North Sea Helicopter Struck Sea After Loss of Control on Approach During Night Shuttling (S-76A G-BHYB 1987)
On 9 December 1987 Sikorsky S-76A G-BHYB of Robert Maxwell owned British International Helicopters, formerly British Airways Helicopters and later bought by CHC, contacted the sea during a night approach to the Shell Fulmar Alpha offshore installation in the Central North Sea.
The UK Air Accidents Investigation Branch (AAIB) safety investigation report explains that the helicopter, temporarily based on Fulmar Alpha, was shuttling maintenance workers between Fulmar Alpha and the Auk Alpha. Six 6 round trips (12 sectors) were planned that evening between the installations that are 6.4 nm apart.
On the fourth sector, whilst descending on an approach from a height of about 500 feet to the Fulmar platform and at about a quarter of a mile from the helideck, the aircraft lost all forward speed and entered a steep descent towards the sea.
At a very late stage, the co-pilot managed to arrest the descent just as the aircraft touched the water. The flight was continued to a normal landing on the Fulmar helideck.
While this accident is many years in the past and much has changed, the AAIB report does highlight a series of threats that are still relevant to offshore helicopter operations.

History of the Flight
The flight crew had been detached to Fulmar Alpha and were working a split shift:
The duty day began at 0600 hrs and ended at approximately 2000 hrs, and included a “split-duty” rest period between 0745 hrs and 1745 hrs.
Both pilot’s had the rank of Captain and so “and it was decided between them who was to be commander”.
Because the prevailing wind dictated that all the approaches would be made from the left side of the helidecks, it was also decided that the commander, [seated] on the right side of the aircraft would be the handling pilot [to use the terminology of the time] throughout. The pilots remained in these respective roles throughout the evening’s flying.
The Aircraft Commander was 47 and had 6540 hours of flight time, 870 on type. He was…
…very enthusiastic about physical fitness and had taken part, with notable success, in both physically and mentally demanding television and social competitions. During the day on which the incident occurred, he had, most unusually, lost several recreational games.
The Co-Pilot was 39 and had flown 5662 hours, 518 on type.
The fourth sector, with 8 passengers, commenced at 18:43.
The weather that evening was well within the requirements for a visual flight and approach to the platforms, the wind was 3500/11 kt, the visibility unlimited and the cloud 4 octas at 2500 feet. Although the sky was nominally less than half obscured by the cloud, it was totally dark, and this darkness was emphasised by contrast to the platform illuminations. On the approach from the south, no other platform or rig was visible to the crew and the sole source of visual reference was the brightly illuminated platform, with its attendant brilliant and pulsating flare.
AAIB observe that:
…the flare…together with the platform’s working lights, combine to produce a significant contrast to the otherwise dark environment.
The short cruise was conducted at about 140 kt, at an altitude of 500 feet. Deceleration commenced about 1 nm from the destination and abeam a Fuel Storage Unit (FSU) vessel moored in the field.
Up to this point, the flight had been normal and the co-pilot had been preparing the necessary paperwork for that sector and the next. At some point during the deceleration, approximately 1/4 nm from the platform, all forward speed was lost and a very high sink rate was established. Replay of the cockpit voice recorder (CVR) showed that, during this descent, the two automatic voice alerting device (AVAD) warnings sounded, activated by the radio altimeters, but the crew have stated that these were not heard.
A failure for flight crew to perceived aural alerts is not uncommon (see the investigation into the incident involving G-WIWI with Paul McCartney aboard) and is the subject of CAP1747: Class A HTAWS Warning Annunciation.
The AVAD provided “CHECK HEIGHT” and “100 FEET” warnings. The former could be set by the crew but in this case it was set, for reasons discussed below, to factionally below 100 feet and so the “100 FEET” warning came momentarily before “CHECK HEIGHT”.
