BK117 Offshore Medevac CFIT & Survivability Issues (Southern Lakes BK117C1 ZK-IMX, Southern Ocean off Auckland Islands)
On 22 April 2019 Southern Lakes Helicopters Airbus / Kawasaki BK117C1 ZK-IMX suffered a Controlled Flight into Terrain / Water (CFIT/W) while positioning for an offshore medical evacuation (medevac) flight.

The Accident
The New Zealand Transport Accident Investigation Commission (TAIC) issued their safety investigation report on 22 April 2023.
TAIC explain the helicopter, based at Te Anau, was tasked for a medevac from a fishing vessel in the Southern Ocean off Auckland Islands. The casualty “required urgent hospital treatment” (though their medical condition is not elaborated upon) and “the first aid stocks on the vessel needed replenishment”.
The operator had 8 helicopters (a mix of BK117s, AS350s, EC120s and R44s). They held a New Zealand CAA Part 135 approval. TAIC give very little other information about them, although while they…
…had substantial procedure manuals for major operations, such as flying in the Antarctic or when working with the local search and rescue organisation, the guidance procedures for this high-risk type of operation was spread across several sections of the exposition.
Ominously:
Much of the operator’s experience had yet to be documented.
In the early 2000’s Ambulance New Zealand and the NZ Helicopter Association had developed a joint standard called the ‘New Zealand Aeromedical and Air Rescue Standard’ (NZAARS). This standard reportedly did not apply because “this flight was a privately-funded medical evacuation”. There is no clarity on how the flight was tasked or by who.
TAIC comment that:
The operator had found from experience that standard aviation weather forecast information was not reliable for the Southern Ocean. They obtained their own weather information from several different but well-known sources, including the automatic weather station (AWS) on Enderby Island, then made their own assessment.
As they were aware of the cold front approaching they planned to position to Enderby Island (the ‘positioning flight’) before it arrived and stay overnight at a hut where the operator had a fuel store. The next day the helicopter would rendezvous with the fishing vessel, hoist aboard the casualty and after refuelling again at Enderby Island, return to New Zealand on 23 April 2019 in the clearer air behind the cold front.
On board for the visual flight rules (VFR) positioning flight were a single pilot, a paramedic in the front left hand seat, and a hoist operator in the cabin.
The pilot had 6673 hours in total (all VFR). They had trained on night vision goggles (NVGs) in 2013 and had 73 hours on NVG experience, but had done less than 1 hour in the last 90 days. The pilot did not hold an instrument rating and and had only flown to Auckland Islands once before.
The paramedic had a logged time 198 hours on NVGs but worked for another company and was only called in when medevacs occurred.
The pilot had completed Helicopter Underwater Escape Training (HUET) in July 2013. The paramedic’s last HUET was in May 2018 and the hoist operator, who was a casual part-time employee, had completed HUET in September 2013.
Our observation: two of the crew had therefore not done HUET in over 5½ years and two were casual staff who were only called in when their specialist skills was required.
TAIC explain that:
The positioning flight was intended to arrive during daylight, but unexpected delays to the departure time resulted in them arriving after dark.
TAIC point our that:
The risk profile changed as the day progressed, but the plan remained the same.
Our observation: always be wary that changes of circumstances may need a reconsideration of the plan. This was especially true in this case as that even with external auxiliary fuel tanks, once the crew passed the point of no return they had insufficient fuel to land anywhere but the Auckland Islands!
These delays were stated to be due to “release of the required medical supplies and delivery to the helicopter”. Furthermore, TAIC found that:
The helicopter was loaded above its maximum certified weight limit…and would have further exceeded it on the return flight.
Because of the delay:
The crew carried NVGs and donned them during the positioning flight to continue under VFR using NVGs.
The investigators give considerable context on NVG operation. They identify that the Flight Safety Foundation (FSF) Basic Aviation Risk Standard (BARS) for Contracted Aircraft Operations has a detailed appendix on NVG / Night Vision Imaging System (NVIS) operations.
TAIC describe both NVG and helicopter air ambulance operations as being within a “regulatory void” in New Zealand.
There are service available that can predict illumination levels at night to aid NVG flight planning but the pilot did not have access to this type of data. The UK Met Office provided investigators with an illumination prediction for Auckland Islands around the time of the planned arrival using Met Office Night Illumination Model (MONIM) of 0.3 millilux. TAIC contrast this with a full moon being c300 millilux.
 The illumination was at its minimum because at that time the sun has set but the moon was still below the horizon.
The illumination was at its minimum because at that time the sun has set but the moon was still below the horizon.
