Wreckage of AS332L2 Super Puma G-WNSB in the Water off Sumburgh (Credit: RNLI)
The CHC helicopter, chartered by Total, was making a 3 sector flight to Aberdeen from the Alwyn North installation in the East Shetland Basin, via the Borgsten Dolphin drilling rig and Sumburgh (for a refuelling stop, following a relatively late manifest change to add an extra passenger on the return flight).
AS332L2 Super Puma G-WNSB Route – Accident Sector in Red (Credit: AAIB)
The G-WNSB Aircraft Commander was an experienced Super Puma pilot who had approximately 15 years experience on the L1 Super Puma [sic] and 3 years experience (1894 flying hours) on the L2 Super Puma. The Co-Pilot had been a flying instructor on single engine, single pilot aircraft at a different company with approximately 3000 flying hours but was new to Super Puma operations. He had been with the company for only a year, initially training on 225 Super Puma but then retrained onto the L2 Super Puma, qualifying in February 2013. The Co-Pilot had approximately 400 flying hours on the L2 Super Puma.
The Accident Flight
Meteorological data for Sumburgh at the time indicated broken cloud at 300ft, with 2,800m visibility. The AAIB say:
The commander was the Pilot Flying (PF) on the accident sector. The weather conditions were such that the final approach to Runway 09 at Sumburgh Airport was flown in cloud, requiring the approach to be made by sole reference to the helicopter’s instruments, in accordance with the Standard Operating Procedure (SOP) set out in the operator’s Operating Manual (OM).
The approach was flown with the autopilot in 3-axes with Vertical Speed (V/S) mode, which required the commander to operate the collective pitch control manually to control the helicopter’s airspeed. The co-pilot was responsible for monitoring the helicopter’s vertical flightpath against the published approach vertical profile and for seeking the external visual references necessary to continue with the approach and landing.
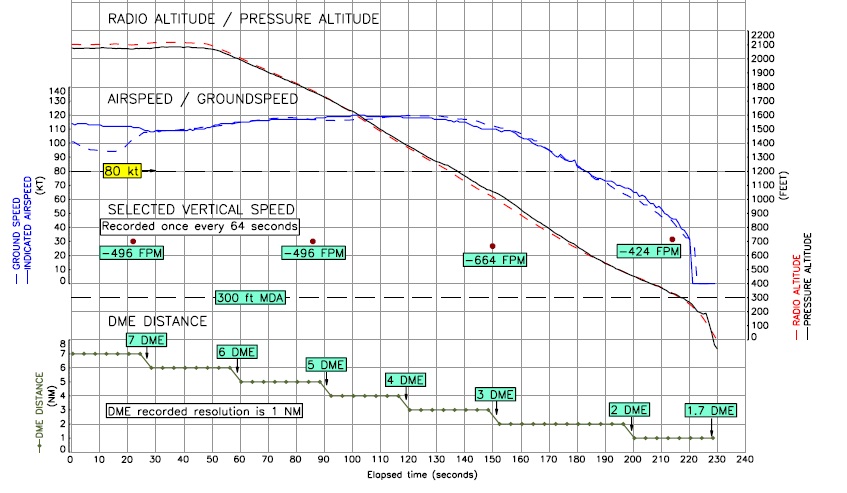
The procedures permitted the helicopter to descend to a height of 300 ft, the Minimum Descent Altitude (MDA) for the approach, at which point a level-off was required if visual references had not yet been acquired. Although the approach vertical profile was maintained initially, insufficient collective pitch control input was applied by the commander to maintain the approach profile and the target approach airspeed of 80 kt. This resulted in insufficient engine power being provided and the helicopter’s airspeed reduced continuously during the final approach.
Control of the flightpath was lost and the helicopter continued to descend below the MDA. During the latter stages of the approach the helicopter’s airspeed had decreased below 35 kt and a high rate of descent [up to 1,800 fpm] had developed.
AS332L2 Super Puma G-WNSB FDR Extract (Credit: AAIB)
The decreasing airspeed went unnoticed by the pilots until a very late stage, when the helicopter was in a critically low energy state.
The AAIB characterise this as “consistent with entry into a Vortex Ring State, making recovery difficult, if not impossible, in the height available”. This reduced the available lift by ~30-45% in the final 8s before impact according to calculations by Airbus Helicopters.
