29 Seconds to Impact: A Fatal Night Offshore Approach in the Irish Sea (CHC Scotia AS365N G-BLUN)
At 18:00 on 27 December 2006 CHC Scotia Airbus AS365N G-BLUN departed Blackpool to conduct 8 sectors within the Morecambe Bay gas field in the Irish Sea. The first two were completed without incident but, when preparing to land on the North Morecambe platform, in the dark, the helicopter flew past the platform and struck the surface of the sea. There were no survivors amongst the five passengers and two crew.

The UK Air Accidents Investigation Branch (AAIB) issued their safety investigation report on 17 October 2008.
The Accident Flight
The flight crew had reported for duty at 12:00.
The aircraft commander had 8,856 hours total time, 6,156 on type and had been “operating in the Morecambe Bay gas field…for 20 years”. At the time of the accident he was simultaneously Blackpool Chief Pilot, a Line Training Captain and a Crew Resource Management (CRM) Instructor.
The co-pilot had 3,565 hours total time, 377 on type. This was his first offshore job, and had been employed by CHC Scotia for 13 months.
He had recorded a total of 467 hrs of night flying, however, he had recorded only 3 hrs of night flying in the previous three months.
Their recent experience included:

They had already completed one multi-sector flight that day. Their second flight was scheduled to depart at 18:00, with eight night sectors all to be flown with the co-pilot as the handling pilot.
G-BLUN was bult in 1985, had 20,469 hours and 130,038 cycles, indicating the nature of the operating environment with continual short sectors. AAIB explain that CHC Scotia’s AS365Ns were…
…fitted with Trimble 2101 Navigator Plus Global Positioning System (GPS), cleared as a primary means of navigation in instrument conditions. The fleet [were] also fitted with an Automatic Direction Finder (ADF) and a Sperry Primus 500 colour radar system. The GPS is the primary means of off-shore navigation, with the radar being used as a back up and to cross-check the GPS data when required.

After preparations….
The helicopter departed Blackpool at 1800 hrs and climbed to 1,000 ft on a westerly heading.
At 1,000 ft, and at an initial IAS of 135 kt, the autopilot altitude mode was engaged; it was disengaged at 1807 hrs and the altitude and speed started to reduce.
Given the average ground speed derived from the radar, and assuming that the GPS distances were accurate, the platform became visible at a range of approximately 4,400m: the windshield wipers were audible in the background.
No Automatic Voice Alert Device (AVAD) annunciations were recorded but the transition through the radio height of 100 ft occurred rapidly as the helicopter transitioned from being over the sea to over the helideck.

The helicopter landed on the AP1 platform at 18:11.
The next sector, to the Millom West platform, was flown without any passengers, baggage or freight and with 360 kg of fuel. The helicopter took off at 1814 hrs, climbed to 500 ft on a north-westerly heading and accelerated to an initial IAS of 145 kt.
The rig became visible 25 seconds after the 5 nm GPS call; this equates to a visual range of approximately 7,100 m. At 1820 hrs the helicopter initiated its descent whilst reducing speed and turned left onto a heading of 105ºM before landing on the Millom West at 1822 hrs.
During the final approach and landing the AVAD “ONE HUNDRED FEET” automatic annunciation was recorded, but no “CHECK HEIGHT” call was recorded
AAIB comment that:
The audio recordings suggest a relaxed atmosphere in the cockpit throughout the first two sectors and indicate that the normal checklists were being followed. The crew discussed the visual conditions and their experiences with similar conditions during their previous military flying.
The helicopter departed Millom West at 18:26 on the third and fatal sector having embarked 5 passengers.

The helicopter climbed to a height of approximately 500 ft on a heading of 120ºM and
accelerated to an initial IAS of 125 kt. The Automatic Flight Control System (AFCS) was engaged, with all channels ON in the Attitude Hold mode; this is the normal stabilisation mode for flight and is engaged prior to take off.Prior to becoming visual with the North Morecambe platform the commander was using the radar and the GPS to provide range information to the co-pilot.
