SAR Helicopter Loss of Control at Night: ATSB Report
19 April 2020
SAR Helicopter Loss of Control at Night: ATSB Report (Careflight AW139 VH-YHF near Darwin, NT)
On 13 May 2018 Leonardo HelicoptersAW139 VH-YHF of HEMS operator Careflight, while descending during a nighttime search, the aircraft entered a degraded visual environment, developed a high rate of descent, an autohover mode was inappropriately selected and came within 31 ft of impacting the ground. The aircraft was also then flown on for one more flight after the related 159.5% over-torque. We look at the Australian Transport Safety Bureau (ATSB) safety investigation report issued 16 April 2020.
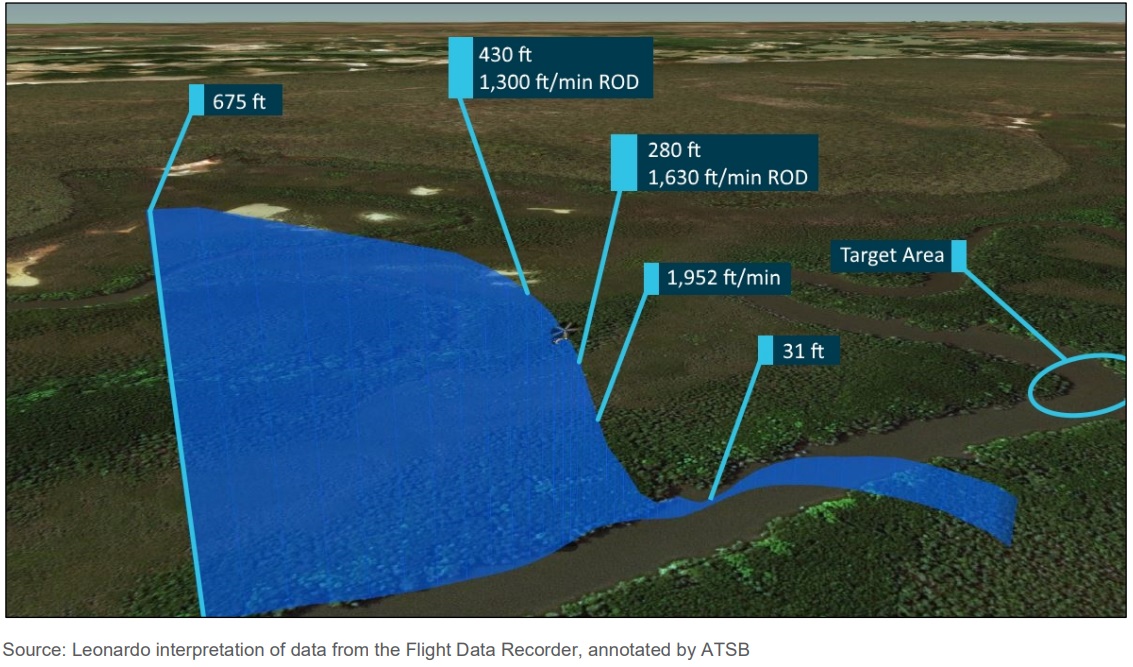
Flight Path Careflight AW139 VH-YHF During Night SAR LOC-I (Credit: ATSB / Leonardo)
The SAR Tasking, Aircraft Equipment and Preparations
The aircraft was operated single pilot (front right seat), an ‘ Aircrew Officer (ACO)’, a dual qualified winch op and winchman (right hand cabin doorway) and a ‘Flight Nurse’ (rear of the cabin), who was “not expected to be involved in the operation of the aircraft in flight”. The Pilot and ACO were equipped with AN/AVS-9 green phosphor Night Vision Goggles (NVGs). The ATSB explain that the rest of the Night Vision Imaging System (NVIS):
• NVG-compatible cockpit lighting
• NVG-compatible cabin lighting
• 2 x 450 W incandescent forward facing steerable search lights
• 1 x 450 W incandescent steerable search light by winch
• White flood lights at the front and back of the aircraft.