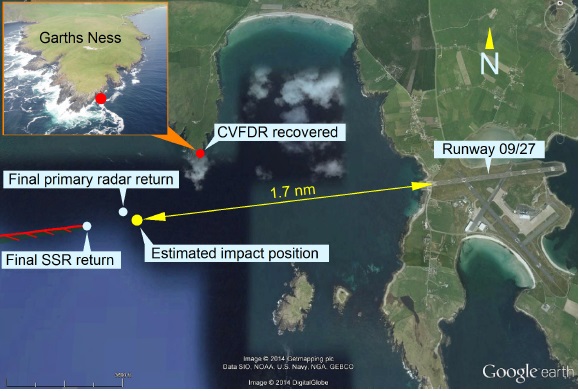
The commander’s attempt to recover the situation was unsuccessful and the helicopter struck the surface of the sea approximately 1.7 nm west of Sumburgh Airport.
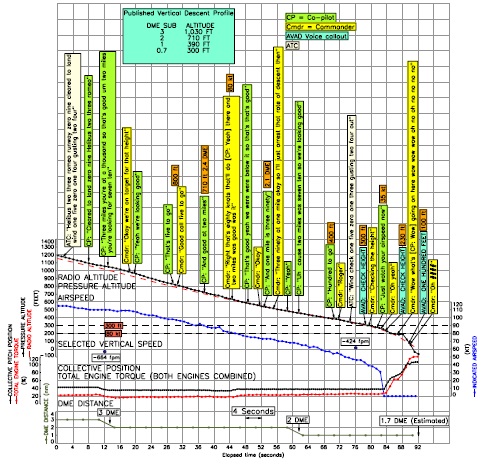
AS332L2 Super Puma G-WNSB CVR Summary (Credit: AAIB)
The Impact, Survival and Rescue
The emergency flotation system had been armed by the co-pilot in the last few moments before the impact. The tail boom separated during the impact but the Crash Position Indicator (CPI) Automatically Deployable Emergency Locator Transmitter (ADELT) did deploy and transmit. At the time of the accident emergency calls by air traffic were routed
through a Police Scotland Command and Control Centre, which created a short delay.
AS332L2 Super Puma G-WNSB Impact Location West of Sumburgh (Credit: AAIB)
The sea state was reported as ‘slight to moderate’ by rescuers (i.e between Sea State 3 and 4). The water temperature was 13°C, sufficiently low for ‘cold shock’ to occur. The crew were not able to warn the passengers before impact but some did adopt the brace position.
Following impact with the water, the helicopter rolled [to the left] upside down and rapidly filled with water but remained afloat, inverted on the surface, supported by the floats which had inflated automatically.
Twelve passengers and two crew members escaped from the helicopter and survived the accident.
There were four fatalities: two passengers did not escape from the upturned fuselage, one passenger was found by the coastguard helicopter, lifeless, floating on the surface and one passenger, who had successfully escaped, subsequently died in one of the liferafts.
This is the first public confirmation of how the four fatalities occurred, only two within the cabin. The AAIB provide greater detail:
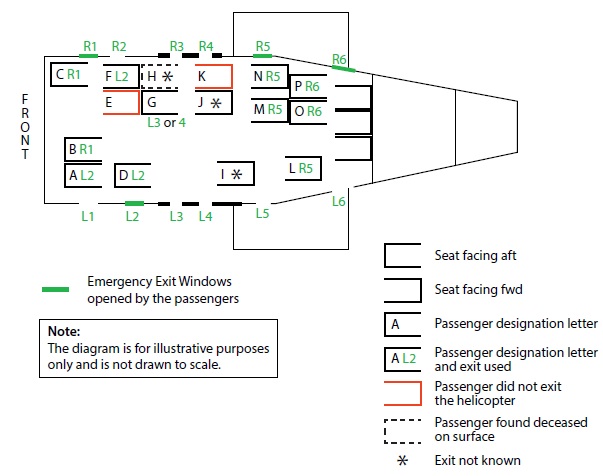
As332L2 G-WNSB Seating Positions: Note the Aircraft Rolled to the Left and Became Inverted After Impact (Credit: AAIB)
Passenger K was recovered from the passenger cabin, still secured in their seat. The post-mortem report indicates that a head injury was sustained, which seemed likely to have rendered the passenger unconscious….Other pathological evidence was consistent with drowning; the seat harness had not been released, most likely as a result of the head injury.