Shortly after the 4 nm GPS call made by the commander, the crew became visual with the rig and the co-pilot said “I GOT THE DECK NOW”; allowing for the speed of the helicopter at the time, this equates to a visual range of about 6,800 m.
The commander then completed the before landing checks, which included arming the floats. Once they had established visual contact with the platform the commander provided no further range information.
Unlike the prior sectors the cockpit voice recorder (CVR) did not record the sound of the windscreen wipers being used on this sector.
Soon after becoming visual, the height reduced to 270 ft; the helicopter then climbed back to just over 400 ft before starting a further descent approximately 30 seconds later.
The installation still had legacy yellow perimeter lights. After UK CAA trials in 1998/1999 of green lights CAP437 Edition 5 had been published in August 2005 to reflect that improvement.
At 18:32:21 hrs, the commander said “YOU GET NO DEPTH PERCEPTION DO YOU?”, and the co-pilot replied “YEAH NOT ON THIS ONE, NOT TONIGHT NO”. The first part of the approach was then marked by steady increases in the collective, tail rotor input, cyclic pitch and cyclic roll input; the radio height initially decreased then increased.
At 18:32:33 hrs, the commander asked “YOU ALRIGHT?”. At this stage the cyclic pitch and roll inputs started to oscillate, whilst still increasing, and the collective increased at an accelerated rate. The helicopter started to pitch nose down and roll to the right as the altitude increased.

At 18:32:35 hrs, the co-pilot replied “NO I’M NOT HAPPY MATE”. The commander asked “WE GOING AROUND?”: at about this time the combined engine torques exceeded 100%. The co-pilot replied “YEAH TAKE… HELP US OUT …..”; however, this request was not initially understood by the commander; and the co-pilot reiterated his request saying “HELP US OUT”.
The commander took control approximately four seconds after the initial request for help and said “I’VE GOT IT I’VE GOT IT I HAVE GOT IT I HAVE CONTROL I HAVE CONTROL”.
This sentence started being spoken urgently but finished calmly.
The helicopter attitude had now reached a maximum of 38º nose down and 38º angle of bank to the right, the IAS was approaching 90 kt and increasing, and the radio altitude, which had peaked at 315 ft, was reducing through 290 ft with a rate of descent of 2,000 ft/min.
One second after the commander stated that he had control, a large left cyclic roll input was made followed one second later by an aft cyclic pitch input. The helicopter rolled through the wings level attitude to about 7º angle of bank to the left and the pitch attitude reduced to 13º nose down. The helicopter was now descending through 180 ft and the IAS was increasing through 100 kt.
During the next six seconds the pitch attitude altered only slightly as the helicopter rolled slowly to the right, the IAS continued to increase as the helicopter descended; the derived vertical speed was initially 1,320 ft/min, increasing to 1,690 ft/min.
During this period the collective was reduced and the engine torques decreased so that their combined input no longer exceeded the 100% level.
At 18:32:45 the co-pilot uttered an expletive, as though disappointed, and the
commander asked “YOU ALRIGHT?”; the co-pilot replied “YEP… NO”, in a resigned
manner.At 18:32:47 the AVAD provided its automatic “ONE HUNDRED FEET” call. Cockpit communications were calm and there were no indications of additional problems.
The last recorded radio altitude was 30 ft; at this time the helicopter attitude was a 12º nose down, with 20º bank to the right and the IAS was 126 kt. The recording ended at 18:32:50 hrs.
On the North Morecambe installation a three-man helideck team were waiting for G-BLUN.
When they first saw the helicopter they estimated the visibility to be about 1,500 m. Everything appeared normal… After what seemed to be a controlled turn to its right the helicopter appeared to initiate a go-around, although it seemed to be faster and closer to the platform than normal.
The helicopter was then seen to bank slightly right as it continued past them, maintaining a steady rate of descent. They lost sight of the helicopter in the dark approximately three seconds before they heard an impact.
The HLO immediately raised the alarm. Two Fast Response Craft (FRC) were launched from field’s sole standby vessel the Highland Sprite. These arrived on scene 16 minutes later.