The operator required the use of NVIS for all visual flight rules (VFR) flights at night.
The Civil Aviation Safety Authority (CASA) provided the Operator with an exemption to Supplement 60 of the AW139 rotorcraft flight manual. The exemption allowed the ACO to operate from the rear cabin of the aircraft during flight below 300ft and for landing at unimproved sites.
The Operator listed the responsibilities of an ACO in their operations manual as “Under direction of the pilot assist with the operation of all aircraft equipment and systems during the conduct of VFR, NVG and IFR operations” and “operate the winch, dispatch, and recovery of personnel and assist the pilot in maintaining clearance from obstacles by lookout and reporting over the intercom”.
The ACO was expected to work from both cockpit and cabin. CASA’s position was that “they supported the role of the ACO in the front left seat” and “preferred operators to land” for the ACO to transfer positions, but ‘climb-throughs’ did occur. The operator seems to have recognised this risky manoeuvre was unusual as everyone had to be reported. ATSB state that the crew believed the tasking would “most likely” need use of the hoist, and so with a nearby search area with limited landing opportunities the ACO was in the cabin.
ATSB note that:
The helicopter’s autopilot was a 4-axis system with enhanced 3-cue flight director (FD). The FD is capable of controlling the helicopter’s movement in the pitch, roll, yaw, and vertical axis. The installed version of the FD had auto-hover functionality (HOV) mode, yet did not offer SAR modes that can mark, return, and transition down to a selected target.
Engaging the system instructs the autopilot to make control inputs to bring the aircraft to a hover at the height showing on the RADALT at the time the pilot presses the switch.
The manufacturer did not intend for HOV mode to be engaged with a high vertical speed, though it did not preclude a pilot from doing so. If engaged with a high vertical speed, the system would show as engaged and the autopilot would make adjustments necessary to attain the height designated by the pilot. This would induce a magnitude of overshoot relative to the vertical speed at time of engagement.
Conduct of the Incident Flights
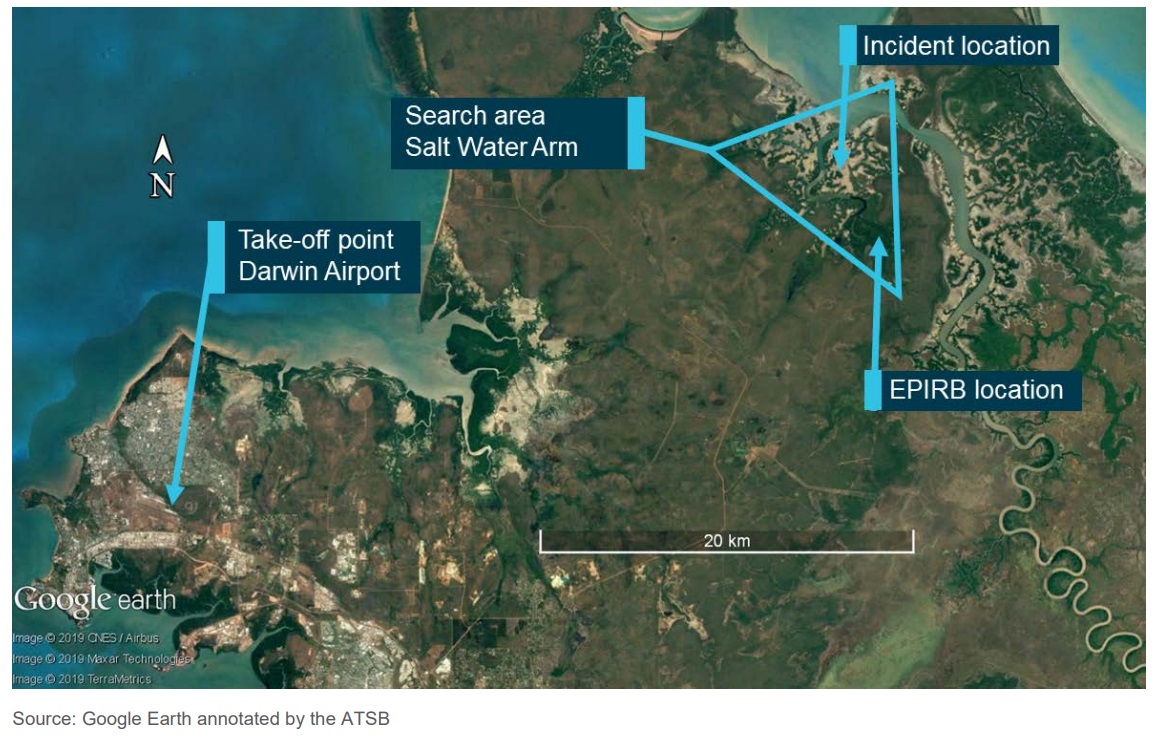
At about 2000, the crew departed Darwin Airport with good visibility. At that time, a five-metre tide was receding from Salt Water Arm.