Passenger H was recovered from the sea. The pathological evidence was consistent with drowning. There were other injuries, which included a head injury, but none were particularly severe. Given that this passenger appears to have released their harness, escaped from the helicopter and inflated their life jacket, it seems unlikely that the head injury had an incapacitating effect.
Passenger E’s body was recovered from the water after the fuselage of the helicopter had broken open due to the wave action and contact with the shore. Evidence from the Emergency Breathing System (EBS) indicates that the mouthpiece had been removed from the pouch and the valve opened in an apparent attempt to use the device. Whilst there were some minor injuries, the evidence showed that the passenger had drowned whilst still in the cabin of the helicopter.
Passenger I was able to escape from the helicopter and was assisted by other survivors onto the inverted fuselage of the helicopter and then into the liferaft. Whilst in the liferaft, the passenger was seen to be showing symptoms of chest pain and then apparently stopped breathing. …cardiopulmonary resuscitation (CPR) [was attempted], but this was unsuccessful. The post-mortem identified evidence of significant pre-existing heart disease which, from the witness accounts and the absence of serious injuries, indicate that the passenger had died of heart disease.
The Commander and one surviving passenger suffered spinal fractures during the crash.
Few of the occupants had been able to take a breath before becoming submerged due to the rate of water ingress and most had difficultly with poor visibility underwater. A passengers few tried to use their passenger EBS (a LAP Plus (LAPP) jacket, hybrid rebreather) but were unable to locate the mouthpiece and “concentrated on escaping instead”.
Interviews with the survivors of this accident identified that they were unaware that the hybrid LAP Plus jacket had an automatically released air supply.
Only 4 of the 12 cabin push out windows appear to have been opened in the cabin (and so most of the 14 passengers who escaped [12 survivors and two who died post-egress] exited through these).
All passengers were equipped with survival suits. The crew has chosen to wear coveralls (as allowed by regulation) due to a comment from another crew of about fatigue from high temperatures on an earlier flight that day.
The Co-Pilot was able to activate the external life rafts using an optional, Heli-One designed, modification the operator had fitted to the aircraft when it was operating in Norway. These additional handles were not part of the passenger safety briefing (they were not standard on the UK fleet) and were only mentioned in the Flight Manual Supplement against the earlier Norwegian registration. The Co-Pilot was aware due to a prior informal crew room conversation. Ten people were able to board a raft (including Passenger I who died of a heart attack).
The survivors (9 from the life rafts and 5 in the water) were rescued by the HM Coastguard Sumburgh SAR helicopter, supported by a second oil and gas industry SAR helicopter based at that time at Sumburgh. The first helicopter was on scene in 23 minutes of the impact, just 13 minutes from their notification.
Overall, the pattern and magnitude of injuries to the occupants was consistent with a relatively low speed impact with water.
AS332L2 Super Puma G-WNSB Wreckage the Next Day (Credit: AAIB)
Analysis of the Approach
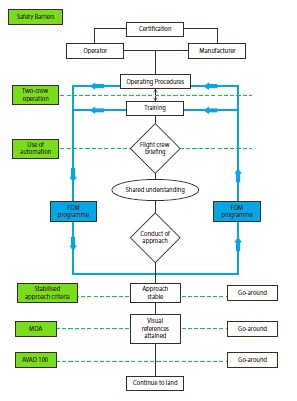
The AAIB describe a number of safety barriers associated with an approach.
Safety Barriers: Operational in Green (Credit: AAIB)
The AAIB discuss the operational controls in more detail:
Two Crew Operation
…in hindsight, the operator’s SOPs for Non-Precision Approaches were not sufficiently well defined, allowing crews to fly such an approach in a number of different ways. The pilots of G-WNSB therefore did not arrive at the same, unambiguous understanding of how the approach was to be flown. The operator has since taken safety action to amend the applicable SOPs to make them more prescriptive and less ambiguous.
The pilots did not adhere to the specified phraseology, with the result that it was more difficult for the co-pilot to challenge events.