Th signal from the Automatically Deployable Emergency Locator Transmitter (ADELT) was first detected, by satellite, at 18:35. Two SAR helicopters and two all-weather RNLI lifeboats were deployed initially. The first SAR helicopter arrived at 19:15.
The FRCs from the Highland Sprite, together with the Search and Rescue (SAR) helicopter recovered six bodies; these were identified as being the two pilots and four passengers. Despite an extensive and thorough search of the area surrounding the wreckage the fifth passenger had not been found when this report was published.
[The] rescue crews commented that the yellow immersion suits worn by the passengers were noticeably more conspicuous, when using the helicopter’s searchlight in the darkness, than the blue immersion suits worn by the pilots.
AAIB Safety Investigation
Survivability
Two Home Office pathologists carried out the post-mortems, assisted by a consultant aviation pathologist. It was concluded that five of these six persons had died from multiple injuries consistent with a high vertical impact with some forward motion. One of the passengers showed evidence that he had died of drowning; however, he had sustained multiple injuries and it is almost certain that he was unconscious from the time of the impact.
The accident was not survivable. Had the accident been survivable, and the immersion suits [being worn] sustained no damage, it is expected that the occupants would have had a survivable time of between 6 and 8 hours in the sea with a water temperature of +11.5º C.
Wreckage
The FRCs located floating debris including the tailboom.
The condition of this wreckage suggested that the helicopter had impacted the sea at high speed, and that the remainder would be scattered on the sea bed.

The diving support vessel Vos Sympathy recovered wreckage from the seabed in early January 2007.

The wreckage was laid out in the CHC Scotia hangar at Blackpool. No anomalies were found with the aircraft.
Weather
The Met Office aftercast indicated:
Moderate rain had probably recently cleared to the north-east of the accident area by 1834 hrs, leaving outbreaks of light rain or drizzle and misty conditions. The surface visibility was 3 to 7 km in mist and light rain or drizzle… Cloud was scattered to broken stratus with a base at 700 ft and broken to overcast stratus with a base at 1,200 to 1,500 ft. The surface wind was from 130º at 15 kt, and the wind at 2,000 ft was from 150º at 20 kt.
The sea state was likely to have produced wave heights of approximately 1.1 m from the south-south-east every four seconds.
AAIB note that:
It was a particularly dark night with the overcast cloud completely obscuring any celestial illumination.
AAIB also note that, at the time, the offshore personnel providing met data to helicopters did not, nor where required to hold any formal qualification. The visibility and cloud estimates
were simply made by observation of neighbouring platforms.
Flight Operations
AAIB explain that the CHC Scotia Operational Manual Part A (OM A) stated that the…
…absolute minima for night VFR operations are 5,000 m visibility with a cloud base of 1,200 ft.
However, “for helidecks less than 10 nm apart, at night” the cloud base could be reduced provide it would “allow flight at 500 ft whilst clear of cloud”. AAIB explain that in fact though…
…this limit does not preclude flying between helidecks if the cloud base is lower as long as it is above the Airborne Radar Approach (ARA) limit of 300 ft at night and the crew are flying the ARA procedure. An ARA can be flown to ¾ nm from a platform as measured on the helicopter’s radar. The crew were not conducting an ARA during the flight to the North Morecambe platform and their previous approaches, to the AP1 and the Millom West platforms, were conducted visually.
AAIB organised flight trials using UK CAA flight test personnel.
The approach path flown by the accident helicopter was apparently shallower than the normal approach angle which reduced the depth perception cues of the helideck.
CAA commented:
There appear to be a number of factors…that conspired to contribute towards possible disorientation of the LHS handling pilot. Having asked the RHS pilot to take control following the go-around…it is almost certain that the RHS occupant would have a very degraded, if any, view of the platform and was probably not expecting to have to take control.
While no AS365N handling qualities deficiencies were noted:
- The location of the Radio Altimeter on the LHS (left hand seat) instrument panel was optimised for the final stages of the visual helipad landing and was difficult to include in the instrument scan required during a go-around.
- The torquemeter’s size, readability and location meant it was difficult to use by the LHS pilot at any stage during the high workload of the approach and go-around.