As the helicopter neared its destination…
The pilot discussed their view of the approach to the landing point with the paramedic. They both recalled that a large bank of cloud covered the landing point and extended to the south, but that there was a clear area over Port Ross extending out toward the northwest. If they could not follow the coastline, they had alternative landing points on the islands programmed into the GPS that they could land at and camp out for the night.
The pilot pointed out the area clear of cloud and advised the paramedic that they would continue to head south past Ewing Island, descend in the clear area, and fly back along the beach to the planned landing point on Enderby Island. They turned south at 1934, passing 1.5 nm to the east of the landing point.
 Investigators however believer that the cloud was very likely to have been sea fog. Furthermore, they also note that:
Investigators however believer that the cloud was very likely to have been sea fog. Furthermore, they also note that:
One of the known risks while using NVGs is the potential loss of contrast that a flat calm sea creates. It makes height judgement more difficult…
Crucially:
With more currency on NVGs, the pilot may have questioned their impression of a dark area beyond the cloud. With a different expectation from Crew Resource Management (CRM), the [paramedic] may have been more effective in challenging the pilot’s perception.
Also:
It was getting near to the maximum duty time for the pilot. The exposition allowed for up to 8.5 hours flying in any 11-hour period, but had no weighting for NVG time.
TAIC note that one source of guidance material suggests weighting NVG flight time 2.3:1.
While the pilot set and reset the radalt bug height while descending it gave only a visual indication (there was no aural alert). It was only visible from the paramedic’s seat if they leaned towards it, and then only with a parallax error. TAIC notes that regulatory requirements on radalts in NZ are ‘very general’ but that the FSF BARS Standard for Offshore Helicopter Operations (BARSOHO) specified “at least one” radalt, with dual analogue displays and aural alerts as well as having defined procedures for their use. BARSOHO would also require Terrain Avoidance and Warning System (TAWS) with the new enhanced offshore modes as soon as they become available.
Without being asked to, the paramedic read out the altitude, but from the barometric altimeter that was readily visible from their seat (unlike the radalt). This would have read 500 ft higher than the radalt due to the pressure setting selected.
The [operator’s] exposition stated that the maximum descent rate on NVGs was 300 ft/min and for pilots to use the radio altimeter both on descent and while in the area, setting the decision height alarm accordingly. The GPS record showed that the pilot descended initially at about 500 ft/min down to 1000 feet above the surface, then at over 1300 ft/min until just before impact.
The investigators describe this as the “next step change in risk”. TAIC explain that:
The pilot…was turning back towards the landing area when the crew member (paramedic in front left-hand seat) alerted them to cliffs rising immediately ahead.

The pilot reacted, but the helicopter impacted the sea [at 19:37]. The helicopter…flipped upside down, but initially remained partially submerged at the surface.
Damage to the wreckage was consistent with the helicopter impacting the water at speed, with the power on, and in a shallow angle of descent with a slight right-hand bank.

The helicopter would have tipped forward until the main rotor blades contacted the water. This action would have rotated the helicopter fuselage up and around and then hard down onto the left-hand side. The transmission and rotor head and the two left-hand doors would likely have departed during this stage of the impact. The cockpit floor had been forced upwards slightly and pivoted around a point in the floor where the front cross-brace for the skid penetrates, back towards the rear of the front door frame…

It was dark, but there was enough light for the crew to see each other and make out their surroundings. The crew recalled that the sea state was dead calm.
While the sea state may have made visually identifying the surface more of a challenge, it was a likely factor in the post-impact survival of the three occupants.
The occupants were all wearing helmets, survival suits and life jackets.
The crew were able to escape while the helicopter was partly submerged, but it sank soon after.
One steel attachment of the hoist operator’s harness broke in overload (similar to that which occurred in 2022 in this AS332L1 Super Puma accident: Sheriff Super Puma Brownout Accident: NTSB Report).

The hoist operator in the rear cabin, despite wearing a helmet,…
…was knocked unconscious during the impact, but was able to be evacuated by another crew member.
It is not clear if the injury was because of movement after the seat harness failure. It appears they were rescued through the cabin doorway (the left hand cabin door having been released on impact). Fortuitously they regained consciousness when in the sea, free of the aircraft.
Water temperature was c 10°C.
None of the crew had an emergency beacon or survival equipment on their person or in their immersion suit pockets. They had packed all their personal locator beacons (PLBs) and other survival gear into an emergency grab-bag that was stowed in the rear cabin and this was lost with the helicopter when it sank.
The yellow FAA TSO-C70a, Type II liferaft carried in the cabin proved difficult to identify in the darkness and was not deployed. Type II rafts are not intended for commercial air transport operations (a further shortcoming).