There was both an experience and an authority gradient between the two pilots, as evidenced on a number of occasions when the co-pilot asked the commander for information or advice, and in his acceptance of the commander’s ambiguous comments during the approach briefing. It was apparent from the CVR and interviews with the co-pilot that he tended to defer to the commander’s decisions, rather than questioning them. The co-pilot himself suggested that this may have been because of the commander’s greater experience.
This safety barrier of two-crew operation was, for these reasons, rendered ineffective.
AAIB also say:
During the latter stages of the approach the co-pilot’s workload was high, which may have affected his ability to monitor effectively.
Automation Modes of the Helicopter
As there is currently no requirement for helicopter manufacturers to set out operational guidance on using aircraft systems or for operators to identify the preferred autopilot selections …
…the operator’s SOPs allowed Non-Precision Approaches to be flown in either 3-axes or 4-axes modes. Data showed that the use of 3-axes with V/S for onshore approaches was more prevalent amongst the operator’s pilots.
Use of the 4-axes mode for the approach would have reduced the commander’s workload, by relieving him of the task of operating the collective pitch lever, and the autopilot would have maintained the selected airspeed during the approach.
Engaging the 4-axes mode is likely to have prevented this accident.
[As] use of automation was not optimised and this safety barrier was ineffective. Following the accident, the operator took a safety action to amend its SOPs for Non-Precision Approaches, requiring them to be flown exclusively with 4-axes coupled, and at a specific, pre-briefed, and nominated fixed airspeed
Stabilised Approach Criteria
The defined stabilised approach criteria were satisfied.
Minimum Descent Altitude with Automated Callouts
The automated callout at the MDA is to ensure that the approach minima are not overlooked at a time when the workload may be high and other distractions may be present.
For this approach, the crew had four options on reaching the MAP but the options were not specified during the commander’s approach briefing, thereby creating uncertainty. The automated ‘check height’ callout activated, but the commander’s actions did not result in the helicopter levelling off as required. This safety barrier was therefore breached.
Automated 100 foot Callout (non-cancellable AVAD)
In this accident the alert came only moments before impact and, given the helicopter’s high rate of descent, it was too late to be effective.
Additionally
Additionally AAIB say:
The evidence suggests that the commander may have retained an expectation of being able to see the runway during the latter stages of the approach and did not adjust his mental model to allow for a possible level-off at MDA, or flying a go-around.
There was no evidence in the historic FDM data reviewed that the commander had ever continued with an approach to land in weather conditions below minima; his previous 29 approaches to Sumburgh Airport had all transitioned to manual flight at altitudes above 500 ft aal. No FDM events were found that indicated that the commander had flown at low airspeed during an approach.
The two human performance studies [commissioned by AAIB – Appendix H and I] utilised different methodologies, but reached similar conclusions… Both reports identified that a decay in airspeed and associated low total energy state of the helicopter were not observed by the crew until it was too late. Neither study was able to determine, with any certainty, why this situation arose and was not detected, although various possibilities were discussed.
The second study, by the RAF Centre for Aviation Medicine (RAFCAM) in particular highlighted that there were systemic human factors that could have affected other crew’s performance.
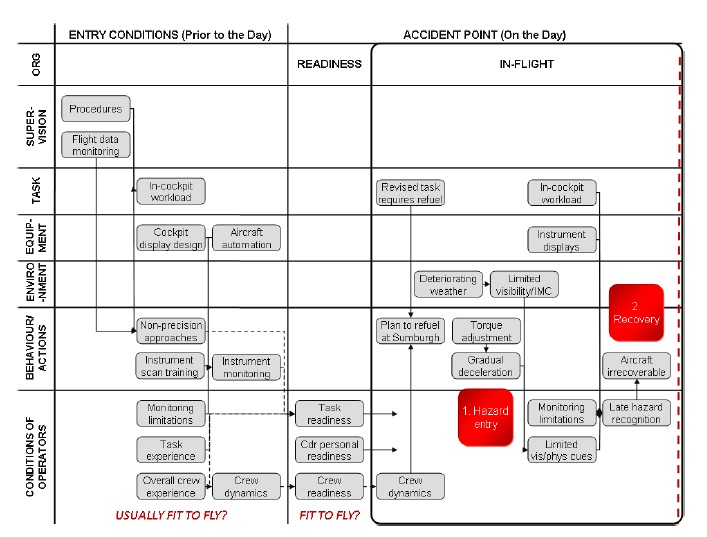
Accident Route Matrix (ARM) for Super Puma AS332L2 G-WNSB (Credit: RAFCAM via AAIB)
RAFCAM also comment:
During the vertical descent profile between 45 and 10 seconds prior to impact there were limited physiological and visual cues to enable the crew to judge the aircraft position and flight profile.