- The helipad lighting included a particularly bright amber perimeter light which made it more difficult to discern the circle of amber lights. It is understood that future helipad lighting will use green coloured lamps which will make it easier to discern the helipad circle amongst the additional lighting on the platform.
- Flying a shallower than optimum approach meant the oval appearance of the circle of lights was difficult to discern and “blurred” into a single line of lights. It would appear from the evidence that G-BLUN flew a very shallow approach and probably never saw a discernible oval of lights.
- The helipad at night gave insufficient cues to allow distance to be judged and without additional information from the weather radar or GPS the crew of G-BLUN would not have known the distance to run accurately.
- When the RHS (right hand seat) pilot took control he would have had no visual cues from the platform.
AAIB comment that:
The use of an [Synthetic Training Device] STD, which fully replicates the flight deck and all of the associated controls, is therefore an invaluable tool in the training of pilots.
At the time CHC Scotia were not using an simulator for the AS365, even though one was available. They introduced simulator us in spring 2008 for the AS365 and in 2009 for the S-76.
AAIB discuss the OM B procedure and call outs for a go around. They observed that:
There is no direction to the crew regarding further actions after executing a go-around when flying below a low cloud base or when the visibility is poor, nor is there any guidance on the use of the AP coupler during a go-around.
They also discuss the OM A guidance in pilot incapacitation, which states…
…crewmembers should closely monitor the helicopter’s flight path in the critical stages of
take off, initial climb, final approach and landing and immediately question any deviation from the norm.If incapacitation is identified, the able crewmember must assume control and return the helicopter to a safe flight path.
There was, however, no definition of a “deviation from the norm”, corrected by a Flying Staff Instruction (FSI) published after the accident.
AAIB also comment on AVAD use:
During the three approaches, as recorded on the CVR, the commander said “JUST YOUR BUTTON TO DO” once visual with the platform. This is believed to have been a reminder, to the co-pilot, to suspend the AVAD as no ‘CHECK HEIGHT’ was subsequently heard.
The OM contains no guidance on the procedure and calls to be employed when suspending the AVAD warning.
Unhelpfully, AAIB found a circular reference:
OM Part A section 8.3.4.4 stated ‘see OM Part B section 3 for type specific radio altimeter bug setting procedures’, however, OM Part B section 3.1.1 stated ‘see Part A Section 8 paragraph 8.3.4’.
After further examination:
The radio altimeter bug settings were actually found in Appendix A to Section 3, on side two of the cockpit checklist. For a VFR landing offshore the radio altimeter bug should have been set at 200 ft.
The operator stated that an FSI had been issued which provided guidance on the use of the AVAD.
However disappointingly:
…a copy of the FSI could not be found. A new FSI has now been published which provides guidance on the use of the AVAD, and this will be incorporated into the new OM.
CHC Scotia Safety Management
This accident pre-dated the regulatory adoption of safety management system (SMS) requirements (then scheduled for 2009 in Europe, far earlier than in US and Canada for example for similar types of operation). AAIB note that:
…the operator stated that all their customers require a SMS to be in place.
Irrespective of that, JAR-OPS 3.037 required an Accident Prevention and Flight Safety Programme.
CHC Scotia had a nominated Company Flight Safety Officer (FSO). AAIB report they were…
…responsible to the Flight Crew Manager for the collection, collation, editing and dissemination of flight safety information and for the promotion of flight safety awareness amongst all company employees. He is also required to monitor all occurrence reports and, where necessary, ensure that appropriate follow up action is taken.
There is an obvious disconnect in being “responsible to the Flight Crew Manager” but with a role meant to engage with “all company employees”.
Despite a fleet of 33 helicopters at the time, and the claim that an SMS was in place, this was only a part-time role according to the AAIB and there was “no dedicated assistant” though “base FSOs were appointed for all operating bases, including Blackpool”. Due to the part-time nature of the role:
He was required to work 200 days per annum, and do half of the flying of a standard line pilot; this should therefore have resulted in 91 days of flying and 109 days for administrative work.
However:
In the 6 months preceding the accident he completed 69 flying days and 35 administrative days.