The AAIB noted that while there was little relevant discussion by the flight crew prior to the AVAD warnings…
…the co-pilot has since stated that he noticed the speed to be very low at about 350 feet, but, in the 2-3 seconds before contact with the sea, the co-pilot queried the commander’s appreciation of the situation and then applied a large amount of power, by raising the collective pitch lever, thereby causing the impact with the sea to be so slight as to result in no structural damage to the helicopter.
The necessary severity of this lever application, although causing the rotor rpm to drop from the indicated 100% to slightly less than 79%, enabled the aircraft to make an almost immediate lift-off from the water.
The helicopter struck the water almost vertically, with no forward speed and the water contact caused no damage to either the airframe or the engines. However, minor bruising of the rotor spindle assemblies occurred as a result of the sudden and severe application of rotor pitch applied in an attempt to prevent the incident
Following the lift-off, the commander stated that he had become “disorientated” and so the co-pilot, being unsure whether the commander was yet fully aware of the situation and having established the aircraft in a climb, remained on the controls and initiated a right hand circuit to the east of the platform. However, as the climb progressed, he felt the commander come back onto the controls, saying again that he had become “disorientated” but now felt “fine”. Nevertheless, the co-pilot followed through on the controls whilst the commander carried out a normal landing on the Fulmar helideck.
On landing the Helideck Landing Officer (HLO) noticed what turned out to be seawater pouring from the aircraft. No one was injured.
Following the landing and the disembarkation of the passengers, the commander stated that he had become “mesmerised” and had seen two rigs, side by side.
The AAIB Safety Investigation
The S-76A was certified for single pilot operations and was being operated as such in the North Sea at the time. However, Shell had contracted that there “be two pilots on board during all their IFR and night flights”. The helicopter operator had not however developed multi-crew procedures as they reportedly felt ” it might be dangerously confusing for a given pilot to have to cope with two sets of operating procedures for the same aircraft”. There was a requirement for the Commander to brief the Co-Pilot prior to an approach, but that did not occur during these repetitive shuttling flights. Consequently the AAIB concluded that the helicopter was…
….operated in a manner very little different from a single pilot operation.
Today, the Flight Safety Foundation (FSF) BARSOHO offshore helicopter Safety Performance Requirements, which align with the risk-based HeliOffshore Safety Performance Model, contains a specific control (1.5) on Multi-Crew Operations and another (3.1) on Flightpath Management. These incorporate the HeliOffshore Flight Path Management recommended Practices.
While the operator’s Ops Manual fully documented the actions to be taken in the event of subtle incapacitation of the handling pilot, “there are very few cues” in an event such as this to alert the non-handling pilot to that possibility.
At the time a Flight Data Recorder (FDR) was not a regulatory requirement and none was fitted. The lack of FDR data…
….severely hampered the capability of the investigation to define either the sequence of events, or possible failures. Had a fatal accident occurred, this lack of FDR data would have made determination of the cause unlikely.
Consequently the AAIB made a safety recommendation that resulted in a change in regulations. A Fairchild A100 magnetic tape CVR was fitted:
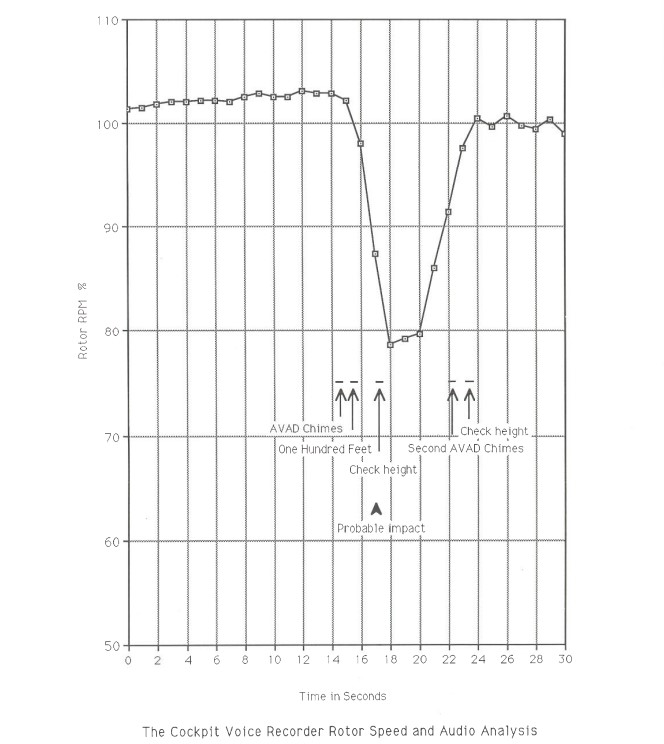
Analysis of the rotor rpm track showed a drop in rotor rpm from 103% just before the helicopter contacted the sea, to a minimum value of 78.7% probably due to the large collective input demanded. The drop in rotor rpm lasted for approximately 9 seconds before the rotor speed returned to 100% as the helicopter climbed away.
