Night Offshore Helicopter Approach Water Impact (Bond Offshore Helicopters EC225 G-REDU, BP ETAP CNS)
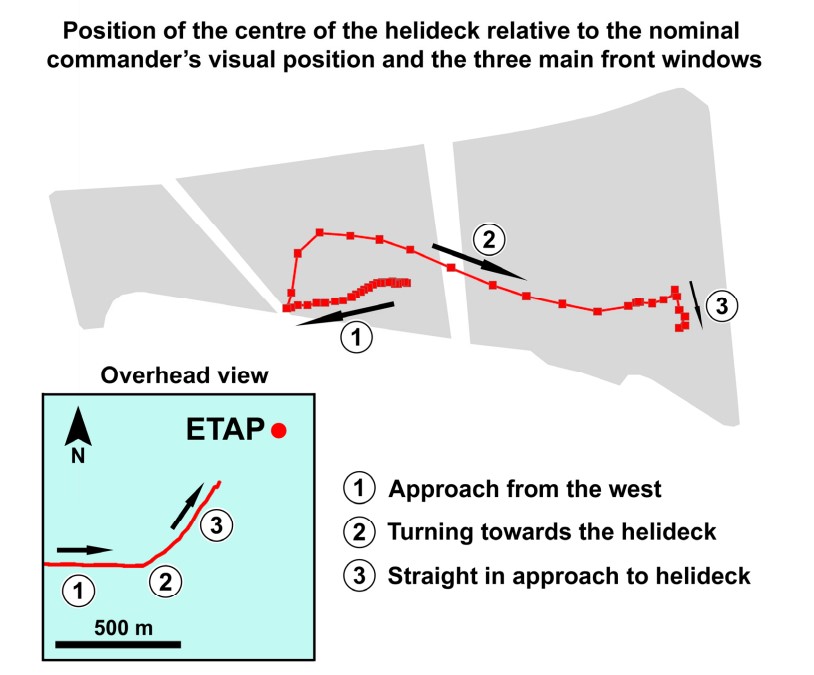
On 18 February 2009 Airbus EC225 G-REDU of Bond Offshore Helicopters impacted the sea during a night visual approach to BP‘s Eastern Trough Area Project (ETAP) Central Production Facility. The crew’s perception of the position and orientation of the helicopter relative to the installation proved erroneous. After entering the water the helicopter floated and everyone on board was rescued. The aircraft capsized subsequently.

This article primarily summarises the extensive 171 page UK Air Accidents Investigation Branch (AAIB) safety investigation report published 14 September 2011.
Background
Bond Offshore Helicopters had been formed in August 2001 and commenced operations in August 2004 with a long term contract for BP for commercial air transport and for Search and Rescue (SAR) operations, known as ‘Jigsaw’. They subsequently gained work with some smaller oil & gas customers and in February 2009 added another large oil and gas customer in Aberdeen. They had also won contracts, commencing in 2010 in Blackpool and Norwich with the AS365N3.
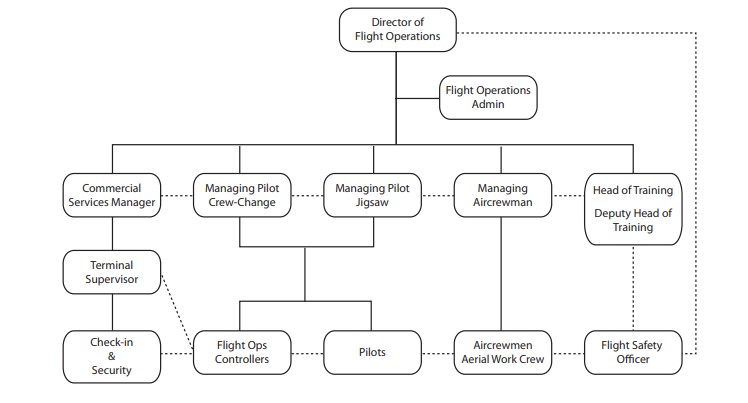
Their operations department was structured as follows:
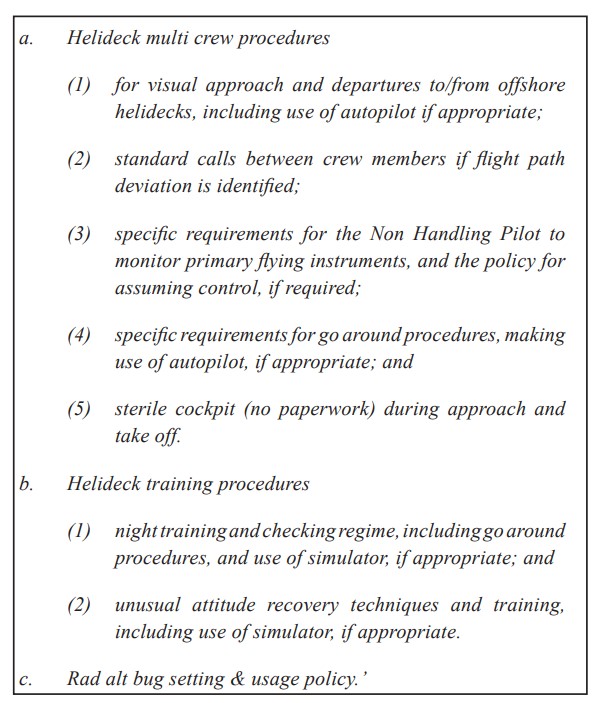
On 27 December 2006, at night, in poor weather CHC AS365N G-BLUN, operating from Blackpool, impacted the Irish Sea near the North Morecambe gas platform with 7 fatalities On 12 February 2007, the UK CAA Head of Flight Operations Inspectorate (Helicopters) wrote to all UK offshore helicopter operators to ask they review the following topics and inform their CAA inspector:
Consequently the Bond Director of Flight Operations tasked their Flight Safety Officer with “carrying out an audit and Flight Operations Risk Assessment (FORA)” against these issues.
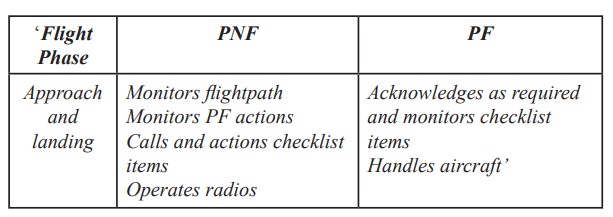
AAIB found that the Bond Operations Manual at the time of the G-REDU accident summarised crew approach and landing duties as follows:
 However:
However:
There were no specific vertical or horizontal profiles set out in the Operations Manual for an offshore visual approach.