…it would appear that the operator had not provided sufficient dedicated resources…
Prior to 2005 flight safety issues had been discussed at a monthly Occurrence Review Board (ORB). The Accountable Manager or his deputy attended ORBs. In 2005 instead separate quarterly Flight Safety meetings were introduced. The operator held three of four meetings during that year but the Accountable Manager did not attend them. In 2006 they reverted to the previous arrangement The logic for these changes was not revealed by AAIB. AAIB also do not comment on the availability of minutes or the procedures followed in the meetings, matters discussed by the Irish AAIU investigation into a 2017 CHC Ireland S-92A fatal accident (e.g. 1.17.4.2 Operator’s Safety Management System), where one SMS recommendation was raised.
AAIB note that the voluntary CHC Scotia SMS…
…was defined in a main document, plus separate documents entitled ‘Safety Case for Operations at [base name]’ for each of its four operating bases in the UK.
In the Executive Summary and Introduction of each base Safety Case it said:

The conclusion to each document is signed by the Accountable Manager and the Business Unit Leader.
Remarkably:
Although the FSO was listed as one of the ‘intended readership’, he was unaware of this.
The UK Air Navigation Order also required Flight Data Monitoring (FDM). This was not, according to AAIB, expected to be introduced to the CHC AS365 fleet until 2009.
UK CAA Regulatory Oversight
On the 23/24 November 2006, the CAA’s Flight Operations Inspector conducted a regularly scheduled audit of the Blackpool base which concluded satisfactorily with minor findings.
The MD of the operator called a meeting with the CAA to discuss various aspects of the operator’s business structure. During that meeting, which occurred on 18 December 2006, a variety of topics were discussed, including CAA concerns regarding the maintenance and operations aspects arising from recent AOC Variations for new types [the S-92A had been introduced that year].
After the accident the operator was informed that an audit would be conducted in February 2007. Afterwards…
…CAA met with the operator to discuss the results of the audit, which raised concerns about the Company’s management organisation, training and accident prevention and flight safety
programme.
Subsequently the operator responded to these concerns and at the time the AAIB report was published in October 2008:
…CAA is continuing to monitor progress and the Company is still subject to heightened oversight.
During that period of ‘heightened oversight’ CHC Scotia also suffered:
- A serious incident on 20 November 2007 to AS332L2 G-CHCF at Aberdeen during an OPC being conducted on the aircraft, rather than in a simulator, where excessive freewheel wear resulted in the number 2 engine shutting down while the no 1 engine was in Training Idle System to simulate one engine inoperative, resulting in a ‘firm’ landing.
- An accident on 9 March 2008 to AS365N G-BKXD at the Leman gas field, Southern North Sea. While landing on the Leman 27 Alpha D helideck the helicopter’s fenestron fairing struck the handrails on the installation’s crane. The AAIB said “choice of approach profile, limited helicopter performance, approach technique and possible fatigue were considered to be factors in the accident”. G-BKXD was the same aircraft used in the UK CAA flight trials for the G-BLUN AAIB investigation. CHC Brazil had a more dramatic S-92A helideck obstacle strike less than 10 years later.
In February 2007 UK CAA wrote to all offshore operators to “encourage” “consideration” of several matters:

The weakness of this simplistic approach was highlighted in the AAIB report into a 2009 accident involving another UK operator. Notably the letter makes no mention of any flight safety / accident prevention matters that other operators needed consider.
AAIB Safety Analysis
There was no evidence of any technical malfunction that may have contributed to the accident and the investigation therefore sought to understand why two experienced pilots were unable to stop a serviceable helicopter flying into the sea.
AAIB explain that:
It is therefore necessary to understand the human factors involved in the sequence of events that led to the accident, and to analyse the helicopter’s response to control inputs.
The organisational factors and the individual and crew actions are then considered.
They say that after…
…the start of the descent…the descent became progressively steeper, there was a steady reduction in collective demand and a steady, positive change in pitch attitude, rather than the adoption of fixed values.
It appears that the intent was to reduce speed throughout the descent until 30 kt was achieved. Conceivably, the pitch change could have been the result, in part at least, of inadvertent activation of the pitch trim. This might have arisen if the co-pilot had already been tense at the initiation of the descent, but the limited evidence from the CVR does not support this concept. However, as a matter of principle, fixed attitude or power settings simplify glidepath control, particularly when approach angle cues are limited.
The change in strategy…is clear, as the collective demand increased steadily, the descent rate was arrested and the helicopter began to climb, and this suggests a change in the appreciation of the helicopter’s position or motion relative to the deck.
It does not appear to represent an attempt to go-around since that decision was not discussed until more than 15 seconds later. Two possible explanations are that the descent was initiated too early or the initial approach angle was too steep, both resulting in the final approach angle becoming too shallow.
A prior comment by the commander, “FIFTY FIVE”, was a standard call related to airspeed.
It is assumed this was not the sole stimulus for the change of strategy. It seems more likely that it was a more complex response based on a revised assessment of the approach angle.
In a period of about 35 seconds, there are two distinct control strategies, rather than a continuous adjustment of one strategy. This could be indicative of a lack of attention but more likely indicates a difficulty in assessing approach angle. Indeed, the crew discussed the difficulty in depth perception at about the time that the change in strategy was initiated.
The approach was flown essentially by reference to visual cues. In dark, overcast conditions, it is likely that some cues were degraded or absent. For example, without a distinct horizon the assessment of pitch attitude and approach angle (by reference to the depression of the deck below the horizon) would be compromised. Without textural cues in the ground plane (in this case the sea surface), judgement of pitch attitude and approach angle by inference from textural perspective would also be compromised, as would the appreciation of the range to the deck.
The illuminated deck would have provided limited cues to roll attitude and, by reference to its apparent size, to range. The crew’s judgement of range and rate of closure to the platform would have improved as they approached the platform, but, initially, this would be relatively insensitive.
The UK CAA flight trials…
…suggested that a bright yellow perimeter light tended to obscure the circle of lights marking the helideck, (although it is uncertain whether this was the case on the night of the accident). This obscuration, if it had been present, may have been more pronounced at longer range making approach angle judgements initially more difficult.
AAIB note that:
The recorded data indicates that the helicopter started to oscillate in both pitch and roll as it approached the helideck, and it is probably this that prompted the commander to ask “YOU ALRIGHT”; the co-pilot replied “NO I’M NOT HAPPY MATE”. The commander then asked “WE GOING AROUND?” and the co-pilot replied “YEAH TAKE… HELP US OUT (name)”, but this request was not initially understood by the commander and the co-pilot reiterated his request saying “HELP US OUT”.
They then opine that:
The co-pilot was not able to control the helicopter during the early stages of the go-around but there was no clear decision to go-around and no definitive call to initiate the procedure as required by the OM. [The commander] did not take control until approximately four seconds after the initial request for help. The confusion that was generated contributed to an imprecise handover of control.
Without the benefit of sound SOPs, and the opportunity to practise regularly these exercises in the controlled environment of an STD, the crew were now reliant upon the flying skills of the commander.
It is clear that he was not expecting to take control of the helicopter; nevertheless, his initial actions in rolling the helicopter to a level attitude and reducing the pitch angle were correct.
But he was now devoid of any external visual cues and became concerned for the well being of his co-pilot… This distraction from his instrument scan, albeit brief, probably explains why he did not notice the increasing angle of bank to the right and the continuing descent into the sea and possibly why he did not hear the AVAD warning at 100 ft. His problems would have been compounded by the disorientation induced by the rapid roll to the left during the initial recovery and the inherent instability of the helicopter.
AAIB Safety Recommendations
AAIB made not one but two recommendations to CHC Scotia to review of their Standard Operating Procedures relating to offshore approaches.
AAIB recommended that UK CAA ensure that the recurrent training and checking be carried out in an approved simulator and “ensure that personnel who are required to conduct weather observations from offshore installations are suitably trained, qualified and provided with equipment that can accurately measure the cloud base and visibility.”
Two recommendations were made to EASA for research on instrument approaches to offshore installations and survival suit conspicuity.