From the CVR it was not possible to identify exactly the point at which the helicopter contacted the sea, however a change in the amplitude of the signal on the area microphone track occurred 2.5 seconds after the chimes [that immediately preceded the aural AVAD warnings] were heard, and this is thought to be the point at which impact took place.
The recorded rotor speed had been 100 to 101% until approximately 23 seconds before the chimes were heard, when a gradual increase in rotor speed occurred, with a maximum of 103%, indicative of a power-off condition.
The AAIB comment that:
Approaches to helidecks, particularly at night, require a very high degree of precision. Standardisation of approaches is a clear objective and, despite the many factors of weather and visual assessment which work against it, training is carried out with this in mind.
However, each pilot interviewed, formally or otherwise, during the investigation…declared his own method of approaching a helideck, and there appeared to be little standardisation of planned approach paths.
A number of Mandatory Occurrence Reports (MORs) had been raised that highlighted occasions when….
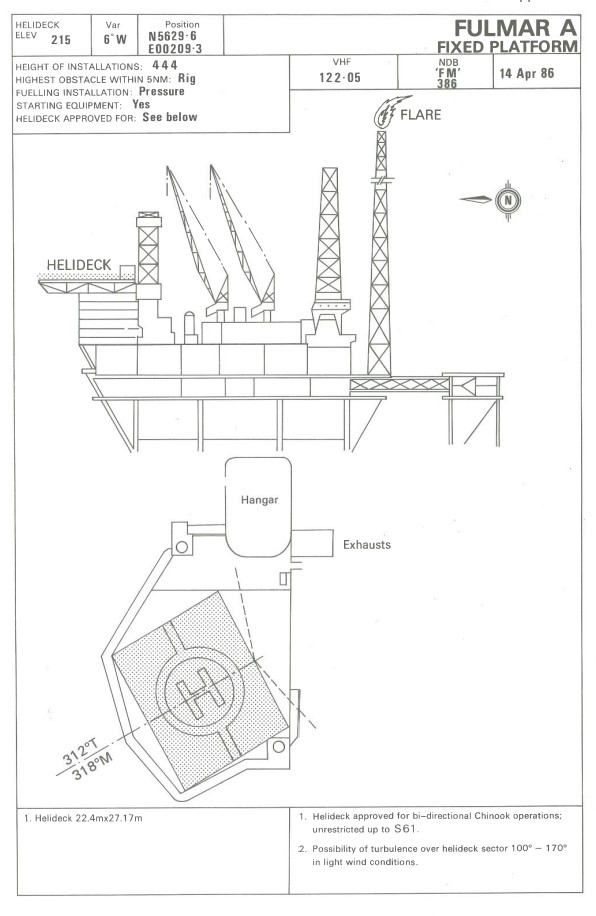
…the heat generated by the platform’s flare has produced a micro weather system in the form of a heat engine. The very strong downdraughts which can be produced by this mechanism can persist over a considerable distance down wind of the flare, in the area from which most approaches to land are made. On one occasion reported, the downdraught exceeded the helicopter’s climb capability.
Another difficulty [is that an installation] may be the only light source in an otherwise totally dark environment. The single light source phenomenon has long been recognised by the aviation community as one which contributes nothing to the pilot’s judgement of distance from it. In this context, although the rigs and platforms have considerably more than one light, when viewed from a distance, they may be considered as a single light source. The usual effects of this phenomenon are that the pilot is deprived of the visual cues normally associated with daylight vision:
(1) The relationship of the object to the horizon;
(2) Other objects and the surface texture between himself and the object in view;
(3) The use, for ranging, of the angle subtended at the viewer’s eye by the object, because;
(a) The absolute size of the object is uncertain and;
(b) The judgement of this angle when it is very small is difficult.
However, as the approach to the Fulmar platform was initiated at a little over 1 nm and beside the well lit FSU and tanker, it is unlikely that this phenomenon had any appreciable effect during the night in question.
Finally, whilst the brilliance of the flare might be slightly dazzling to the pilot, it does provide a quite bright illumination of the whole structure and the sea surface immediately surrounding it.
This accident is cited by UK CAA as one of three accidents (including AS365 G-BLUN and EC225 G-REDU) that justify the development and implementation of helideck circle and H lights as described in CAP1077: Specification for an Offshore Helideck Lighting System
Medical examination of the Aircraft Commander…
…did not suggest any pre-existing mental or medical condition likely to cause the commander’s disorientation. However, the tests did reveal a latent tendency to squint but, whereas this was so slight and normal as to have no effect upon his suitability to exercise the privileges of a flying licence, it could possibly contribute to the occurrence of double vision in certain circumstances of reduced mental awareness.
To better understand the circumstances of the accident two flights to Fulmar Alpha in another S-76A were conducted, first with an AAIB Inspector and then with the Head of the Flight Skills Section of the RAF Institute of Aviation Medicine (IAM) in the co-pilot seat. These were to…
…investigate the effects of various types of approach, with the intention of finding one which, as closely as possible, matched that of the incident aircraft.
A number of abnormal approaches were then made. When the undercarriage selection point was delayed, only a few seconds of delay had an appreciable effect on the degree of power reduction needed to arrive alongside the platform at the speed required to achieve a landing. The same effect was also noted when the descent was either delayed or steepened. In most of the abnormal approaches demonstrated, the torque had to be reduced to nearly zero in order to achieve the desired arrival at the helideck.
It was also apparent that considerable anticipation of the large amount of power needed to regain level flight was required in these circumstances. Furthermore, any delay in its application produced a more rapid onset and greater degree of downwards vertical acceleration.
It was also observed that visual assessment of distance from the platform was very difficult, but that the visual cues as to aircraft height, with reference to that of the helideck, was not. The prime reason for this is that the platform is built in storeys, well illuminated by linear rows of lights. When looking along the side of the structure, particularly from below the level of the platform, the sight of passing downwards, from being aligned with one storey to the next lower one, provided a strong clue to descent and descent rate.
AAIB Analysis: Conduct of the Flight & AVAD
The AAIB highlight three key factors:
- the loss of speed
- the loss of height
- the delay before either crew member noticed these.
The flight tests showed that, for the aircraft to have decelerated from its 140kt cruising speed to the final manoeuvring speed alongside the platform in about 0.75 nm, the collective lever must have been lowered almost completely. Therefore, as the speed reduced, the power should have been restored in time to anticipate the consequent loss of lift, and thus to reduce the rate of descent.
A significant observation was that:
[Main rotor speed] was increasing for 14 seconds before the sudden lever application. With the lever down or nearly down, this increase in rotor rpm could be caused by either a flare manoeuvre or an increasing rate of descent in autorotation. However, as both pilots have stated that no such flare occurred, it is most likely that the increase in rotor rpm occurred as a result of autorotational forces, which therefore marks the beginning of the severe accelerating descent rate, 17 seconds before impact with the water.
As no evidence was found to suggest any malfunction of the aircraft or its systems, the reason for the descent rate demonstrated in the incident must be attributed to either a downdraught which exceeded the helicopter’s climb capability, and/or to the actions of the handling pilot. Had a significant downdraught, caused by the flare, been the only reason for the descent, firstly it is unlikely that all forward speed would have been lost and secondly, it is almost certain that the commander would have made some comment to the co-pilot, which he did not. However, the possibility that it contributed to the rate of descent cannot be ruled out.