More comprehensive duties, challenges and responses were set out for precision and non-precision instrument approaches. These included altitude calls and instrument crosschecks as well as any deviation from the horizontal or vertical profile of the approach.
Also:
There was no specific company lesson plan for teaching offshore approach and landing techniques.
However, the training staff had detailed lesson plans which identified the need to use the flight instruments to monitor the approach and the Oculogravic illusions which may be experienced when pitching up.
However:
Neither crew member could recall receiving this information during their company training.
G-REDU, registered in May 2008, was the first EC225 in their fleet, that until that point had consisted of AS332L2s.
A Honeywell MkXXII Enhanced Ground Proximity Warning System (EGPWS) Terrain Awareness Warning System (TAWS) had been retrofitted to G-REDU in November 2008. This modification was not required by regulation but was “recommended” for “long term” contracts in the Aircraft Management Guidelines (AMG Report 390) of the International Association of Oil and Gas Producers (IOGP, then OGP), of which BP was a member. This recommendation was subject to the caveat that “when an approved modification exists for the aircraft type and it is recommended by Company Aviation Advisory personnel”. The TAWS replaced the original Automatic Voice Alerting Device (AVAD), also an OGP recommendation for long term contracts.
Although recommended by OGP, AAIB note that because helicopters can “land close to or on nominally hazardous terrain or obstacles, the levels of protection” from TAWS “are reduced under certain circumstances, such as low airspeed”. AAIB explain that defined the “applicable speed range for the EGPWS MkXXII as 85 kt and above. Therefore, under this certification, there are no alerting requirements below 85 kt”. Also:
The certification of the installation of TAWS does not require that a comparison be made between TAWS alert envelopes and the ability of the helicopter to recover from the situation once an alert has been triggered.
Furthermore Honeywell…
…indicated that some operators would prefer not to have oil and gas platforms included in the database in order to reduce the amount of nuisance warnings. The ETAP platform was not in the [EGPWS] database.
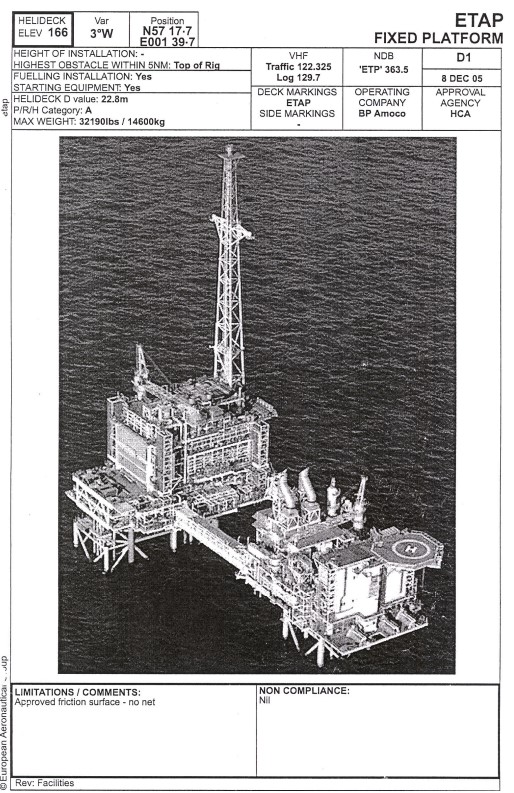
ETAP is in the Central North Sea 125 nm east of Aberdeen.
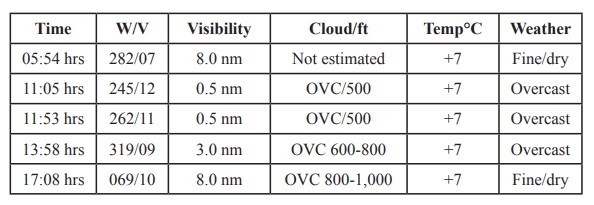
The flight was planned based on weather reported by ETAP at at 1708 hrs:
The Accident Flight
The helicopter departed Aberdeen at 17:42 Local Time with 2 crew and 16 passengers.
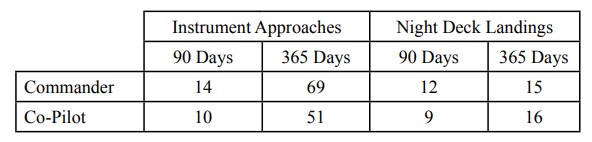
The aircraft commander had 17,200 flying hours total time (in the Royal Navy and the civil offshore industry), with 3,018 on type according to AAIB. Closer inspection suggests this was likely combined AS332L/AS332L2/EC225 time as in September 2007 he completed an AS332L2 Differences Course and a year later a EC225 Differences Course (both conducted in-house).
The co-pilot had 1,300 flying hours total time, with 808 on type. He had also his AS332L2 and EC225 Differences Course in the same months as the aircraft commander.
The flight crews’ recent instrument approach and night approach history was as follows:
Thirteen minutes after take off…
…the commander recalled turning ON the ACAS [Airborne Collision Avoidance System] and, coincident with that action, a TAWS caution caption being displayed on the Caution and Warning Panel (CWP). It cleared shortly after, with no intervention from the crew, and there was no indication of the system having failed on any of the Multi-Function Flight Displays (MFDs).
On board the ETAP the Helicopter Landing Officer (HLO) and the helideck team assembled at c 1800 hrs to complete their routine helideck inspection and to perform the fuel checks. The sun had set an hour earlier.
Whilst on the deck, the HLO noticed that the cloud base was just above the top of the flare pylon, which is 525 ft amsl, and estimated that the visibility, in the dark and foggy conditions, was about 0.5 nm.
This information was relayed to the flight crew. In contrast, shortly afterwards, the radio operator on the Galaxy 1 drilling rig radioed the ETAP that they could see the ETAP and estimated the visibility to be around 10 miles.
At 1814 hrs the crew confirmed that they were receiving transmissions from the ETAP non-directional beacon (NDB), which they had identified, and the commander carried out a briefing for an Airborne Radar Approach (ARA) to the ETAP platform. It was to be a straight-in ARA, commencing from an altitude of 1,500 ft, descending to a Minimum Descent Height (MDH) of 300 ft, with a Missed Approach Point (MAP) at 0.75 nm.
The commander would perform the landing and so was Pilot Flying (PF).
At 1819 hrs, the descent checks were completed and the helicopter was descended, using the autopilot (AP), to an altitude of 1,500 ft.