No aircraft Emergency Locator Transmitter (ELT) signal was received because the fixed unit was submerged on impact and no Automatically Deployable ELT (ADELT) was carried. The operator’s Chief Pilot had however been monitoring satellite flight tracking signals.
After attempting to contact the helicopter crew on the satellite phone, and confirming with the TracPlus call centre that it was not a system fault, the chief pilot notified the Rescue Coordination Centre New Zealand (RCCNZ) at 20:08 [31 minutes after impact].
Three rescue helicopters departed New Zealand at about 1015 on 23 April 2019 [14+ hours after the accident]. The first arrived on scene at 1142 and saw the three crew members in their brightly coloured immersion suits walking on a beach near Crozier Point at 1145 [15.5+ hours after the accident].
Meanwhile:
After sheltering under cover overnight, [the helicopter crew] were spotted the next day by one of the rescue helicopters and brought back to Invercargill to be checked in the hospital.
The crew suffered only minor injuries and the helicopter, was recovered about three weeks later from a depth of 15 m.
TAIC’s Key Lessons
- The minimum requirements for NVG currency do not equate to proficiency. A pilot needs to also feel comfortable flying with NVGs and confident about their own knowledge and skill with NVIS operations.
- The benefit of underwater escape techniques training and immersion suits [i.e. survival suits] to helicopter crew flying over water cannot be emphasised enough. They are lifesaving.
- If you need to wear an immersion suit because of the risk presented by your operating environment, also carry a PLB and other selected survival items on your person to support your survival chances and expedite a rescue.
- When operating helicopters using NVGs, radio altimeters become an essential instrument. Their effective use at low level and crew awareness of what actions to take with height alerts should be a standard flight crew and NVIS crew member recurrency training exercise.
- Pilots should log their NVG flight time in a separate column of their logbook.
- Overloading the internal load capacity of a helicopter is a safety hazard.
- To be effective, emergency equipment (such as a life-raft) must not only be accessible, but must be locatable in an emergency and deployable for the crew to use. [Our Observation: that’s why BARSOHO for example specifies external liferafts that can be deployed from the cockpit or from immediately outside the cabin].
TAIC Omissions
Despite stating that NVG/NVIS and helicopter air ambulance operations are both within a “regulatory void” in New Zealand, TAIC fails to also identify that offshore helicopter operations are in the same void.
To better understand the survivability measures after an offshore helicopter accident we recommend the Flight Safety Foundation (FSF) Basic Aviation Risk Standard for Offshore Helicopter Operations (BARSOHO), launched in May 2015. It is loosely based on the concept of their award winning Basic Aviation Risk Standard, used in the mining industry, but written specifically offshore operations. BARSOHO is fully aligned with the HeliOffshore Safety Performance Model (SPM) and includes appendices for SAR, transport hoisting and medevac.
The standard is orientated around a risk bow-tie, contains a number of common and specific threat controls as well as recovery measures (grouped in distinct categories, for survival after an offshore accident) and underpinning enablers:
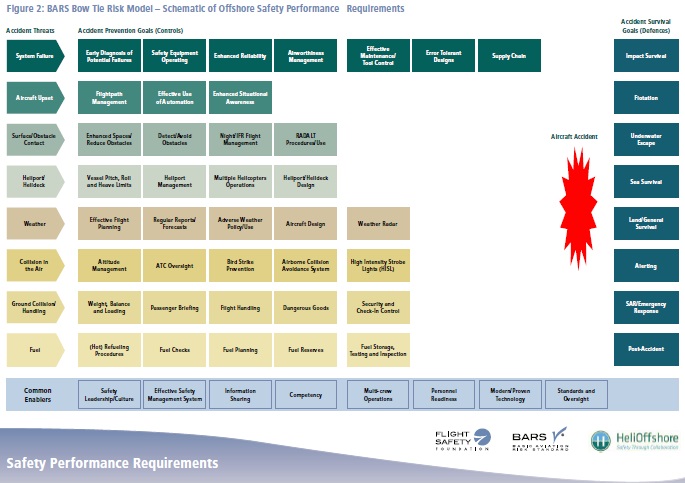
The right hand side is based on UK CAA / industry developed methodology in CAP641 Review of Helicopter Offshore Safety & Survival (the RHOSS Report). Some of the other issues that become evident with this operation when comparing with BARSOHO:
- Impact Survival: The BK117C1 certification basis predates improvements in crashworthy seating requirements. Hence the cabin seats were designed to survive only 4 G (front, back, left and right),
1.5 G (upward) and 8 G (downward) impacts. - Flotation: No Emergency Flotation System (EFS). While the helicopter suffered a water impact rather than a ditching, EFS coupled with Automatic Float Deployment Systems (AFDS) has proved very effective in similar case in the past (e.g. Bond Offshore G-REDU in 2009 on approach to the BP ETAP installation in the Central North Sea). Coincidentally you may have noticed the BP logo on ZS-IMX; its presence is not explained. NZAARS surprisingly only requires EFS for single engine helicopters operating more than 10 nm from shore.