In addition, the combination of deceleration and pitch could have contributed to a somatogravic illusion which led the crew to perceive that they were flying straight and level and at a constant speed.
The AAIB do note that:
Several research projects have been undertaken which have identified a need for revised training in pilot instrument scan techniques. The new research initiated by HeliOffshore using eye-tracking tools and LOSA observations should provide valuable new data.
AAIB note that Flight Data Monitoring (FDM) is a “fundamental tools for ensuring compliance with SOPs” as a “a closed-loop monitoring system”. They acknowledge that the UK CAA facilitated the introduction of Helicopter FDM (HFDM) with their initial research and that the operator’s have voluntarily implemented HFDM. they go on to say though that “having acknowledged the difficulties of HFDM”, given the complexities of offshore helicopter operations, its on-going development was then predominantly left to the operators” where there have been active CAA and EASA forum for airline FDM development.
The importance of work enhancing the waning time that can be provided by Helicopter Terrain Awareness Warning Systems (HTAWS) is also noted.
AAIB Conclusions
The AAIB identified two causal factors:
The helicopter’s flight instruments were not monitored effectively during the latter stages of the non-precision instrument approach. This allowed the helicopter to enter a critically low energy state, from which recovery was not possible.
Visual references had not been acquired by the Minimum Descent Altitude (MDA) and no effective action was taken to level the helicopter, as required by the operator’s procedure for an instrument approach.
They identified four contributory factors:
The operator’s SOP for this type of approach was not clearly defined and the pilots had not developed a shared, unambiguous understanding of how the approach was to be flown.
The operator’s SOPs at the time did not optimise the use of the helicopter’s automated systems during a Non-Precision Approach.
The decision to fly a 3-axes with V/S mode, decelerating approach in marginal weather conditions did not make optimum use of the helicopter’s automated systems and required closer monitoring of the instruments by the crew.
Despite the poorer than forecast weather conditions at Sumburgh Airport, the commander had not altered his expectation of being able to land from a Non-Precision Approach.
The AAIB note they found similarities between this accident and previous accidents resulting from ineffective monitoring of the flight instruments by the flight crew.
Safety Recommendations
The AAIB had previously issued safety recommendations in two of their three earlier Special Bulletins:
S7/2013 dated 18 Oct 2013 (covered an overview of the evidence gathered, including an FDR trace, plus a recommendation on airport sea rescue capability)
S1/2014 dated 23 Jan 2014 (contained a recommendation related to passenger briefing on emergency breathing systems)
In this final report they have issued further 26 recommendations (a number of which are perhaps disappointing prescriptive on specific solutions rather than focused on the desired safety outcomes and relate to other initiatives already underway by the European Aviation Safety Agency [EASA], HeliOffshore [and its members] and the Civil Aviation Authority [CAA]):
Safety Recommendation 2016-001: It is recommended that the European Aviation Safety Agency introduces a requirement for instrument rated pilots to receive initial and recurrent training in instrument scan techniques specific to the type of aircraft being operated.
Safety Recommendation 2016-002: It is recommended that the European Aviation Safety Agency reviews the existing research into pilot instrument scan techniques, particularly with respect to glass cockpit displays, with a view to addressing shortcomings identified in current instrument scan training methods.
Safety Recommendation 2016-003: It is recommended that the Civil Aviation Authority reviews the methods used by UK North Sea helicopter operators for confirming compliance with their Standard Operating Procedures (SOPs), to ensure they are effective.
Safety Recommendation 2016-004: It is recommended that the Civil Aviation Authority reviews the Standard Operating Procedures of helicopter operators supporting the UK offshore oil and gas industry, to ensure their procedures for conducting Non-Precision Approaches are sufficiently defined.
Safety Recommendation 2016-005: It is recommended that the European Aviation Safety Agency amends the Certification Specifications for Large Rotorcraft (CS 29) to align them with the Certification Specifications and Acceptable Means of Compliance for Large Aeroplanes (CS 25), with regard to the provision of operational information in Flight Manuals.