At 1825 hrs, after passing through a layer of cloud, visual meteorological conditions (VMC) prevailed and the crew could see what appeared to be the ETAP platform at a range of 13 nm.
The aircraft descended through a height of 1,500 ft RA at 1828 hrs. The crew…commenced the approach checks.
While the crew had briefed for an ARA, now being visual with what was believed to be the ETAP, they commander rebriefed for a visual approach.
“IT WILL BE AN ENROUTE DESCENT DOWN TO 300 FT USING THE NDB NEEDLE. THERE IS HARDLY ANY WIND THERE’S 5 KT THERE. HE SAID HIS WIND WAS 350. WE’LL GET ANOTHER WIND CHECK FROM HIM BEFORE WE GET THERE. RIGHT LANDING I’LL COME ALONGSIDE MOVE DOWN AND RIGHT. I’LL CALL YOU ON COMMITTED. IF THERE IS A PROBLEM IT’S A GO AROUND, VTOS, VY AND WE’LL GO TO ABERDEEN”. The co-pilot acknowledged the briefing and had no questions.
AAIB comment:
The crew were not exhibiting any signs of stress and were demonstrating good Crew Resource Management (CRM), jointly agreeing their plan with no cross-cockpit gradient.
At 1827 hrs the co-pilot carried out the pre-landing passenger briefing whilst the commander contacted the ETAP platform on the radio for an update on the weather.
However the ETAP reported that the visibility had reduced to what was estimated to be 0.5 nm.
The co-pilot was unaware of this report, as he was briefing the passengers at the time.
The crew could see the ETAP [gas] flare, and the lights of the installation, and agreed to carry out a straight-in visual approach, descending to a height of 300 ft to ensure clearance from any cloud. They carried out the final approach checks and commenced the descent with reference to the radio altimeter.
At 1831 hrs the helicopter descended to a height of 300 ft, at a range of 7 nm from the ETAP. As it did so it entered low cloud and the crew lost sight of he ETAP, so they commenced a climb and at a height of 400 ft they regained visual contact with the platform.
AAIB note that:
The workload of flying the helicopter was at this stage undertaken by the upper modes of the AP [autopilot], with the commander selecting and monitoring height and speed. This provided him with the capacity to look out of the cockpit at the platform whilst the AP maintained a safe flight path
The crew discussed the conditions and agreed that they had encountered a fog bank. They elected to remain at 400 ft and, with 5 nm to run to the ETAP, continued the approach visually, monitoring their range using the weather radar.
At 1833 hrs the crew, using the Navigation Display (NAVD), agreed that the wind was about 5 kt from the north. The commander reduced speed from 130 kt to 80 kt and, with 4.5 nm to run, they again ‘paged down’ the weather radar.
With 3 nm to run to the platform, the co-pilot advised the commander to alter the helicopter’s heading five degrees to the left, based on the weather radar picture. The commander then stated that they would have to make a left turn into the wind. He again reduced the speed, passing through Vy [best rate of climb speed] (80 kt) with some 2 nm to run to the platform.
At 1835 hrs the radar was again ‘paged down’ and the commander descended the helicopter to a height of 300 ft. The co-pilot stated “JUST ONE MILE TO GO” and, when level at 300 ft RA [Radalt height], both pilots could see the glow of the flare, although they were having difficulty seeing the lights of the platform.
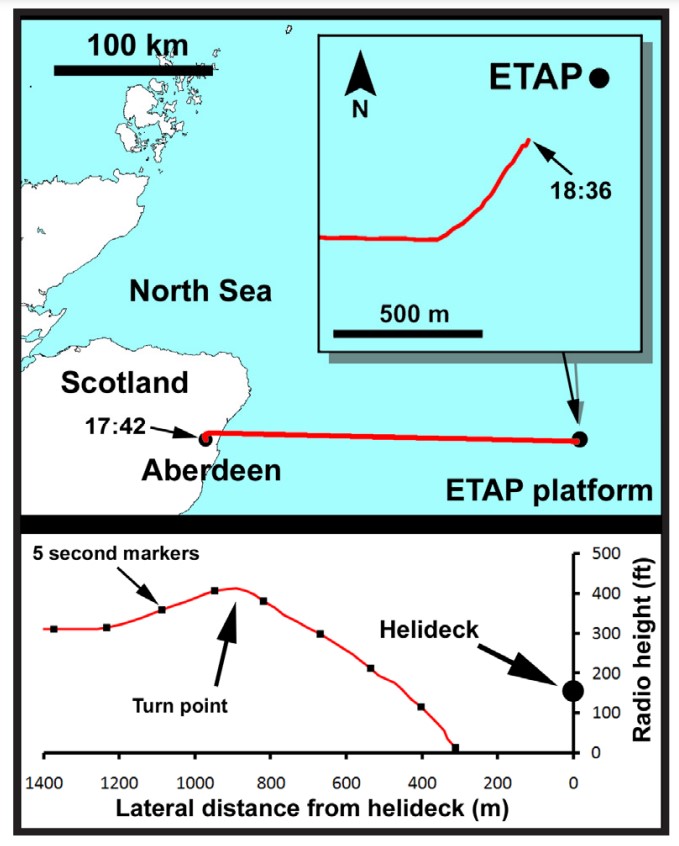
At 1836 hrs the co-pilot confirmed that the range to the platform was 0.75 nm. The commander stated “OK, WE’LL JUST STAY ON THIS HEADING THEN GO UP”. The co-pilot responded “OK AS YOU CLIMB, IF WE MAKE A SECOND APPROACH I RECKON WE’LL GET IN. CAN YOU SEE”.
As the helicopter passed [up] through 350 ft, the commander could see the flare and the diffused lights of the platform. As the helicopter reached the top of its climb, at a height of 415 ft, the co-pilot could see the flare, the diffused lights of the platform and the green perimeter lighting of the helideck, which has an elevation of 166 ft.
The commander decoupled the upper modes of the AP and suspended the ‘CHECK HEIGHT’ aural alert that would have been activated as the aircraft passed through a height of 150 ft.
AAIB comment that he did not verbally articulate these actions and that…
…the workload involved in flying the helicopter on instruments, as well as maintaining sight of the platform, would have increased.
This also posed a practical dilemma:
If he retained his instrument scan, the possible effect was to lose sight of the platform at a late stage in the approach. In order to maintain sight of the platform, the attention to instrument flying was reduced. The option to execute a go-around at this stage was available but, with the platform lights visible, there appeared to be no need.