- Underwater Escape: As noted above two of the crew had not done HUET in over 5½ years. Four years is normally accepted as the maximum per period between HUET training and the longer gap risked skill fade. They occupants do not appear to have been equipped with a Compressed Air Emergency Breathing System (CA-EBS). The layout of the cabin and access to emergency exits in particular is not elaborated upon by TAIC nor it clear if a Helicopter Emergency Exit Lighting System (HEELS) was fitted. The row of three side facing troops seats (see below) does appear to leave only the cabin doorway / cabin door windows available for egress. It was fortuitous in this case that one cabin door detached (rather than jammed) upon impact.
- Sea Survival: The lack of external liferafts and the remoteness of the accident site meant the occupants had to swim to shore to survive as in 10°C water they would have not been expected to survive for 15.5+ hours until rescuers arrived. Once the only occupant in the cabin was knocked unconscious, the probability that the sole internal raft could be deployed reduced significantly.
- Alerting: No ADELT. ADELTs have been common in Europe and on large offshore helicopters since the 1990s, their performance has been patchy as described by UK CAA in CAP1144, but when they work they provide a floating (jettisoned) ELT to transmit a signal to alert rescuers, independent of any survivors, even after the helicopter sinks. An ADELT signal would most likely have reduce the 31 minute period of uncertainty after the satellite tracking data ceased.

Safety Resource
The European Safety Promotion Network Rotorcraft (ESPN-R) has a helicopter safety discussion group on LinkedIn. You may also find these Aerossurance articles of interest:
- Blinded by Light, Spanish Customs AS365 Crashed During Night-time Hot Pursuit
- Offshore Night Near Miss: Marine Pilot Transfer Unintended Descent
- A HEMS Helicopter Had a Lucky Escape During a NVIS Approach to its Home Base
- Air Ambulance Helicopter Struck Ground During Go-Around after NVIS Inadvertent IMC Entry
- Automation Issues During Night SAR Training – Near CFIT
- North Sea Helicopter Struck Sea After Loss of Control on Approach During Night Shuttling (S-76A G-BHYB 1983)
- NTSB Investigation into AW139 Bahamas Night Take Off Accident
- Night Offshore Training AS365N3 Accident in India 2015
- Loss of Control, Twice, by Offshore Helicopter off Nova Scotia
- SAR Helicopter Loss of Control at Night: ATSB Report
- US Fatal Night HEMS Accident: Self-Induced Pressure & Inadequate Oversight
- HEMS A109S Night Loss of Control Inflight
- Air Ambulance A109S Spatial Disorientation in Night IMC
- HEMS S-76C+ Night Approach LOC-I Incident
- Night Offshore Windfarm HEMS Winch Training CFIT (BK117C1 D-HDRJ)
- TCM’s Fall from SAR AW139 Doorway While Commencing Night Hoist Training
- Swedish SAR AW139 Damaged in Aborted Take-off Training Exercise
- Fatal Taiwanese Night SAR Hoist Mission (NASC AS365N3 NA-106)
- SAR Crew With High Workload Land Wheels Up on Beach
- Beware Last Minute Changes in Plan
- NH90 Caribbean Loss of Control – Inflight, Water Impact and Survivability Issues
- SAR AW101 Roll-Over: Entry Into Service Involved “Persistently Elevated and Confusing Operational Risk”
- Night Mountain Rescue Hoist Training Fatal CFIT
- Heliski Flat Light Flight into Terrain
- Canadian Flat Light CFIT
- That Others May Live – Inadvertent IMC & The Value of Flight Data Monitoring
- UPDATE 16 July 2023: SAR AW139 LOC-I During Positioning Flight
- UPDATE 17 February 2024: Night Offshore Take-Off Loss of Control Incident
- UPDATE 18 February 2024: Night Offshore Helicopter Approach Water Impact
- UPDATE 13 July 2024: Fatal USCG SAR Training Flight: Inadvertent IMC
- UPDATE 20 July 2024: Night CHC HEMS BK117 Loss of Control
- UPDATE 8 February 2025: S-76D Loss of Control on Approach to an Indian Drilling Rig
The Tender Trap: SAR and Medevac Contract Design Aerossurance’s Andy Evans discusses how to set up clear and robust contracts for effective contracted HEMS operations.