Safety Recommendation 2016-006: It is recommended that the European Aviation Safety Agency requires manufacturers of Large Rotorcraft to develop Flight Crew Operating Manuals for public transport types already in service.
Safety Recommendation 2016-007: It is recommended that the Civil Aviation Authority expedites the requirement for companies operating helicopters in support of the UK offshore oil and gas industry to establish a Helicopter Flight Data Monitoring (HFDM) programme.
Safety Recommendation 2016-011: It is recommended that the Civil Aviation Authority expedites the publication of the Helicopter Safety Research Management Committee report into improving [HTAWS] warning envelopes and alerts.
Safety Recommendation 2016-012: It is recommended that the Civil Aviation Authority supports the ongoing development of Helicopter Terrain Awareness Warning Systems, following the publication of the Helicopter Safety Research Management Committee report into improving warning envelopes and alerts.
Safety Recommendation 2016-013: It is recommended that the European Aviation Safety Agency requires the installation of Helicopter Terrain Awareness Warning Systems to all helicopters, used in offshore Commercial Air Transport operations, with a Maximum Certificated Take-off Mass (MCTOM) of more than 3,175 kg, or a Maximum Operational Passenger Seating Configuration (MOPSC) of more than nine, manufactured before 31 December 2018.
Safety Recommendation 2016-014: It is recommended that the European Aviation Safety Agency introduces a requirement for the installation of cockpit image recorders, in aircraft required to be equipped with Flight Data and Cockpit Voice Recorders, to capture flight crew actions within the cockpit environment.
Safety Recommendation 2016-015: It is recommended that the European Aviation Safety Agency introduces a requirement to install image recorders, capable of monitoring the cabin environment, in aircraft required to be equipped with Flight Data Recorder and Cockpit Voice Recorders.
Safety Recommendation 2016-016: It is recommended that the European Aviation Safety Agency instigates a research programme to provide realistic data to better support regulations relating to evacuation and survivability of occupants in commercial helicopters operating offshore. This programme should better quantify the characteristics of helicopter underwater evacuation and include conditions representative of actual offshore operations and passenger demographics.
Safety Recommendation 2016-017: It is recommended that, where technically feasible, the regulatory changes introduced by the European Aviation Safety Agency Rulemaking Task RMT.120 are applied retrospectively by the EASA to helicopters currently used in offshore operations.
Safety Recommendation 2016-018: It is recommended that the European Aviation Safety Agency amends the Certification Specifications for rotorcraft (CS 27 and 29) to require the installation of systems for the automatic arming and activation of flotation equipment. The amended requirements should also be applied retrospectively to helicopters currently used in offshore operations.
Safety Recommendation 2016-019: It is recommended that the European Aviation Safety Agency amends the Certification Specifications for Large Rotorcraft (CS 29), certified for offshore operation, to require the provision of a side-floating capability for a helicopter in the event of impact with water or capsize after ditching. This should also be applied retrospectively to helicopters currently used in offshore operations.
Safety Recommendation 2016-020: It is recommended that the European Aviation Safety Agency amends the Certification Specifications for Large Rotorcraft (CS 29), certified for offshore operation, to ensure that any approved cabin seating layouts are designed such that, in an emergency (assuming all the exits are available), each exit need only be used by a maximum of two passengers seated directly adjacent to it.
Safety Recommendation 2016-021: It is recommended that the European Aviation Safety Agency amends the Certification Specifications for Large Rotorcraft (CS 29), certified for commercial offshore operations, to include minimum size limitations for all removable exits, to allow for the successful egress of a 95th percentile-sized offshore worker wearing the maximum recommended level of survival clothing and equipment.
Safety Recommendation 2016-022: It is recommended that the European Aviation Safety Agency amends the Certification Specifications for Large Rotorcraft (CS 29), certified for use in commercial offshore operations, to require a common standard for emergency exit opening mechanisms, such that that the exit may be removed readily using one hand and in a continuous movement.
Safety Recommendation 2016-023: It is recommended that the European Aviation Safety Agency amends the operational requirements for commercial offshore helicopters to require the provision of compressed air emergency breathing systems for all passengers and crew.