AAIB note that…
…the selected 150 ft height alert remained in the form of visual warnings displayed on each pilot’s Primary Flight Display (PFD). A second audio voice warning of ‘ONE HUNDRED’, which cannot be suspended, is automatically activated by the TAWS when the aircraft descends through a height of 100 ft RA.
The commander commenced a 20° banked turn to the left and the co-pilot informed him that he was descending.
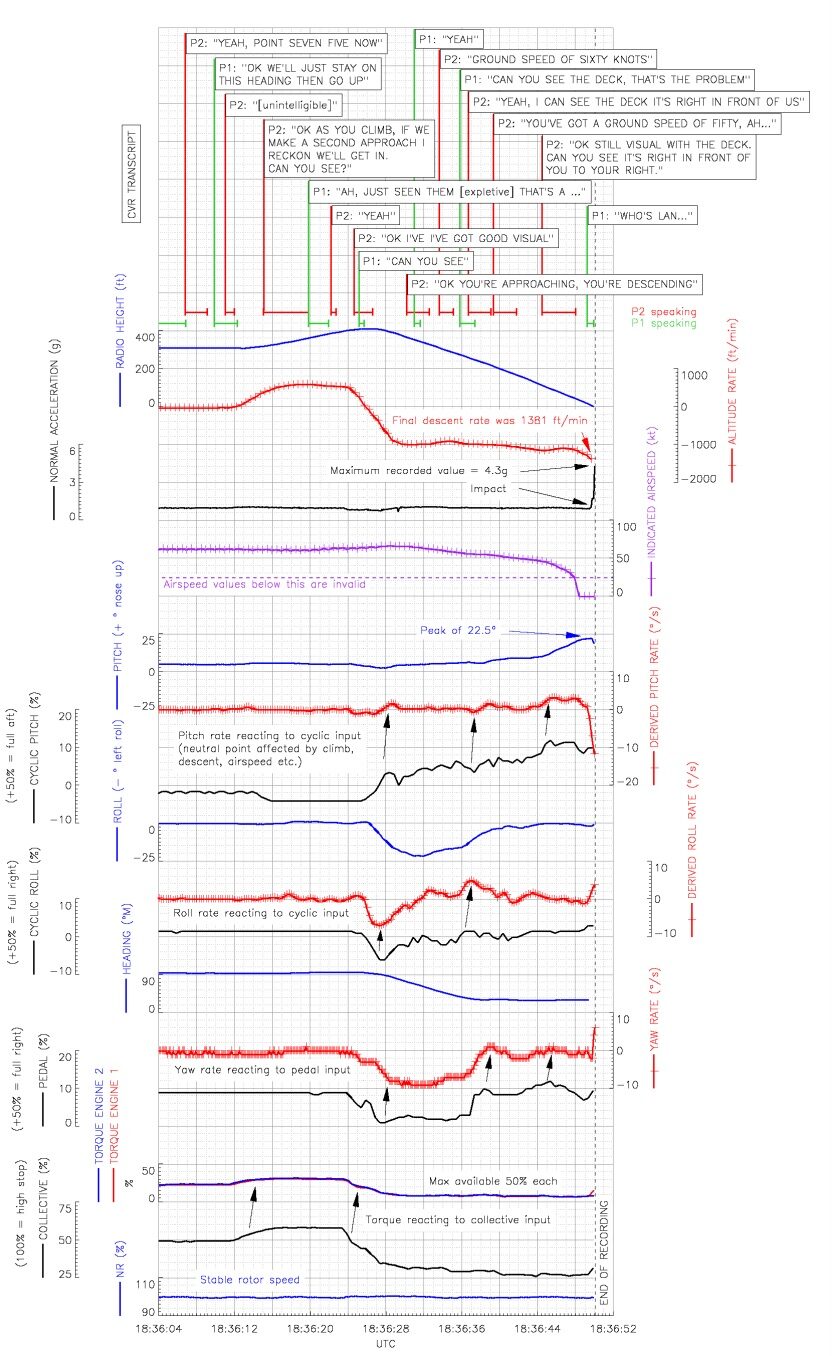
 The commander could see the flare and the lights of the platform but could not see the helideck. As the helicopter passed 280 ft, he asked the co-pilot, “CAN YOU SEE THE DECK, THAT’S THE PROBLEM”. The co-pilot responded “I CAN SEE THE DECK RIGHT IN FRONT OF US YOU’VE GOT A GROUND SPEED OF FIFTY FIVE. AH”. As he finished his response, the helicopter passed through 200 ft.
The commander could see the flare and the lights of the platform but could not see the helideck. As the helicopter passed 280 ft, he asked the co-pilot, “CAN YOU SEE THE DECK, THAT’S THE PROBLEM”. The co-pilot responded “I CAN SEE THE DECK RIGHT IN FRONT OF US YOU’VE GOT A GROUND SPEED OF FIFTY FIVE. AH”. As he finished his response, the helicopter passed through 200 ft.
The co-pilot was visual with a diffused picture of green lights but momentarily lost visual contact, simultaneously announcing the word “AH”. By moving forward in his seat, he was able to relocate the green deck lights.
The commander rolled the helicopter out of the turn, having turned through 62° instead of the intended 90°. It passed through 150 ft, the height at which the ‘CHECK HEIGHT’ alert should have activated had it not been suspended, at a rate of descent of 1,096 ft/min with an IAS of 49 kt, achieved ‘wings level’ and continued to descend.
The commander could still make out the lights of the platform and had the sensation that his approach was fast and high.
There was no TAWS ‘ONE HUNDRED’ aural alert when the helicopter passed through 100 ft, though the system had activated at 100 ft on the previous offshore landing that day. Both pilots’ attention “was fully focused on the external visual picture”, in other words the instruments were no longer being monitored.
The co-pilot, believing that they were above the height of the deck and in close proximity to it, checked the radar for its range. He then advised the commander, “OK STILL VISUAL WITH THE DECK CAN YOU SEE IT’S RIGHT IN FRONT OF YOU TO YOUR RIGHT”. The commander could not see the helideck and started to ask the co-pilot “WHO’S LA..(NDING)” but his question was interrupted as the helicopter impacted the surface of the sea.
On the helideck the HLO had had seen the helicopter’s landing light.
He estimated that it was at a range of 500 metres and appeared to be descending rapidly. He then lost sight of the light and heard a splashing sound “like a surfboard hitting the water” The HLO immediately realised that the helicopter had struck the water and raised the alarm [as did another witness].