Search Area (Credit: ATSB)
There was little illumination as the moon had set at 1653, and the sun had set at 1830. There was limited celestial light available through the gaps in the clouds which were forecast as scattered cumulus and stratocumulus clouds at 2,000 ft, with cloud tops to 10,000 ft. Smoke from outlying grass fires drifted across the search area below 7,000 ft, reducing visibility to 4 km in places. The crew could not easily detect the smoke due to low illumination.
As the crew arrived and commenced the search, smoke became evident.
The ACO described visibility as 5 km but dropping in and out due to large amounts of smoke. These conditions are common for the region, and recent check flights for the crew had been conducted in similar conditions. During the flight, the beam of the search light would reflect off smoke and ash. Backscatter from the beam was affecting visibility, reducing NVG image quality, and reducing peripheral vision. As a result, the beam required frequent adjustment. The ACO contacted the RCC and advised that limited visibility may hamper the operation.
Direction Finding readings from the EPIRB were erratic so locating the beacon was problematic. The crew conducted a visual search from 800 ft above ground level (AGL) but to identify a potential target while using NVG, needed to descend to 400 ft AG.
The company operations manual highlights three critical instruments for the initial stage of the approach:
• attitude indicator, to avoid incorrect attitude adversely affecting airspeed and rate of descent
• vertical speed indicator, to make up for the reduced visual cues for rate of descent
• radio altimeter, to incorporate a visual and audible warning that is set at 400 ft as a defence against unexpected rates of terrain closure.
The crew flew the descent to the target visually, using searchlights to ensure the approach and departure paths were clear of obstacles. The intent was to decrease rate of descent and airspeed before activating auto-hover (HOV) mode at 400 ft AGL.
At 2110:30, the crew commenced an approach from the north to a point of interest in Salt Water Arm. The pilot reported visibility on approach to the target as good to the north-west, and dark to the north and east. During this approach, the pilot lost visual references.
Critically:
At 2110:40, the pilot activated HOV mode. At this time, the helicopter had already developed an undesired high rate of descent.