Safety Recommendation 2016-024: It is recommended that the European Aviation Safety Agency (EASA) amends the operational requirements for commercial offshore helicopter operations, to require operators to demonstrate that all passengers and crew travelling offshore on their helicopters have undertaken helicopter underwater escape training at an approved training facility, to a minimum standard defined by the EASA.
Safety Recommendation 2016-025: It is recommended that the European Aviation Safety Agency amends the design requirements for helicopters to ensure that where liferafts are required to be fitted, they can be deployed readily from a fuselage floating in any attitude.
Safety Recommendation 2016-026: It is recommended that the European Aviation Safety Agency requires that, for existing helicopters used in offshore operations, a means of deploying each liferaft is available above the waterline, whether the helicopter is floating upright or inverted.
UPDATE 26 May 2016: UK CAA issues FACTOR F3/2016 that contains their update on progress on their actions. Five actions are marked ‘Open’ with target dates ranging from 30 Sept 2016 to 31 Dec 2017. One (2015-007), on expediting a requirement for FDM, is rejected.
UPDATE 13 August 2020: The AAIB have issued an addendum to their report as subsequent evidence shows that one passenger who died, who had been thought to have attempted to deploy their EBS, did not in fact do so.
Fatal Accident Inquiry
In Scotland a Fatal Accident Inquiry (FAI) is broadly equivalent to a coroners’ inquest but are only held fora death in the workplace or “in cases which give rise to reasonable suspicion” and are held before a Sheriff.
UPDATE 30 March 2020: Due to COVID-19 the FAI has been adjourned:
Although some court and tribunal business is currently being conducted via virtual links and in courtrooms adhering to social distancing, several factors make this unrealistic in this instance. This includes the large number of parties involved; the number of witnesses who are medical professionals required to deal with the Coronavirus pandemic; and the high degree of media and public interest.
Sheriff Pyle agreed to go ahead with this course of action given that “technical issues may arise” during “the first large inquiry in Scotland ever to be done in this way”. Sheriff Pyle instructed a final preliminary hearing to be held on August 24 to ensure all parties…were prepared to begin the following week.
UPDATE 25 August 2020: The FAI will start next week as case INV B29-20, with the AAIB as the first witnesses. The virtual technology was been tested on 24 August 2020.
UPDATE 31 August 2020:Virtual FAI access details. On Day 1 an agreed summary of the accident was read, the Deputy Chief Inspector of Air Accidents gave evidence and the inquiry heard a written statement and saw video evidence from the aircraft commander.
UPDATE 1 September 2020: On Day 2 the FAI heard evidence for passengers. In relation to HUET one passenger said: “It saved my life on that day.” Another suggested that the standard for practical survival training had deteriorated over the years, although there may have been confusion between initial and recurrent training. It also emerged that one passenger had committed suicide in 2017 after a battle with PTSD.
UPDATE 2 September 2020:On Day 3 the FAI further passenger evidence was heard as well as evidence from Professor James Grieve, who carried out post-mortem examinations on the four who died in the crash:
1 had severe heart disease and was showing classic indications of severe heart problems during their time offshore and likely suffered heart failure shortly after egress, due to the stress and exertion
1 had a head injury that may well have proved fatal even if the aircraft had not capsized
1 drowned but was probably unconscious due to a moderate head injury
1 drowned (although they did have mild head injuries)
UPDATE 3 September 2020:On Day 4 of the FAI evidence was given by AAIB engineering and flight data inspectors.
UPDATE 14 September 2020: On Day 11 UK CAA’s Rick Newson was the final witness. Parties now have just over a week to provide final written submissions prior to the last oral session on Friday 25 September 2020.
In his closing submission at a fatal accident inquiry, Martin Richardson for the Crown said the helicopter failed to maintain its target approach speed…and that failure arose because the flight instruments were not effectively monitored by the flight crew.
The inquiry has now concluded. Derek Pyle, sheriff principal of Grampian, Highland and Islands, said he would make his determination in no more than four weeks. Mr Richardson said the Crown wished to apologise for the “very very long time” it had taken for the fatal accident inquiry to be held.