Survivability & Rescue
The impact with the water was survivable, involving little or no main fuselage deformation, no seat damage and no reported occupant injuries.
The passengers were not aware of anything unusual until, after “a heavier than normal” landing, the cabin began to fill with water.
The Emergency Flotation System (EFS) had been activated by the Automatic Float Deployment System (AFDS). The helicopter remained afloat and upright in what were initially Sea State 3 conditions and <5°C sea temperature.
…electrical power to the flight deck was lost. The Emergency Exit Lights were the only lights illuminated and both engines remained running. In the darkened environment, the commander located the engine control switches on the overhead panel, by feel, and selected them to OFF. He shouted to the passengers not to evacuate until the rotors had stopped. both engines running down, he gently applied the rotor brake in order to prevent the helicopter rolling over.
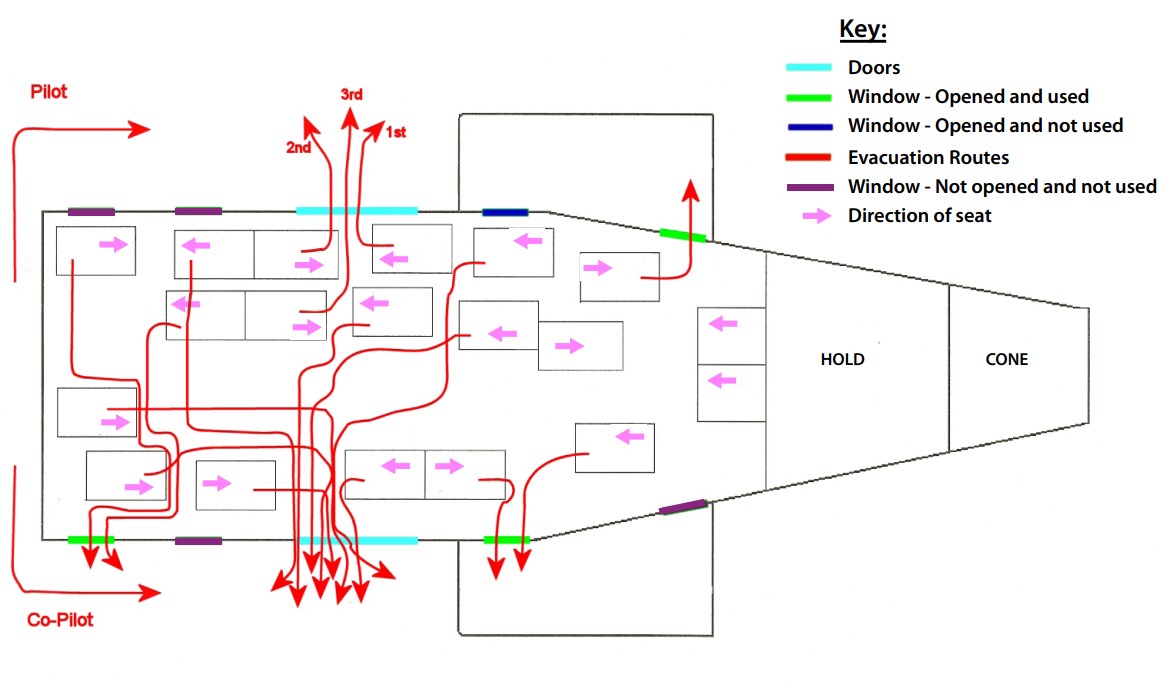
The co-pilot deployed the left had external liferaft using a handle behind his head.
As the left liferaft was inflating, it seemed to the passengers to be restricted by various lanyards, so some of them assisted with its deployment. The right liferaft external deployment handles on the [out]side of the fuselage were pulled [by a passenger] but the liferaft did not deploy as expected, so the passengers manually removed the liferaft from its housing in the right sponson allowing it to inflate.
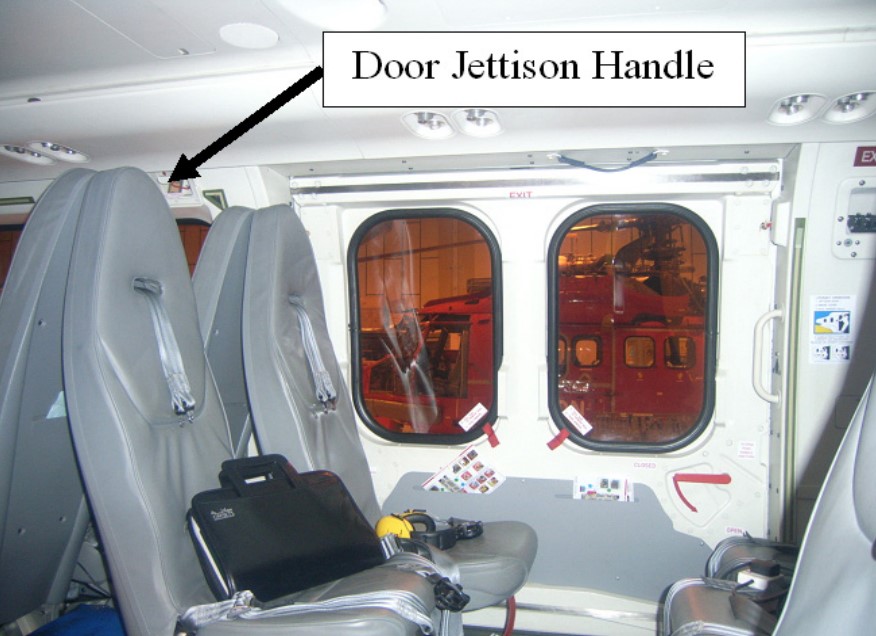
Most of the passengers did not experience any problems with the exits. However, those who were sitting beside the right cabin door were unable to locate that door’s jettison handle.
There was no placard at the door to highlight the door jettison handle was behind the seat headrests.
They opened the cabin door using the normal method and, in so doing, blocked the right forward cabin window exits.
The passengers, and the commander, exited the aircraft directly into the life rafts. The co-pilot jumped into the water, via his own door, then climbed into the left liferaft.
At no stage were the sea anchors deployed and, as the conditions were calm, the decision was made not to raise the covers of the liferafts.
The liferafts were in close proximity to the ETAP platform and the occupants could see the platform’s lights through the ‘fog’. They could also hear people on the platform shouting but, aware of the large amount of background noise on a working platform, they realised that the people on the platform could probably not hear them.