The AAIB comment that the Ops Manual contained no procedures for the use of the AVAD during visual approaches and the system “was not being used in a manner advantageous to flight safety”.
Given the environmental workload that is typical of oil field Shuttle flights, it is surprising that crews should have arranged their handling of this system such that it could provide no effective warnings at all. The subject incident would, most likely, not have occurred had the co-pilot’s altimeter bug, to which the AVAD was slaved, not been set at a height below that of the helideck [which was 215 ft].
The declared reason for this usage was that the repetitive warnings, occasioned by ‘bugging’ a height greater than that of the helideck, were more of an irritation than a safeguard.
AAIB Analysis: The Crew
It is probable that when the commander used the terms “mesmerised” and “disorientated”, he did so in a conversational way, rather than as a clinical description… However, the fact that he did suffer such an event is supported by other evidence.
Firstly…he remembered…he was able to see a double image of the rig with both images in clear focus, but had no visual memory of the descent to the water.
Secondly, the fact that he failed to respond to the AVAD warnings and, finally, the statement of the co-pilot that, during the short descent to the water, the commander appeared “frozen” and unresponsive.
As the neurological, ophthalmological and medical examinations revealed no significant abnormalities, it is left to analysis of the psychology behind his behaviour to try to explain the events which occurred. The report on this examination,…although unable to identify any specific cause for it, strongly suggests that he did suffer a temporary incapacitation [and so] the uncontrolled descent and the absence of forward speed can be attributed only to a lack of anticipation of the required power increase as the aircraft reduced speed.
The French Bureau d’Enquêtes et d’Analyses (BEA) recently reported on a case where the Pilot Flying of Airbus A350-900 F-HREV, operated by French Bee, suffered a cognitive incapacitation on approach to Paris Orly. We recommend their VIDEO.
The S-76A’s non-handing pilot was expected to monitor the flightpath to detect deviations.
In this case, the monitoring was successful only to the extent that the severity of the impact was considerably reduced by the actions of the co-pilot.
The co-pilots observation of low speed when passing through 350 ft was described by AAIB as ‘peripheral’ rather than flightpath monitoring as such. The available…
…indications of departure from the normal flightpath…were the decrease in height shown on both radio and pressure altimeters, an increasing rate of descent on the vertical speed indicator, an indicated pitch attitude dissimilar to that of normal flight, an airspeed unlikely to be normal except when directly abeam of the platform (when the latter is definitely in view) and finally, the relationship between this lack of airspeed and the absence of engine torque. Nevertheless, it would appear that during the 14 seconds before power was re-applied these indications passed unnoticed.
The AAIB observer that certification requirements assumed one second for recognition of a problem and a further one second for action to be taken. Hence, a 12 second delay “does seem to be rather a long time”. They postulate that “the co-pilot may well have felt disbelief upon seeing what was happening and thus taken longer than expected to rationalise and act upon it”.
The co-pilot’s subsequent actions however were considered to have prevented a major accident and the AAIB recommended the UK CAA consider requiring two crew.
AAIB Conclusions
- The Commander suffered a temporary incapacitation.
- The co-pilot’s response to the emergency situation was delayed partially by insufficient flightpath and instrument monitoring and partially by the difficulty of appraising the situation. The proportion of each is not known.
- The company Operations Manual contained no procedures for the use of the Automatic Voice Alerting Device during visual approaches
Footnote
Curiously, this helicopter, when registered as C-GIMR, was destroyed while being operated as an air ambulance in Ontario by Canadian Helicopters on 8 February 2008. The Transportation Safety Board of Canada (TSB Canada) concluded in their safety investigation report that:
- The pilot flying (PF) was likely affected by visual spatial disorientation and perceived the approach height of the helicopter to be too high. While correcting for this misconception, the helicopter descended into trees 814 feet short of the helipad.