Our Safety Observations & Two Trilogies of Offshore Helicopter Safety Case Studies
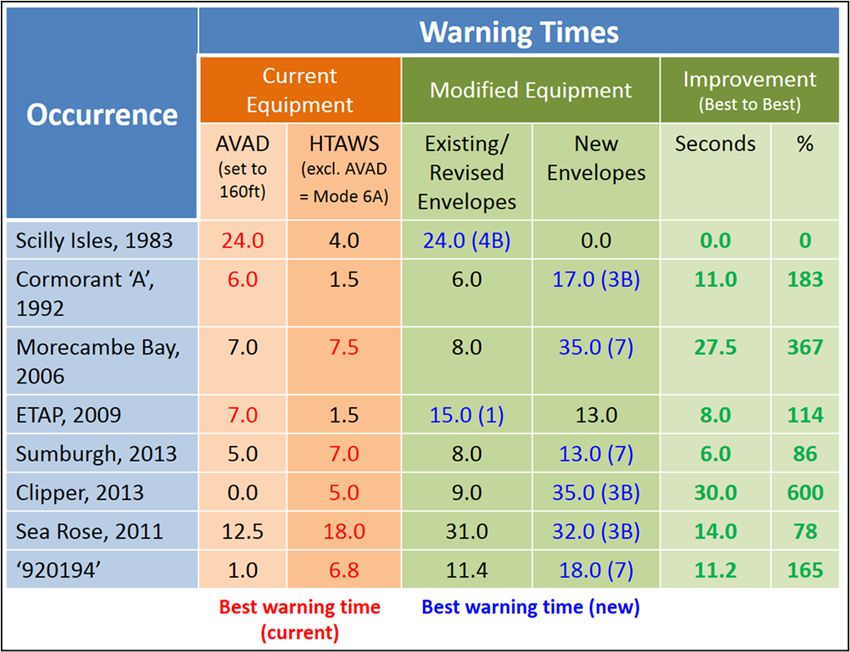
Helicopter Terrain Awareness and Warning System (HTAWS): subsequent UK CAA research identified that while AVAD could provide 7 seconds warning in the G-BLUN scenario, an optimised HTAWS with specific offshore envelopes could increase this to 35 seconds.
The introduction of such a capability is a UK CAA requirement from 2025 onwards.
With Part 135 operators in the US being required to have an SMS in the next 3 years, operators would be well advised to seek the implementation of an effective and appropriately resourced SMS, and avoid it becoming shelfware. Back in May 2012 Flight Safety Foundation (FSF) President Bill Voss wrote: SMS Reconsidered. Voss posed four key questions to ask of an SMS: “What is most likely to be the cause of your next accident or serious incident? How do you know that? What are you doing about it? Is it working?” He also made the insightful comment: “The easiest way to make people do silly things is to measure them against mindless objectives”.
UK CAA CAP1077 (Specification for an Offshore Helideck Lighting System) published in 2013 stated:
There have been three notable accidents in which visual cueing at offshore platforms is believed to have been a significant factor.
- These accidents were:
S-76A G-BHYB of BIH (later bought by CHC), near Fulmar Alpha, 9 December 1987, covered by Aerossurance in 2022 - G-BLUN on 27 December 2006
- EC225 G-REDU of Bond Offshore Helicopters near the ETAP platform on 18 February 2009, covered by Aerossurance earlier in 2024
UK CAA noted that in all three cases:
- Helicopters were conducting manually flown, visual approaches to offshore platforms at night
- The prevailing meteorological conditions resulted in a degraded visual cueing environment
- The pilot became disoriented and/or suffered a loss of situational awareness.
This article therefore completes this trilogy of case studies.
G-BLUN and G-REDU also make up a another trilogy, with the CHC Scotia AS332L2 G-WNSB accident on approach to Sumburgh, covered by Aerossurance in 2016. All three accidents would have benefited from the new enhanced offshore HTAWS, discussed above, with 86-367% greater warning.
The 2013 CHC accident was at least partially responsible for triggering a number of initiatives and reports including:
- The Joint Operators Review (JOR) review and the formation of HeliOffshore.
- A hurried UK CAA Review of North Sea helicopter safety, and the CAP1145 report.
Considering the issues already raised in the G-BLUN and G-REDU reports its perhaps surprising the UK CAA didn’t look at offshore helicopter operations in a structured way earlier that 2014.
HeliOffshore has recently issued the fourth iteration of its offshore helicopter Flight Path Management (FPM) recommended practice, highly relevant to a number of these accidents:

This contains extensive relevant recommendations:


Safety Resources
The European Safety Promotion Network Rotorcraft (ESPN-R) has a helicopter safety discussion group on LinkedIn. You may also find these Aerossurance articles of interest:
- North Sea Helicopter Struck Sea After LOC-I on Approach During Night Shuttling
- Loss of Sikorsky S-76C+ 5N-BQG of Eastwind Off Nigeria 24 October 2024
- South Korean Night Black Hole Spatial Disorientation Fatal Helicopter Accident
- Loss of Control, Twice, by Offshore Helicopter off Nova Scotia
- Offshore Night Near Miss: Marine Pilot Transfer Unintended Descent
- Technology Friend or Foe – Automation in Offshore Helicopter Operations and Aerossurance Marks RAeS 150th Anniversary by Sponsoring Rotorcraft Automation Conference
- AAIB Report on 2013 Sumburgh Helicopter Accident
- Fatal Offshore S-76C++ LOC-I & Water Impact Brazil 2022: CENIPA Investigation
- SAR Helicopter Loss of Control at Night: ATSB Report
- NTSB Investigation into AW139 Bahamas Night Take Off Accident
- Night Offshore Training AS365N3 Accident in India 2015
- BFU Investigate S-76B Descending to 20ft at 40 kts En Route in Poor Visibility
- Review of “The impact of human factors on pilots’ safety behavior in offshore aviation – Brazil”
- HEMS S-76C+ Night Approach LOC-I Incident
- HF Lessons from an AS365N3+ Gear Up Landing
- NH90 Caribbean Loss of Control – Inflight, Water Impact and Survivability Issues
- Helideck Heave Ho!
- AAIB Report on 2013 Sumburgh Helicopter Accident
- AAIB Report on the Ditchings of EC225 G-REDW 10 May 2012 & G-CHCN 22 Oct 2012
- EC225 LN-OJF Norway Accident Investigation
- CHC Scotia AS332L Rollover on West Navion Helideck After Loss of Dynamic Positioning
- 2009 Newfoundland S-92A C-GZCH Accident: A Failure of Design and Certification
- ADA AW139 A6-AWN Ditching off UAE, 29 April 2017: Final Report
- Night Offshore Windfarm HEMS Winch Training CFIT
- NTSB Report on Bizarre 2012 US S-76B Ditching
- Fatal USCG SAR Training Flight: Inadvertent IMC
- Sikorsky S-92A Loss of Tail Rotor Control Events
- S-92A Emergency Landing: MGB Oil Checklist Recommendation
- Loss of Bell 412 off Brazil Remains Unexplained
- RLC B407 Reverses into Sister Ship at GOM Heliport
- CAP1145 Helicopter Water Impact Survivability Statistics – A Critique
- Hong Kong Harbour AW139 Ditching – HKCAD Report Issued
- Dramatic Malaysian S-76C 2013 Ditching Video
- In-Flight Flying Control Failure: Indonesian Sikorsky S-76C+ PK-FUP
- Safety Lessons from a Fatal Helicopter Bird Strike: Sikorsky S-76C++ N748P, 4 January 2009
- Wrong Deck Landings
- Offshore Helicopter Emergency Response
- Blinded by Light, Spanish Customs AS365 Crashed During Night-time Hot Pursuit
- BK117 Offshore Medevac CFIT & Survivability Issues
- SAR AW139 LOC-I During Positioning Flight
- Night Offshore Take-Off Loss of Control Incident
- Night Offshore Helicopter Approach Water Impact
- UPDATE 8 February 2025: S-76D Loss of Control on Approach to an Indian Drilling Rig
- UPDATE 25 May 2025: CHC Sikorsky S-92A Seat Slide Surprise(s)