Several flares were fired. The Automatically Deployable Emergency Locator Transmitter (ADELT) or Crash Position Indicator (CPI) did not activate. 406 MHz distress signals from the TechTest 500-12Y Survival ELTs (ELTS) carried by crew and in the rafts were successfully received and logged by the COSPAS/SARSAT alerting system. The 406 MHz signal is sent in periodic burst and is not continuous, hence it is not suitable for homing. For that, a 121.5 MHz transmission is used.
No 121.5 MHz signal was detected by SAR aircraft as they approached the ETAP. The passengers had been equipped with ‘wristwatch’ Personal Locator Beacons (PLBs) that would transmit on the 121.5 MHz distress frequency c 5 nm. Unfortunately, in an unforeseen interaction, the more powerful Survival ELTs had a so called ‘smart mode’. This proved to be a misnomer in this case. It was designed to save battery life if multiple ELTs were active by not transmitting if another beacon was. In this case the low power wristwatch units supressed any Survival ELT 121.5 MHz transmissions.
Only after a period of 27 minutes, searching in the vicinity of the platform, was a faint location signal on 121.5 MHz detected.
It was said at post-accident industry debriefs that the Man Overboard (MOB) System on the ETAP did detect the adjacent wristwatch PLBs however.
The Survival ELTs had a voice capability but failed to allow communication with the SAR assets because this functionality depended on extending their antenna, which the crew and passengers were unaware of.
An RAF [Sea King] SAR helicopter, a Norwegian SAR helicopter, 2 Jigsaw SAR helicopters [operated for BP by Bond], 2 passenger helicopters, an RAF Nimrod aircraft, a [Jigsaw] RSV [Regional Support Vessel], 2 ARRC [Autonomous Rescue and Recovery Craft from the RSV] and several other ships were tasked into the area to assist with the search and rescue. The passenger helicopters made an initial sweep of the area then returned to their normal duties as the SAR helicopters approached the scene.
The BP Jigsaw project was an innovative combination of helicopter and marine SAR assets in place of transitional standby vessels. The project was ended in 2015 although a Central North Sea Industry SAR service continued in Aberdeen. The ARRCs are now better know as Border Force patrol vessels.
The Nimrod from RAF Kinloss had been about to conduct a training sortie (refreshing a crew that had been doing onshore support mission in Afghanistan with maritime patrol operations). It was tasked to be Aircraft Co-ordinator (ACO), an important task with 6 helicopters and several vessels responding in conditions of poor visibility in proximity to a large offshore installation. It arrived after the first helicopters and was unable to establish communications with some helicopters and establish the full air picture and provide an ACO service.
At 1957 hrs the first Jigsaw SAR helicopter located two liferafts in the water, approximately 400 m from the ETAP platform. They did so using a combination of radar, a very weak PLB homing signal, Forward-looking Infra‑red (FLIR) and visual guidance from personnel on the ETAP platform.
On arrival, they winched a member of the crew (the winchman) down to the liferafts to establish the number of survivors. The winchman was not equipped with a radio and had to be recovered back into the helicopter to confirm that all of the occupants of G-REDU were in the liferafts and accounted for.
The RAF SAR helicopter was the next SAR asset on scene, arriving as the winching operation commenced. It landed on the ETAP platform, from where its crew were able to observe the rescue. They also saw another helicopter which they were unable to contact by radio on any frequency, hovering in the fog behind the winching Jigsaw SAR helicopter. This helicopter is believed to have been the Norwegian SAR helicopter that had advised the ETAP platform that it was on scene.
The second SAR Jigsaw helicopter landed on a nearby rig to avoid adding to the congestion in the area of the rescue.
The winching operation was complicated by the fog and calm weather conditions in which the liferafts, without their sea anchors deployed, were being drifted by the helicopter’s downwash.
The equipment fit of the Jigsaw AS332Ls differed to that of the trial Jigsaw helicopter (the trial was conducted for BP by another operator) and crucially there was no pilot hoist controls which if fitted would have freed the hoist operator to assist with moving casualties into the helicopter. AAIB say that it was at this point “the crew discovered that it was difficult to winch two survivors simultaneously into the cabin, and were therefore restricted to winching one survivor at a time”. AAIB note that:
Jigsaw crews had been unable to practise winching from multi-seat liferafts due to the logistical difficulties the operator had experienced during its numerous attempts to set up the training. As a result, this was the first time that this crew had winched from a multi-seat dinghy. Furthermore, it was in the demanding conditions of a calm night, in fog involving a dinghy with no sea anchor deployed.
The close proximity of the ETAP platform was also a concern and, at one stage, the crew stopped the winching operation and used the helicopter’s downwash to blow the liferafts away from the legs of the platform.
At 2023 hrs the first of the ARRCs arrived at the liferafts and the Jigsaw SAR helicopter instructed them to complete the rescue. The ARRC recovered the 15 remaining survivors and the Jigsaw SAR winchman from the liferafts, having them all safely on board by 2028 hrs.
The SAR Jigsaw helicopter took its three survivors to the ETAP Platform and they were later transferred ashore by the RAF SAR Helicopter. The 15 other survivors and the Jigsaw helicopter winchman in the ARRC were transferred to their RSV [the Caledonian Victory] before also being taken ashore.
By the following morning the helicopter was capsized but it remained afloat. The tail boom had separated shortly after impact and sunk.
Aspects of the AAIB Safety Investigation
AAIB document an extensive investigation into the failure of the TAWS to give a 100 ft alert, but they were unable to identify a reason for its failure.
The final approach on the accident flight was compared with three previous platform landings, captured in the same CVFDR data recording, to establish how representative the visual perspective of the helideck in the windscreen was prior to the helicopter striking the surface of the sea.
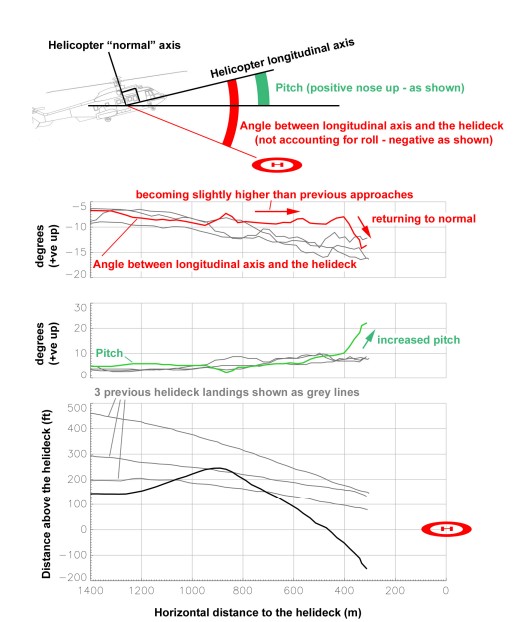
This study showed…
…that as the helicopter lost height the vertical position of the helideck in the windscreen became higher than on previous platform landings by an average of approximately 5° and that the pitch input towards the end of the flight path served to bring the visual angle back to normal.