- The pilots were likely distracted during the critical phase of the approach and did not identify that the helicopter had deviated from the intended approach profile and recommended descent rates.

Safety Resources
The European Safety Promotion Network Rotorcraft (ESPN-R) has a helicopter safety discussion group on LinkedIn. Having sponsored their 2021 online event, we will be attending the OEUK Aviation Seminar in Aberdeen on Tuesday 7 June 2022.
You may also find these Aerossurance articles of interest:
- HeliOffshore 2022 Conference Review
- Loss of Control, Twice, by Offshore Helicopter off Nova Scotia
- Offshore Night Near Miss: Marine Pilot Transfer Unintended Descent
- Technology Friend or Foe – Automation in Offshore Helicopter Operations and Aerossurance Marks RAeS 150th Anniversary by Sponsoring Rotorcraft Automation Conference
- AAIB Report on 2013 Sumburgh Helicopter Accident
- SAR Helicopter Loss of Control at Night: ATSB Report
- NTSB Investigation into AW139 Bahamas Night Take Off Accident
- Night Offshore Training AS365N3 Accident in India 2015
- BFU Investigate S-76B Descending to 20ft at 40 kts En Route in Poor Visibility
- Review of “The impact of human factors on pilots’ safety behavior in offshore aviation – Brazil”
- HEMS S-76C+ Night Approach LOC-I Incident
- NH90 Caribbean Loss of Control – Inflight, Water Impact and Survivability Issues
- Helideck Heave Ho!
- Strictly Scheduled: S-92A Start-Up Incident
- 2009 Newfoundland S-92A C-GZCH Accident: A Failure of Design and Certification
- ADA AW139 A6-AWN Ditching off UAE, 29 April 2017: Final Report
- Night Offshore Windfarm HEMS Winch Training CFIT
- NTSB Report on Bizarre 2012 US S-76B Ditching
- Sikorsky S-92A Loss of Tail Rotor Control Events
- S-92A Emergency Landing: MGB Oil Checklist Recommendation
- Loss of Bell 412 off Brazil Remains Unexplained
- RLC B407 Reverses into Sister Ship at GOM Heliport
- CAP1145 Helicopter Water Impact Survivability Statistics – A Critique
- Hong Kong Harbour AW139 Ditching – HKCAD Report Issued
- Dramatic Malaysian S-76C 2013 Ditching Video
- In-Flight Flying Control Failure: Indonesian Sikorsky S-76C+ PK-FUP
- Safety Lessons from a Fatal Helicopter Bird Strike: Sikorsky S-76C++ N748P, 4 January 2009
- S-92A Collision with Obstacle while Taxying
- Troublesome Tiedowns
- Helideck and Helicopter Egress Training Facilities
- Wrong Deck Landings
- FOD and an AS350B3 Accident Landing on a Yacht in Bergen
- Helideck Lightning Strike: Damage Missed
- Offshore Helicopter Emergency Response
- UPDATE 28 December 2022: Night Mountain Rescue Hoist Training Fatal CFIT
- UPDATE 7 January 2023: Blinded by Light, Spanish Customs AS365 Crashed During Night-time Hot Pursuit
- UPDATE 8 July 2023: BK117 Offshore Medevac CFIT & Survivability Issues
- UPDATE 16 July 2023: SAR AW139 LOC-I During Positioning Flight
- UPDATE 17 February 2024: Night Offshore Take-Off Loss of Control Incident
- UPDATE 18 February 2024: Night Offshore Helicopter Approach Water Impact
- UPDATE 18 December 2024: Loss of Sikorsky S-76C+ 5N-BQG of Eastwind Off Nigeria 24 October 2024
- UPDATE 20 December 2024: 29 Seconds to Impact: A Fatal Night Offshore Approach in the Irish Sea
- UPDATE 8 February 2025: S-76D Loss of Control on Approach to an Indian Drilling Rig
- UPDATE 25 May 2025: CHC Sikorsky S-92A Seat Slide Surprise(s)