Highlands, Islands and Grampian Sheriff Principal Derek Pyle, who has been conducting the inquiry virtually because of Covid restrictions on courts, said he will considering the actions of the pilot, …and co-pilot…in his findings, but added “both should be commended” for their actions following the crash, in particular [the co-pilot] who activated the flotation devices [i.e. the EFS using an external belly handle only fitted to ex-Norweigian aircraft] and liferaft. He said he would also be “mentioning in some detail” the experience of the passengers following the accident “and what they went through when they were swimming around in the sea”.
Finally, the sheriff principal said: “I will certainly be asking the question, how safe are helicopters genuinely in the North Sea?”
UPDATE 19 October 2020: The Sheriff Principal issued his determination. This included:
The flight crew of the helicopter failed to maintain the target approach airspeed and the stabilised approach criteria contained in the operator’s operations manual during the latter stages of the non-precision approach to Sumburgh Airport. This was due to the flight crew not effectively monitoring the helicopter’s flight instruments, thereby allowing the helicopter to enter a critically low energy state resulting in the loss of control of the aircraft.
And the conclusion:
This was a dreadful accident with long term repercussions for the survivors and the families of the deceased which no determination by this court can properly describe. I do hope that it has at least assisted in an understanding of what occurred, the reasons for it and what has been done to ensure so far as practicable that such an accident does not occur again. My condolences go, in particular, to the families of the deceased, including – lest it be forgotten – the family of Mr Bull.
The considerable delay in holding the FAI is partly explain by an inability of the UK CAA to provide expert support, a role finally filled by Mark Prior.
A hurried UK CAA Review of North Sea helicopter safety, which resulted in the CAP1145 report (‘Safety review of offshore public transport helicopter operations in support of the exploitation of oil and gas’).
We have received the AAIB‘s final report into the tragic accident at Sumburgh in 2013 and will be considering it carefully… The safety of those who rely on offshore helicopter flights is one of our top priorities and we will continue to work with the helicopter operators, the offshore industries, international regulators, unions and pilot representatives to enhance offshore safety standards still further.
The Sumburgh incident was a tragedy for all those involved.
Many safety improvements have already been made to helicopter operations since this tragic accident but pilots and safety experts will be examining the report to identify what more can be done to avoid a repeat.
The challenge will be to drive up industry-wide standards at a time when the drive to reduce contract prices puts those standards under pressure.
While some early press reports took the rather dated, cliqued and myopically unhelpful approach of labelling this accident as ’caused’ by ‘pilot error’ it is refreshing to see one survivor more reflectively state:
I don’t have anything against the pilots. We’re only human.
Extra Resources
We have previously written a number of relevant articles:
Previous studies on and accident investigations into helicopter ditchings and water impact events have highlighted inadequacies in the existing certification specifications (CS-27, CS-29) and in the rules governing offshore operations. In particular, it has been established that in an otherwise survivable water impact, most fatalities occurred as a result of drowning because the occupants were unable either to rapidly escape from a capsized and flooded cabin, or to survive in the sea for sufficient time until rescue. Furthermore, the testing environment in which helicopters are type-certified for ditching bears little resemblance to the sea conditions experienced in operation.
In order to thoroughly address these and other ditching-related issues, and due to the nature of ditching-related hazards, this rulemaking task (RMT.0120 (27&29.008)) has taken a holistic approach to the problem, which crosses traditional airworthiness/operational boundaries. A detailed risk assessment has been undertaken that reflects both certification and operational experience and builds upon data extracted from accident reports and previous studies.
The specific objective of this NPA, however, is to propose changes to CS-27 and CS-29… Retroactive rules are to be considered in a second phase of this RMT.
…the primary change proposed aims to establish a new ditching certification methodology by which a target probability of capsize following a ditching can be determined based on the level of capsize mitigation applied to the design.
UPDATE 24 September 2016: The UKCAA has issued CAP1386, their second update on CAP1145. We have summarised that report.
Aerossurance is also pleased to sponsor the 2017 European Society of Air Safety Investigators (ESASI) 8th Regional Seminar in Ljubljana, Slovenia on 19 and 20 April 2017. Registration is just €100 per delegate. To register for the seminar please follow this link. ESASI is the European chapter of the International Society of Air Safety Investigators (ISASI).
Aerossurance has extensive proven offshore helicopter safety, SAR flight operations, airworthiness, survivability and accident analysis experience. For practical aviation advice you can trust, contact us at: enquiries@aerossurance.com