Three reports were commissioned [by AAIB] to assess the possibility of illusions contributing to the pilots’ failure to detect the descent. The complete reports are included in Appendices A, B and C [of the AAIB final report].
These covered:
- Oculogravic illusions (a visual illusion that affects the apparent position of an object in the visual
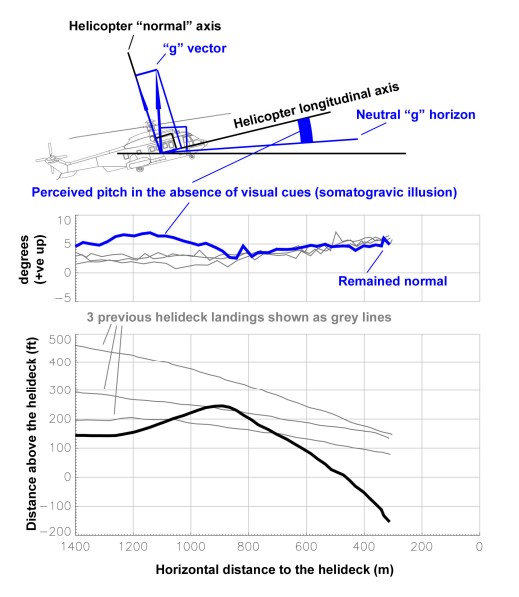
field) - Somatogravic illusions (a non-visual illusion that produces a false sensation of attitude)
- Visual perception (if the appearance of the platform and its reflection on the surface of the sea, diffused by the fog/reduced visibility, could have been confusing)
The somatogravic illusion is examined in this short SKYclip, which Aerossurance helped develop, available here:
AAIB note that “there was no visible horizon or surface texture and the appearance of the platform was ambiguous and confusing”.
Somato-sensory cues to orientation were also inadequate in providing them with a proper appreciation of the helicopter’s pitch attitude. As a result, increasing pitch was confused with, firstly, a stable approach angle and, secondly, with becoming high and fast in the final stages.
Also:
The helicopter manufacturer carried out simulation work to evaluate how the helicopter could have reacted had corrective actions been taken in response to a 100 ft callout during the final descent [if the TAWS had worked].
The simulation indicated that the helicopter could have climbed away and that the minimum clearance would have been 12 ft, with a pitch attitude of 12° nose up, giving a tail skid clearance of 8 ft.
AAIB caveat this by observing that it was dependent on the assumptions made (including pilot reaction times).
On TAWS, AAIB determined that:
The operator provided 33 crew safety reports related to TAWS, averaging one report every 123 flight hours. It was apparent that the majority of the reports were associated with problems with the system and not related to useful alert warnings generated by the system.
At the moment, the helicopter variant is much less mature, with much less operational data supporting it [than its implementation on fixed wing aircraft].
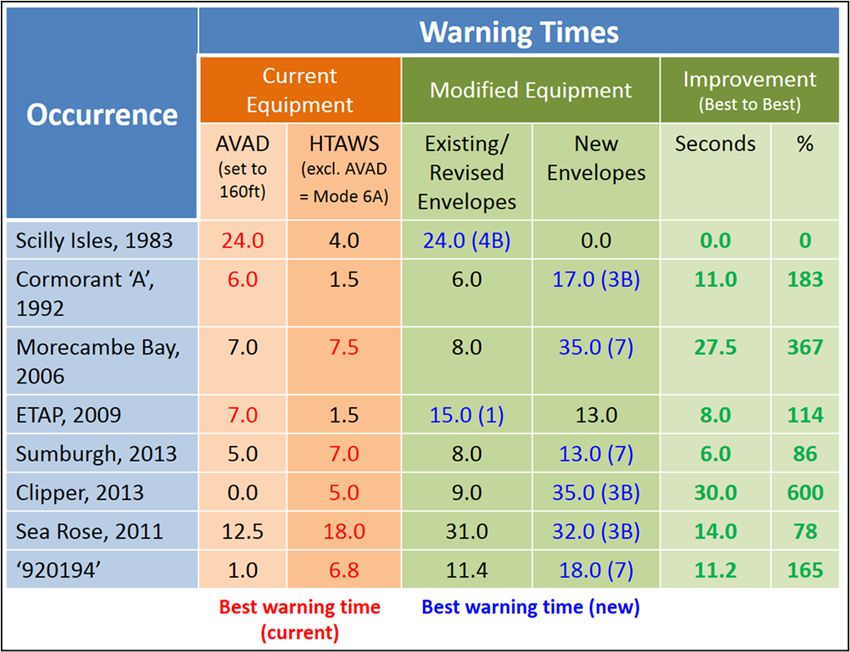
Subsequent research by UK CAA showed that AVAD could have given 7 s warning to the G-REDU crew vs just 1.5 s for TAWS. Improved TAWS envelopes could increase this to 15 s.
Observations
AAIB did not examine the actions taken by BP when introducing a new operator to both offshore crew change and provide the helicopter element of an integrated SAR service to replace the conventional stand-by vessels. After the G-REDU accident BP temporarily suspended operations with Bond’s EC225 but continued using their AS332L2s. However, on 1 April 2009 Bond AS332L2 G-REDL suffered a catastrophic main gear box failure with the loss of 16 lives. This resulted in BP suspending the use of Bond for 6 weeks.
The AAIB also don’t discuss how or when the UK CAA reviewed what operators had done in response to their 12 February 2007 letter to operators (discussed above) or their oversight of Bond more generally.
In evidence given to the G-REDL Fatal Accident Inquiry after another accident, the CAA stated that their flight ops oversight of Bond up to 1 April 2008 – 1 April 2009 consisted of:
- Audit/Inspection: 24 April 2008
- Annual Audit: 13 -15 May 2008 (which resulted in 1 x Level 1 Finding, 1 x Level 2 & 2 x Observations)
- Inspection: 19 June 2008
The 2009 CAA Annual Audit of Bond was delayed a months to 17 June 2009 because of the two AAIB investigations and “special BP audits” during BP’s 6 week suspension of operations.
