Fixed Wing Accident & Incident Digest
There have been a number of interesting air accident reports or updates recently on a range of fixed wing accidents and incidents, each with unique lessons.
1) Loss of propeller control during descent causes fatal DHC-8 forced landing in Papua New Guinea
On 15 June 2014 the Papua New Guinea Accident Investigation Commission (AIC) released their final report into a fatal accident to Bombardier DHC-8-100 (aka Dash 8-100) P2-MCJ of Airlines PNG near Madang on 13 October 2011. The AIC concluded that both propellers oversped during descent after having been put incorrectly into beta range. A forced landing occurred on sparsely timbered terrain. Twenty eight passengers died but the Australian and New Zealand pilots, a cabin crew member and one passenger survived the accident.
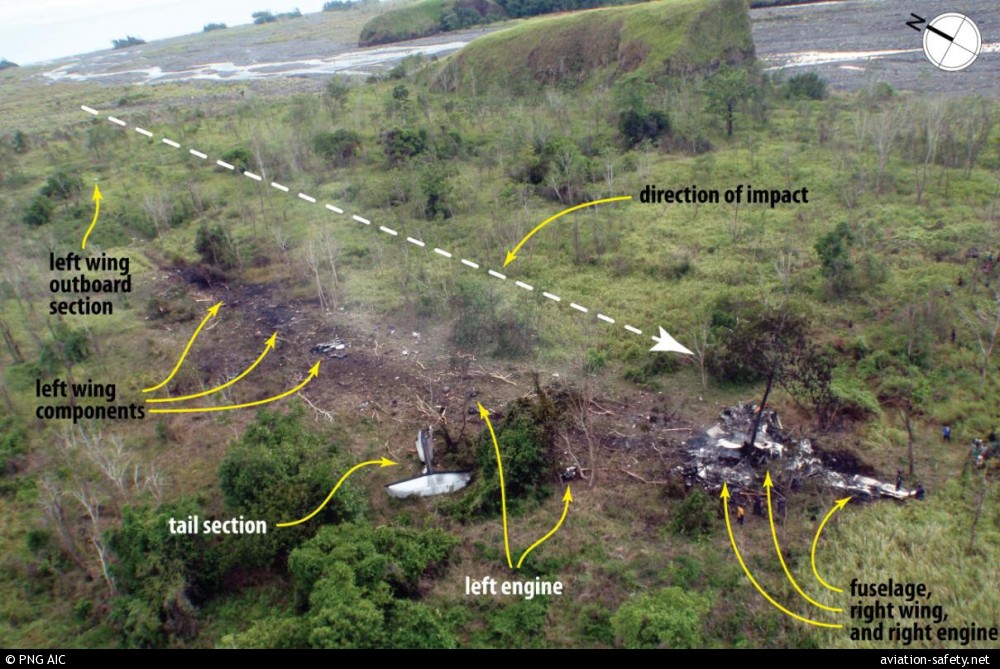
The pilot-in-command (PIC) conducted a low power, steep descent with the propellers set at 900 revolutions per minute (RPM) in an attempt to get below cloud. Neither pilot noticed that the airspeed increase to the aircraft’s maximum operating speed (VMO). At that point a warning sounded in the cockpit and the PIC pulled the power levers backwards, through the flight idle gate and into the ground beta range.
Moments later, at 10,090 feet, both propellers oversped simultaneously, back-driving the engines, causing damage to both engines, so a forced landing without power became inevitable. The landing gear and flaps were not lowered, if they had been the impact could have been less severe. The AIC stated:
…the aircraft’s degraded controllability and the high rate of descent/short time to impact were at least partly attributable to the fact that the flight crew did not use the standard emergency procedures early on. While it is not possible to determine exactly what would have happened if the flight crew had had more time to deal with the situation, it is reasonable to suppose it may have positively affected their ability to assess and manage the situation in a systematic manner.
The AIC identified the following contributing safety factors:
- The Pilot-in-Command moved the power levers rearwards below the flight idle gate shortly after the VMO overspeed warning sounded. This means that the release triggers were lifted during the throttle movement.
- The power levers were moved further behind the flight idle gate leading to ground beta operation in flight, loss of propeller speed control, double propeller overspeed, and loss of usable forward thrust, necessitating an off-field landing.
- A significant number of DHC-8-100, -200, and -300 series aircraft worldwide did not have a means of preventing movement of the power levers below the flight idle gate in flight, or a means to prevent such movement resulting in a loss of propeller speed control.
If a beta lockout mechanism had been installed on the aircraft, the double propeller overspeed would not have occurred when the power levers were moved below the flight idle range and into the ground beta range during flight. The Civil Aviation Safety Authority of Papua New Guinea issued their own Airworthiness Directive shortly after the accident. Installation of the beta lockout mechanism became a mandatory requirement of the State of Design following the issue of a Transport Canada Airworthiness Directive (Bombardier is a Canadian manufacturer) in 2013. They had however been required on DHC-8s in the US since 2000 following National Transportation Safety Board recommendations after an 1994 SF340 accident.
However, if you charter DHC-8-100, -200, and -300 series aircraft you should however be aware that compliance is requited within 6,000 flying hours or 3 years of the effective date of the AD (17 December 2013) and that the State of Design Airworthiness Directive’s are not automatically adopted in all countries.
After an incident on another aircraft in 2013, the US repair station that overhauled the propeller control unit (PCU) installed, identified a quality failure, namely the use of incorrect reassembly procedures for the installation of the beta switch within the PCU. That defect could lead to uncommanded propeller feathering and a recall was instituted.
The AIC report notes that:
On 28 October 2011, with the approval of CASA PNG, the operator re-commenced DHC-8 services on a reduced schedule for the first three weeks to minimise stress on the organisation. An operational return-to-service risk assessment was undertaken to ensure that all risks were identified and treated prior to restarting regular passenger transport (RPT) operations on the DHC-8 fleet.
As Airline PNG point out in their press release:
In the majority of aircraft accidents over the years, there have been multiple contributing factors. The AIC Report clearly points to the fact that the forced landing near Madang was no exception – with human factors, “a systemic design issue” and other factors all combining to cause this tragic event.
For more details on this accident see Aviation Herald or Aviation Safety Network.
Australian press coverage of the release of the accident report is here.
An interview with the airline’s General Manager of Safety is here and one with the Head of the AIC here.
2) ATR-72 descends below glideslope in IMC
On 12 June 2014 the Irish Air Accident Investigation Unit (AAIU) reported on a serious incident to an ATR-72. On 19 December 2011, an ATR-72 of Aer Arann was being operated from Dublin to Kerry in Ireland with a flight crew of a training captain (commander) and a captain, who was being line checked by the commander.While the aircraft was conducting an Instrument Landing System (ILS) approach with the autopilot engaged, difficulty was experienced in following the glideslope and the aircraft descended below the glide path. As the aircraft passed over a ridge on the approach the Enhanced Ground Proximity Warning System (EGPWS) activated and a go-around was initiated. Following this, a non-precision approach was flown which resulted in a successful landing. During that approach similar problems with the glideslope were experienced.
Subsequent examination by the Operator found that the unstable reception of the ILS glideslope signal was caused by a missing reflective strip from the inside of the aircraft’s radome which had been recently repaired.
3) Jetstream 32 control problems caused by too low RPM on takeoff
On 9 June 2014, the Statens Haverikommission (SHK), the Swedish Accident Investigation Authority, published their report on a 3 May 2013 incident involving J32 ES-PJR operated by Estonia operator AS Avies.

ES-PJR (Credit: Avies)
Shortly after take off, at about 500 feet, substantial fluctuations in power (torque) and engine speed (RPM) occurred on both engines. Data from the Flight Data Recorder and from analysis of a private video indicate the engine RPM was too low. It was a known problem that a start with a too low RPM in some cases could cause engine problems on the J31/J32. There had been a accident in the US in 1987 in which a too low RPM setting was identified as the root cause.
SHK reported that:
The operational documentation of the operator did not contain a requisite level of information on potential risks when starting with too low RPM. The aircraft type has no warning system to identify a faulty engine configuration and the checklist does not contain a “memory item” procedure for immediate action by the crew.
The circuit breaker was not pulled on the CVR so data from the incident was over written. The operator did not have the conversion data for the FDR, hampering the investigation. SHK found corrosion and ‘temporary’ repairs. SHK also identified a number of irregularities with the aircraft’s technical records, including defects not recorded in the Technical Log but in separate ‘Maintenance Requests’.
Three recommendations were made to EASA:
-
Investigate the conditions for installation of a warning system on the aircraft type in question which notifies the pilots of an incorrect engine configuration in connection with take-off. (RL 2014:07 R1)
- Endeavour to revise the emergency checklist for this aircraft type so that measures in the event of engine oscillations in connection with take-off are changed so as to be included as “memory items”. (RL 2014:07 R2)
- Take measures to ensure that initial and recurrent training on this aircraft type are supplemented with information and training regarding the risks of incorrect engine configurations during take-off. (RL 2014:07 R3)
4) Short-circuit likely caused Emergency Location Transmitter (ELT) battery fire on Boeing 787-8 at London Heathrow
The UK Air Accidents Investigation Branch (AAIB) published a Special Bulletin on 18 June 2014 containing information on the progress of the investigation into a ground fire on an unoccupied Boeing 787-8, registration ET-AOP of Ethiopian Airlines, at London Heathrow on 12 July 2013. Examination of the aircraft’s Honeywell ELT revealed that the internal battery pack exhibited evidence consistent with having experienced a thermal runaway. All five cell cases had been breached and burnt battery material had been ejected into the battery compartment and outside of the ELT case.
The AAIB reports that the most probable cause of the thermal runaway was a short-circuit caused by improperly installed battery wires, leading to an uncontrolled discharge of the battery. The wiring issue had been identified by the manufacturer, who had change production procedures, but had not take action with regard to the in-service fleet.
It was established that this condition in isolation should not have caused a battery thermal event, if the battery short-circuit protection features had effectively limited the current to a safe level. In addition, the failure sequence would have required one of the battery cells to deplete more rapidly than the others until it reversed polarity, becoming resistive and absorbing energy from the other four cells as they discharged and ultimately resulting in thermal runaway of the depleted cell. Several tests demonstrated that when a cell failed in this manner, the heat released caused the failure to cascade to the remaining four cells.
AAIB discuss the certification requirements and standards in detail.
Five safety recommendations were issued:
- It is recommended that the Federal Aviation Administration develop enhanced certification requirements for the use of lithium-metal batteries in aviation equipment, to take account of current industry knowledge on the design, operational characteristics and failure modes of lithium-metal batteries.
- It is recommended that the Federal Aviation Administration require that electrical performance and design-abuse certification tests for lithium-metal batteries are conducted with the battery installed in the parent equipment, to take account of battery thermal performance.
- It is recommended that the Federal Aviation Administration work with industry to determine the best methods to force a lithium-metal cell into thermal runaway and develop design-abuse testing that subjects a single cell within a lithium-metal battery to thermal runaway in order to demonstrate the worst possible effects during certification testing.
- It is recommended that the Federal Aviation Administration require equipment manufacturers wishing to use lithium-metal batteries to demonstrate (using the design-abuse testing described in Safety Recommendation 2014-022) that the battery and equipment design mitigates all hazardous effects of propagation of a single-cell thermal runaway to other cells and the release of electrolyte, fire or explosive debris.
- It is recommended that the Federal Aviation Administration review whether the Technical Standard Order (TSO) process is the most effective means for the certification of lithium-metal batteries installed in aircraft equipment, the actual performance of which can only be verified when demonstrated in the parent equipment and the aircraft installation.
5) A330 Voyager loss of control due to loose article
On 9 February 2014 a Royal Air Force (RAF) A330 Voyager ZZ333, was involved in an incident during a flight from Afghanistan. Voyager is the UK military name for converted Airbus A330’s operated as Military Registered Civil Owned Aircraft. The aircraft are owned and maintained by AirTanker, and operate from RAF Brize Norton.

RAF Voyager (Credit: Air Tanker)
During the incident the aircraft suddenly pitched nose down while in the cruise at 33,000ft. Within 27 seconds, the aircraft lost 4,400ft, with a maximum rate-of-descent of approximately 15,000ft per minute, before recovering. The resulting negative g forces were sufficient for almost all of the unrestrained passengers and crew to be thrown towards the ceiling, resulting in a number of minor injuries. The aircraft diverted to Incirlik in Turkey.
The UK Military Aviation Authority (MAA) issued a preliminary report on 17 March 2014 (an encouraging development as this is the first time they have every issued such a report). It explained that the investigation:
…found evidence to link the movement of the seat to the movement of the side-stick, in the form of a Digital SLR camera obstruction which was in-front of the Captain’s left arm rest and behind the base of the Captain’s side-stick at the time of the event. Analysis of the camera has confirmed that it was being used in the three minutes leading up to the event. Furthermore, forensic analysis of damage to the body of the camera indicates that it experienced a significant compression against the base of the side-stick, consistent with having been jammed between the arm rest and the side-stick unit. Crew interviews have corroborated this evidence. As such, the Inquiry has confidence that the pitch-down command was the result of an inadvertent physical input to the Captain’s side-stick by means of a physical obstruction (the camera) between the arm-rest and the side-stick unit. Simulations have been carried out which have re-created the scenario which has shown that it is possible for objects to become inadvertently lodged in the space between the arm rest and the side-stick, generating an identical pitch-down command to that seen during the incident.
It is noteworthy that the Captain was the only person on the flight deck at the time. No doubt the investigation will examine in-flight procedures after the introduction of the two crew A330 that replaced previous VC10s that had 4 crew flight deck and Tristars that had 3 flight deck crew.
UPDATE 23 March 2015: The full SI report has been published.
6) ATR-72 operated 13 flights with tail damage
On 10 June 2014 the Australian Transport Safety Bureau (ATSB) published a preliminary report into a serious incident with a Virgin Australia Regional Airlines (VARA formerly Perth, WA based SkyWest) ATR72, registered VH-FVR .

VH-FVR arriving on stand 20 Feb 2014 (Credit: Sydney Airport)
During a flight on 20 February 2014 the crew noticed airspeed increase. While dealing with this, the crew suddenly felt high positive g (sufficient to result in injury in the cabin), the controls felt different and spongy, and cockpit warnings activated. The crew regained control and the aircraft landed safely at Sydney. The incident was initially considered to be turbulence related. Maintenance checks were conducted overnight and no defects identified.
Subsequently, on 25 February 2014, after a further 13 sectors, the aircraft suffered what the crew initially believed was a bird strike after the pitch trim system fluctuated abnormally after landing, following an approach in close proximity to birds. Subsequent inspections did not identify any bird debris but did discover various damage where the horizontal stabiliser attaches to the vertical stabiliser and some minor damage to the rudder. The damage was consistent with an overstress condition. Subject to further assessment and non-destructive testing (NDT), ATR recommended replacement of the horizontal stabiliser, elevators, and vertical stabiliser.
The operator identified that the two incidents may be linked. The ATSB report that on initial examination of data from the 20 February flight:
…the recorded data showed that when the airspeed approached 240kt, at about 8,500ft during the descent into Sydney on 20 February, the first officer used touch control steering and manually pitched the aircraft up. The airspeed increased again and then both the first officer and captain pulled on the control column. Shortly after, when the vertical load factor was increasing through 1.8 g, the first officer began to push the control column. The differential force on the control column that resulted from the captain and first officer applying an opposing force exceeded the differential force required to generate a pitch disconnect. Each pilot was then controlling the elevator on their side of the aircraft in opposite directions for a brief period before the first officer released his control column.

Tailplane external damage indicated by marks and stickers (Credit: ATSB)
The ATSB investigation is still underway, but undoubtedly will examine the circumstances of the maintenance inspection on 20 February.
It is noticeable that to deal with two different unscheduled inspections that day the two ‘duty engineers’ started at 0600 and finished at 2200 (a 16 hour day each) and the ‘off-duty’ engineer came in during a rest period, worked from 1900 to 2300 (4 hours) before returning the next morning at 0600 (after a break of just 7 hours).
While it is not possible to draw any conclusions on whether fatigue was a factor in this incident, the rostering practices of this maintenance organisation do deserve closer attention. For details on managing maintenance fatigue see this Australian Civil Aviation Safety Agency (CASA) guidance. This includes material from a UK Civil Aviation Authority (CAA) report (CAA Paper 2002/06) on Work Hours of Aircraft Maintenance Personnel based by Dr Simon Folkard of the Department of Psychology, University of Wales. That report recommended:
- No scheduled shift should exceed 12 hours.
- No shift should be extended beyond a total of 13 hours by overtime.
- A minimum rest period of 11 hours should be allowed between the end of shift and the beginning of the next, and this should not be compromised by overtime.
The ATSB report that the on-going investigation will include review of the:
- meteorological data
- data from the flight data recorder
- data from the cockpit voice recorder
- closed circuit TV footage
- aircraft operator’s procedures and training
- aircraft maintenance records
- maintenance organisation’s procedures and equipment
- arrangements between the aircraft operator and maintenance organisation
- aircraft manufacturer’s maintenance instructions
- information as it becomes available during the repair process.
For more details on this incident see Aviation Herald or Aviation Safety Network.
Recent Comments