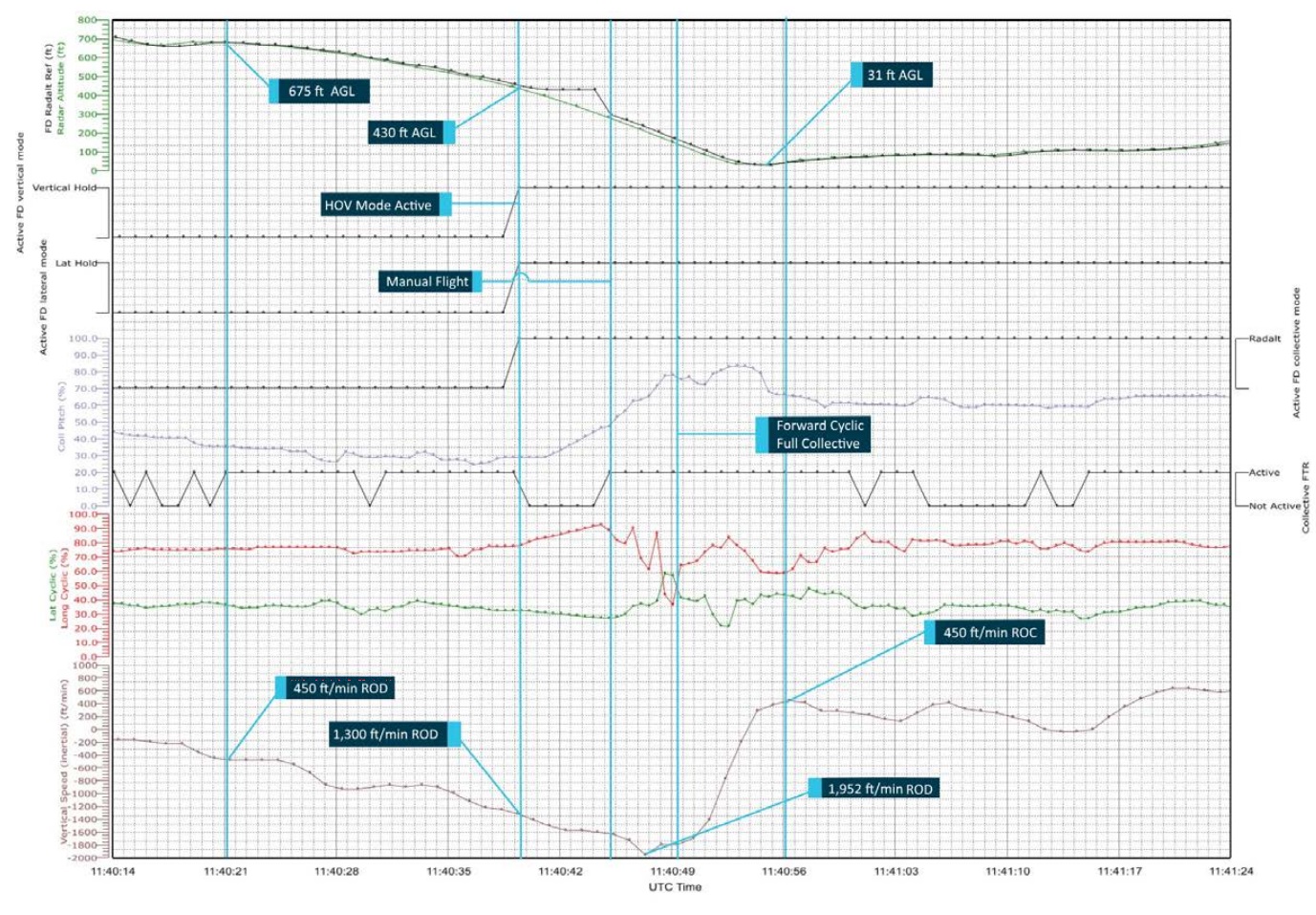
FDR Careflight AW139 VH-YHF During Night SAR LOC-I (Credit: ATSB / Leonardo)
At the point of activation of HOV mode, the aircraft was at 430 ft, pitched 19.7 degrees nose-up, and descending at over 1,300 ft/min with a ground speed of 14 kt. The autopilot increased collective pitch to 48 per cent to arrest the rate of descent.
The ACO had a better view of the ground below and advised the pilot of a high rate of descent.
The ACO provided advice twice more to the pilot before transitioning to an emergency call of ‘Climb! Climb! Climb!’ The pilot was by now receiving clear visual cues and detected a rapid rate of closure with the ground.
At 2140:46, at a height of 280 ft with a rate of descent of 1,630 ft/min…the pilot overrode aircraft automatics and used forward cyclic and collective to reverse the rate of descent. The pilot directed his attention to the attitude indicator and the picture outside. The pilot increased collective pitch to 77 per cent. At this point, the rate of descent increased to 1,952 ft/min, indicative of onset of vortex ring state.
Occupied with the recovery procedure, the pilot flew solely through the outside picture and the attitude indicator. The aircraft descended to a height of 31 ft AGL before attaining a positive rate of climb.
The pilot had notice an Amber caution light but this extinguished before he had chance to read the caption. The ATSB opine that any further delay overriding the autopilot would have been catastrophic.
The aircraft landed back at base at 21:58 and the crew debriefed. As they thought that a Main Gearbox (MGB) overtorque may have occurred, they called an engineer (seemingly on call but off-site).
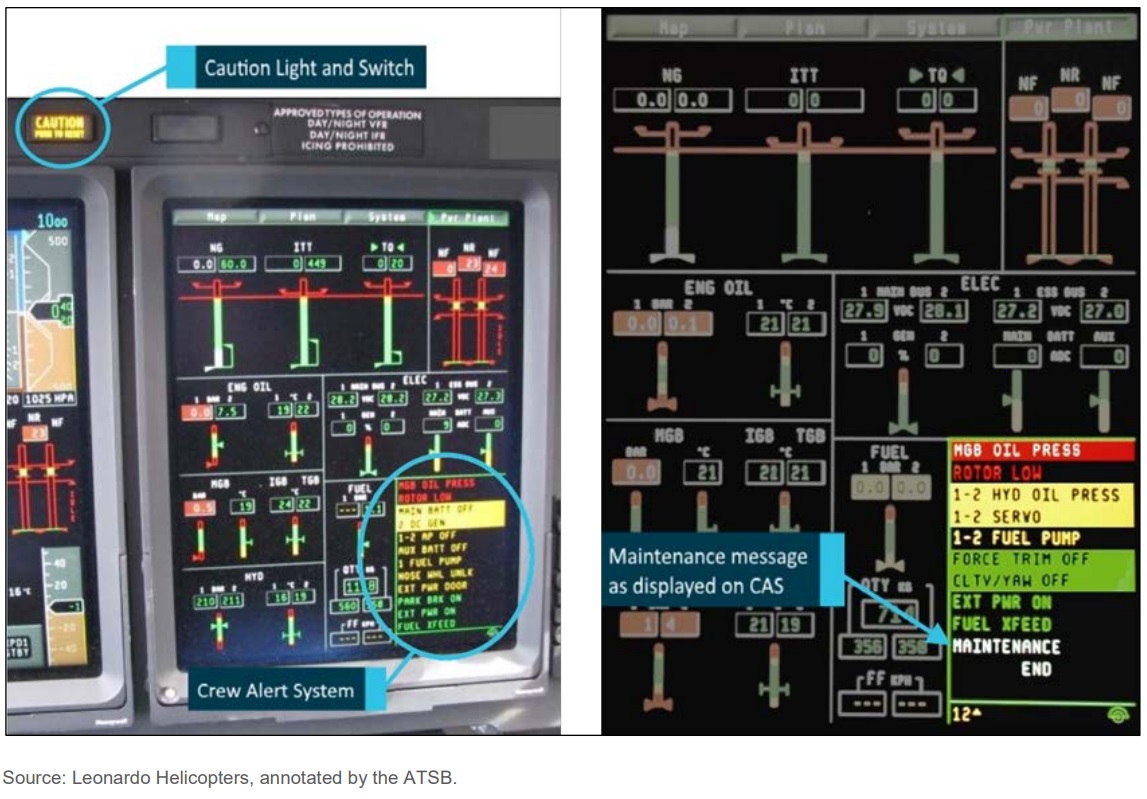
The duty engineer asked the crew to check the CAS system for messages. If an overtorque occurred, a white status message saying “MAINTENANCE” would be present. This would signal a requirement to download and analyse data from the aircraft’s central maintenance computer (CMC).
Example AW139 Maintenance Message (Credit: Leonardo / ATSB)
The “MAINTENANCE” message is significant because following exceedance of a limit such as torque, it will illuminate after landing. The presence of the “MAINTENANCE” message is a cue to an aircraft maintenance engineer (engineer) to investigate and rectify the cause of the message before cancelling the message.
The ATSB say “the pilot estimated the extent of a potential over-torque to be within operational limits”, without any indication why that was considered likely. The crew did not detect a maintenance message, for reasons the ATSB don’t explain, so the engineer advised no further action was required.
The crew then briefed for a second flight to complete the tasking, adopting a different search strategy. They departed at 22:54 and flew along the river’s tributaries at 1,000 ft using the autopilot, with the pilot on instruments and the ACO visually searching from the cabin.
A 14 ft metal hulled boat with two occupants was detected in complete darkness and an a Northern Territory Water Police vessel vectored to the scene.
Detecting the Over-torque
The next day the crew asked an engineer to download the CMC. The limits for all engines operative are 110% for 5 minutes and 121% for 5 seconds. He found that a:
…main gearbox over-torque to 159.5% had occurred during the first flight.
The extent of the over-torque was such that the helicopter should not have been flown until the engine and airframe manufacturers declared the helicopter serviceable. This meant that the crew had departed for their second flight of the previous evening in an aircraft of uncertain airworthiness.
Five days later, the engine manufacturer confirmed that the engines were undamaged and suitable for service. The helicopter manufacturer advised that the helicopter’s main gearbox was serviceable and required inspection of oil for metal contamination at 50 flight-hour intervals. The engineers carried out the necessary actions, and subsequently returned the helicopter to service.
Risk Management of Deteriorating Weather and Loss of Visual References
The operator recognised the risk of deteriorating weather and loss of visual references during a SAR flight and that this could result in a loss of control leading to an aircraft accident. Controls for the prevention of loss of visual references were:
Training and checking, to ensure that crews have relevant experience of similar conditions, all crew know how to assist in the approach and landing phase, and that procedures are being correctly followed.
Maintenance of good CRM, to ensure effective mission management and decision making aboard the aircraft.
Keeping the ACO current to assist the pilot with management of the flight.
Their recovery controls were:
Equipment fit, ensuring that the aircraft is appropriately equipped and has a functioning RADALT and Attitude Indicator.
Sound knowledge of procedures and limits for visual illusions and inadvertent instrument meteorological conditions (IIMC).
Crew preparedness: Use of simulator training to ensure crews have exposure to implementing correct technique in recovery procedures.
Crew Resource Management: Ensuring unambiguous and timely communication in situations requiring urgent action.
ATSB Safety Analysis: Operator’s Risk Management
There were…gaps in the implementation of all of the documented controls:
• Training and checking achieved the aim of creating relevant experience, yet an identified limited practice opportunity reduced efficacy.
• Crew resource management (CRM) lapsed in a missed announcement of loss of visual references. CRM was, however, restored to good effect in recovery.
• The aircrew officer (ACO) was trained yet not positioned to assist the pilot in managing the approach.
There were no preventative controls that helped crews to define limits of visibility beyond the description of visual flight rules (VFR) minima.
The operations manual stated: “Illumination levels are significantly affected by moon position and strength, cloud presence, and cultural lighting and during NVG operations; illumination levels have a profound effect on the ability of the NVG to clearly discern terrain at distance. Visibility is also affected by the usual day time issues of dust, snow, moisture, bushfire smoke and other atmospheric obscurants”.
However, the operations manual offered no guidelines on interpretation of factors affecting visibility or definition of acceptable limits. This meant the crew had to interpret marginal conditions during operations and decide if the minima were sufficient. This meant that the organisation did not set its own tolerance for risk in this regard.
During the event, CRM, the well-rehearsed recovery drill, and use of the attitude indicator were all vital in recovering control of the aircraft. The documented and implemented recovery controls worked as intended.
ATSB comment later on the risk reduction if the aircraft had been operated with another crew member.
ATSB Safety Analysis: NVIS
Studies have shown that NVG performance can lead pilots to revert to a daytime model of operation (Rash, 2010), leading them to overlook the threats and complexities of operating with NVG. The operator’s operations manual clearly reminded crew…that the use of NVG carries limitations and risk.
The search area was an area of low-contrast terrain for NVIS operations. This meant that elements of the terrain reflected similar amounts of celestial light, creating a low-quality image in the NVG. This lack of detail reduced visual cues [which] most likely led to difficulty in perceiving the aircraft’s attitude and estimation of terrain clearance (Parush et al., 2011).
Airborne particles affect the image that NVG produce. The cues that would normally be relied upon for loss of visual meteorological conditions (VMC) may not be present. Operating unaided, light sources begin to disappear as obscurants increase. Under NVG, as obscurants reduce the light energy reaching the goggles, NVG will continue to amplify the light signal, disguising the worsening visibility (see CAAP 174-01 11).
An early decision to use a recovery drill if visual references are lost is also vital to ensure entry into IMC does not develop into a loss of control or controlled flight into terrain.
Conditions of degrading visibility create ambiguity. This ambiguity can stall decision-making, as two contextually different situations are faced (Orasanu and others, 2001).
Pilots tend to underestimate the likelihood of loss of control and overestimate their ability to continue to control the aircraft if visual references are lost (Wiggins and others, 2012).
Humans also often incorrectly believe that changes will be easy to detect in their environment. Unless someone observes a change while it is taking place, there is a good chance it will not be picked up (Wickens & McCarley, 2008). While searching outside for cues, changes on instruments can be missed.
ATSB Safety Analysis: Single Pilot Operation
Monitoring is a fundamental tool to boost threat and error management (Flight Safety Foundation, 2014). While there is a clear benefit to multi-crew operations, there is no requirement for multicrew in Australian search and rescue (SAR), and emergency medical services (EMS).
Crucially the ATSB note that:
Crew in the back of an AW139 cannot hear alarms from the cockpit. The 400 ft warning from the Radio Altimeter (RADALT) and the 150 ft warning from the aircraft are only available to front seat crew. The aircraft descended through 400 ft at 1,430 ft/min. The pilot resumed manual control at the time of the emergency climb call as the aircraft passed through 280 ft, 3.5 seconds later.
Had there been a second person in the cockpit monitoring the approach, their first indication of a loss of visual reference, if not announced by the pilot, would most likely be an unusual combination of attitude and vertical speed. The aircraft had developed an unusually high 900 ft/min rate of descent 12 seconds before passing through 400 ft. This information may take a monitoring ACO a second or two to process. Once processed, however, the ACO is in a position to call for a go-around, and to provide accurate information to the pilot regarding the aircraft state much sooner in the sequence.
While facing a high risk of encountering a degraded visual environment, the requirement to have the ACO in the rear cabin for winch operations degraded the crew’s defences against loss of control. The addition of another trained crewmember would be an ideal risk control for operations in potentially degraded visual environments.
ATSB Safety Analysis: Detection of the Overtorque
Analysis of the central maintenance computer (CMC) required an to access the CMC through a laptop. ATSB take the rather odd view that this is “often impractical” for a 24 hour operation in a “remote location” (actually the aircraft’ normal main operating base it the Northern Territory’s capital city). They also refer oddly to nuisance warnings resolved 6 months earlier.
ATSB Safety Analysis: Automatic Hover (HOV) Modes
HOV can be engaged while the helicopter has a high rate of descent.
It would display as engaged even though it could be subject to a considerable overshoot, outside of the system’s capacity to recover before impact with terrain.
At the height engaged, the mismatch between reference height and actual radar height would have triggered a PFD message ‘HTLM’ and an aural callout of ‘ALTITUDE, ALTITUDE’ after about 2.5 s, as the aircraft passed through a point between 39 ft and 70 ft below the reference height. The pilot input came 4.2 s after engagement of automatic hover.
Without the correct mental model of HOV mode operation, time taken to interpret autopilot performance may have delayed manual recovery actions.
ATSB Findings: Contributing Factors
During the search for a transmitting beacon, the helicopter crew planned to approach to a hover near a target. However, low celestial illumination and drifting smoke created a high risk of encountering a degraded visual environment. This resulted in a loss of visual references on approach.