With two accidents in the UK in 2009, the fatal loss of PHI Sikorsky S-76C++ N748P in the US on 4 January 2009 and the fatal loss of Cougar Sikorsky S-92A C-GZCH in Canada on 12 March 2009, 2009 was a dreadful year for offshore helicopter operations with 41 fatalities in these accidents alone.
Its also surprising that in 2009 the UK CAA did not launch the type of review that happened after the 23 August 2013 CHC AS332L2 G-WNSB fatal accident off Sumburgh that resulted in CAP1145 but waited for the third night operational accident since G-BLUN less than 7 years earlier.
AAIB Conclusions
The AAIB identified the following causal factors:
- The crew’s perception of the position and orientation of the helicopter relative to the platform during the final approach was erroneous. Neither crew member was aware that the helicopter was descending towards the surface of the sea. This was probably due to the effects of oculogravic and somatogravic illusions combined with both pilots being focussed on the platform and not monitoring the flight instruments.
- The approach was conducted in reduced visibility, probably due to fog or low cloud. This degraded the visual cues provided by the platform lighting, adding to the strength of the visual illusions during the final approach.
- The two radio altimeter-based audio-voice height alert warnings did not activate. The fixed 100 ft audio-voice alert failed to activate, due to a likely malfunction of the Terrain Awareness Warning System (TAWS), and the audio-voice element of the selectable 150 ft alert had been suspended by the crew. Had the latter not been suspended, it would also have failed to activate. The pilots were not aware of the inoperative state of the TAWS.
The AAIB also identified the following contributory factors:
- There was no specified night visual approach profile on which the crew could base their approach and minimum heights, and stabilised approach criteria were not specified.
- The visual picture on final approach was possibly confused by a reflection of the platform on the surface of the sea.
Safety Actions & Recommendations
Immediately following the accident involving G-REDU, the operator carried out a review of their offshore night approach procedures. As a result, the following requirements for offshore night operations were introduced and included in the company’s Operations Manual:
“For all Night operations over water, upper modes must be utilized in three or four axis coupled.
For operations at night crews shall carry out one of the following procedures: Airborne Radar Approach (ARA) Procedure OR Visual Gate Approach (VGA) Procedure.”
The AAIB provide more detail in their report.
One UK CAA initiative that was underway and came to fruition after this accident was the introduction of green ‘Circle and H’ lights to give a clearer indication of the helideck, and based on the shape that the circle was received to be. These are now a mandatory requirement for night operations in the UK sector. AAIB note that the CAA was scheduled for to present to the OGP Aviation Safety Committee [sic] in September 2010. IOGP adopted circle & H lights as a recommended practice 13 years later.
Another initiative was the analysis and optimisation of TAWS to increase its effectiveness for helicopters, and in particular offshore helicopters (discussed above).
In relation to survivability & SAR:
- North Sea Operators of EC225 helicopters have now fitted visual aids to indicate to passengers the location of the starboard main door jettison handle.
- The helicopter passenger safety briefing video has been modified to improve the way passengers are briefed on the location of the door jettison handles.
- BP improved the Jigsaw SAR helicopter capabilities by ensuring crews have multi-seat liferaft hoist training as a part of their SAR role currency.
- The Jigsaw winchmen were equipped with ‘wet fit’ radio.
- A pilot’s hoist control was embodied in the Jigsaw SAR helicopters.
- The RAF Kinloss Aeronautical Rescue Coordination Centre (ARCC) procedures were amended to apply for the establishment of a Temporary Restriction of Flying Regulation around any major incidents where more than two SAR helicopters are being tasked.
- The ‘smart’ capability was inhibited on the Survival ELTs and the PLBs withdrawn for a period.
Twenty seven safety recommendations were raised by AAIB.
Safety Resources
The European Safety Promotion Network Rotorcraft (ESPN-R) has a helicopter safety discussion group on LinkedIn. You may also find these Aerossurance articles of interest:
- South Korean Night Black Hole Spatial Disorientation Helicopter Fatal Accident
- Taiwan NASC UH-60M Night Medevac Helicopter Take Off Accident
- Night Offshore Take-Off Loss of Control Incident
- Technology Friend or Foe – Automation in Offshore Helicopter Operations
- The ‘Automation Problem’ – A Discussion
- HEMS S-76C Night Approach LOC-I Incident a near accident in Canada
- NH90 Caribbean Loss of Control – Inflight, Water Impact and Survivability Issues
- Korean Kamov Ka-32T Fire-Fighting Water Impact and Underwater Egress Fatal Accident
- AW139 A6-AWN Ditching off UAE, 29 April 2017
- NTSB Report on Bizarre 2012 US S-76B Ditching
- BK117 Offshore Medevac CFIT & Survivability Issues
- Night Offshore Training AS365N3 Accident in India
- In-Flight Flying Control Failure: Indonesian Sikorsky S-76C+ PK-FUP
- Loss of Control, Twice, by Offshore Helicopter off Nova Scotia
- NTSB Investigation into AW139 Bahamas Night Take Off Accident
- Helideck Heave Ho!
- Wrong Deck Landings
- Offshore Helicopter Emergency Response
- Fatal Offshore S-76C++ LOC-I & Water Impact Brazil 2022: CENIPA Investigation
- Offshore Night Near Miss: Marine Pilot Transfer Unintended Descent
- Automation Issues During Night SAR Training – Near CFIT
- Night Offshore Windfarm HEMS Winch Training CFIT
- North Sea Helicopter Struck Sea After Loss of Control on Approach During Night Shuttling (S-76A G-BHYB 1983)
- UPDATE 13 July 2024: Fatal USCG SAR Training Flight: Inadvertent IMC
- UPDATE 18 December 2024: Loss of Sikorsky S-76C+ 5N-BQG of Eastwind Off Nigeria 24 October 2024
- UPDATE 20 December 2024: 29 Seconds to Impact: A Fatal Night Offshore Approach in the Irish Sea
- UPDATE 8 February 2025: S-76D Loss of Control on Approach to an Indian Drilling Rig
- UPDATE 25 May 2025: CHC Sikorsky S-92A Seat Slide Surprise(s)
HeliOffshore has published a Flightpath Management (FPM) Recommended Practice (RP) for Offshore Helicopter Operations. The key elements of the FPM RP are embedded in the risk based controls within Flight Safety Foundation (FSF) Basic Aviation Risk Standard for Offshore Helicopter Operations (BARSOHO).
Another short SKYclip on somatogravic illusions is available here: