Airshow
UPDATE 13 November 2018: Inadequate Maintenance, An Engine Failure and Mishandling: Crash of a USAF WC-130H: investigators discuss a strong cultural overtone in this accident that killed 9.
UPDATE 17 November 2018: Investigation into F-22A Take Off Accident Highlights a Cultural Issue
UPDATE 18 December 2018: USAF Engine Shop in “Disarray” with a “Method of the Madness”: F-16CM Engine Fire
UPDATE 13 January 2019: Pathological to Generative. Moving up the Regulation Culture Ladder with Bruce.
UPDATE 26 January 2019: MC-12W Loss of Control Orbiting Over Afghanistan: Lessons in Training and Urgent Operational Requirements
UPDATE 28 March 2019: USAF T-38C Downed by Bird Strike
UPDATE 30 March 2019: Contaminated Oxygen on ‘Air Force One’ Poor standards at a Boeing maintenance facility, partially triggered by excessive workload and fatigue, resulted in contamination of two oxygen systems on a USAF Presidential VC-25 (B747).
UPDATE 14 December 2019: A “culture of safety” is lacking at the Massachusetts Bay Transportation Authority (MBTA) “according to a scathing report by three outside experts“.
UPDATE 4 October 2020: Investigators Suggest Cultural Indifference to Checklist Use a Factor in TAROM ATR42 Runway Excursion
UPDATE 25 April 2021: A Second from Disaster: RNoAF C-130J Near CFIT
UPDATE 5 June 2021: SAR AW101 Roll-Over: Entry Into Service Involved “Persistently Elevated and Confusing Operational Risk”
UPDATE 3 October 2021: French Cougar Crashed After Entering VRS When Coming into Hover
UPDATE 9 April 2022: SAR Seat Slip Smash (RCAF CH149 Leonardo Cormorant LOC-I)
UPDATE 14 May 2022: Review of “The impact of human factors on pilots’ safety behavior in offshore aviation – Brazil”
Recent Comments