During the approach to hover in a degraded visual environment, searching outside for visual cues drew the pilot’s attention away from the flight instruments. This resulted in flight instruments not being referenced when they were needed.
The required position of the aircrew officer in the rear of the helicopter prior to descent negated the benefit of having a trained and competent crewmember to assist the pilot, resulting in a degraded monitoring capability in the approach to hover.
While on approach in a degraded visual environment, without the protections of flight instrument use or monitoring, the helicopter entered an uncommanded, undetected high rate of descent, resulting in a transmission overtorque during recovery.
ATSB Findings: Other Factors that Increased Risk
Auto hover had no design limit on vertical speed for engagement, which permitted overshoot following engagement with high rate of descent.
As the aircrew could not confirm the existence of an exceedance, and a maintenance message was not detected on the Crew Alert System, the aircraft was operated despite requiring an inspection.
ATSB Findings: Other Findings
Application of good CRM and practiced recovery techniques supported the crew in restoring control.
The emergency position-indicating radio beacon was not registered to the current owner, and was incorrectly placed in the boat. The placement scattered the beacon’s signal, leading to loss of accuracy in direction-finding equipment. As a result, mission complexity and time taken to rescue were increased.
ATSB Follow-Up on Single Pilot Ops
ATSB has been approached by a number of reporters “with concerns regarding loss of control incidents involving AW139s operated by SAR operators, crewed with single pilots utilising night vision goggles (NVG)”.
Conducting single pilot NVG operations for out-landings is in line with other jurisdictions. However, the Australian SAR/EMS NVG single pilot role has expanded to include advanced low-level operations, searching, advanced winching, vessel winching and low visibility operations. These operations are frequently being conducted as emergency situations in poor useable cue environments (UCE) due to the tasking priority and task approval by the contracting agency. The heightened risks of single pilot NVG operations are outlined in multiple research papers, regulator guidance and past incident and accident reports.
The reporters collectively state that the Australian industry’s liberal interpretation of the mandatory second occupant, has allowed aircrew officers (ACO) to operate from the cabin during NVG winching operations. One reporter stated that when the ACO is in the rear cabin, their attention is required on other critical duties and is no longer focused on the cockpit. In the winching phase, the full attention of the ACO is required on exactly that, resulting in the pilot being left with degraded or no cockpit support at the time of highest risk, when they would benefit from it most (ATSB investigation AO-2018-039). Conversely, if the pilot has any expectation of help or crosscheck from the ACO, it may exacerbate a situation when it is not forthcoming, as highlighted in ATSB investigation AO-2016-160.
The reporters believe that Australia continues to base the SAR night winching crewing model from a time when smaller, performance limited helicopters, that could not accommodate multi-crew, were used. This is no longer the case in the era of AW139s, which is an aircraft that is designed for, and mostly operated by multi-crew. Australia’s crewing model and mission profiles are outside global norms, best practice, and beyond the intention of CASA regulations and the rotorcraft manufacturer’s certifications.
All the reporters believe that even non-complex night SAR operations utilising NVGs is at the upper end of pilot cognition, regardless of single pilot experience or training.
CASA has agreed to…
….update the NVIS multi-part AC to include detailed information on the UCE and use of white light for situational awareness. Due to competing priorities, it is expected the amendment to the AC will be complete by late September 2022.
Safety Resources
We have discussed helicopter automation previously:
SAR Consultancy: Procurement, Tenders, Contacts and In-Service Assurance and Aviation Advice
In September 2017 one European Coast Guard selected Aerossurance to be their new aviation consultants after a competitive tender with 7 bidders. In July 2018 Aerossurance started work supporting a second European Coast Guard with a procurement project. The Aerossurance team is and has supported humanitarian aid agencies, air ambulance charities, military air arms, environmental agencies and blue chip energy companies on other emergency service and special mission aviation projects around the world.
Aerossurance has extensive air safety, flight operations, SAR, HEMS, airworthiness, human factors, aviation regulation and safety analysis experience. For practical aviation advice you can trust, contact us at: enquiries@aerossurance.com