SMA SAR Leonardo Helicopters AW139 SE-JRM With Damaged Landing Gear After Training Accident (Credit: SHK)
Background to Training
The Swedish Accident Investigation Authority (SHK) explain in their safety investigation report (issued 7 October 2020) that the flight was a training flight for a new SMA SAR pilot focused on confined area take-off and landings.
The student pilot was experienced, both as a helicopter pilot and on the helicopter type [c 4000 hours on the AW139]. However, the student pilot had not practised the take-off profile in question previously, except in a simulator in the week prior to the occurrence. Nevertheless, the simulator that was used did not have a full visual field downwards through the lower windows (‘chin windows’), which is necessary if it is to be possible for the exercise to be performed in accordance with the type certificate holder’s rotorcraft flight manual (RFM).
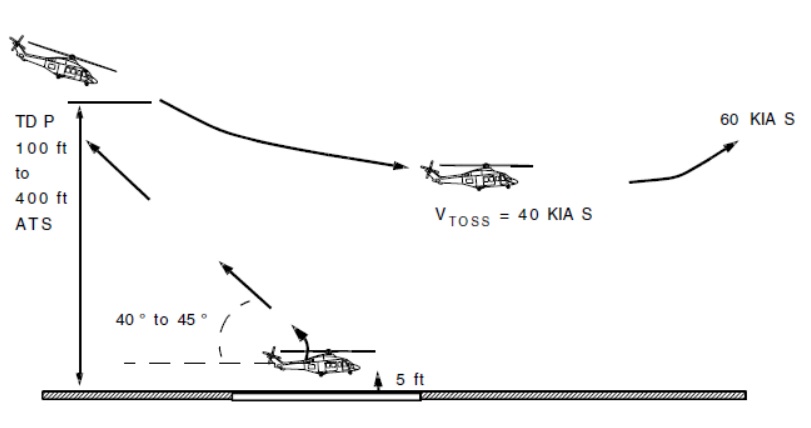
The flight profile…involves the helicopter climbing vertically…and then commencing a climbing reverse manoeuvre that continues until the helicopter has reached a ‘decision altitude’. This means that, from there, the pilot is able to dive to increase speed and fly over obstacles ahead in the event of the failure of one engine.
Intended Take-Off Profile (Source: Leonardo AW139 RFM via SHK)
Should an engine failure occur before the take-off decision point has been reached, the intention is for it to be possible to land the helicopter at the original take-off site. It is important that the pilot maintain visual contact with the take-off site until such time as the TDP has been passed…
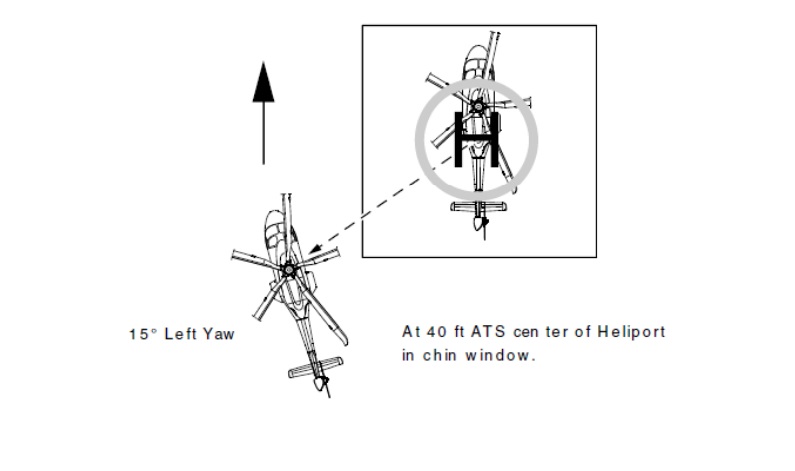
So that it is possible to…maintain continuous contact with the take-off site through the chin window, the pilot flying the helicopter has to yaw it [by 10-15 degrees] once they reach 40 feet.
Take-Off Profile Yaw above 40 ft when Pilot Flying is in the Right Hand Seat (Source: Leonardo AW139 RFM via SHK)
[The RFM] contains images of the pilot’s visual impression through the chin window at various altitudes.
Example Take-Off Profile Image at 150 ft when the Pilot Flying is in the Left Hand Seat (Source: Leonardo AW139 RFM via SHK)
It is also [specifies] how much engine output is to be increased from hover prior to take-off and then from the state at which the helicopter transitions from climbing vertically to climbing backwards up to the TDP.
The Training Exercise
The SHK comment that:
The exercise had been run through carefully during the simulator training and an alternative to the initial yaw had been discussed. The student pilots had been given the opportunity to move sideways instead [as] the yaw itself may overload the student pilot and because there were certain limitations with regard to downward vision in the simulator, which were accentuated when yawing the helicopter.
The exercise is normally not particularly dramatic and does not require the rapid monitoring and manoeuvring that are characteristic of, for example, emergency landing and autorotation exercises. Nor is the exercise deemed to lead to an increased risk that requires the emergency services to adopt a higher state of readiness.
No specific abort criteria were discussed during the exercise.
The training was being conducted using the Visby base’s on stand-by AW139.
In order to maintain readiness during the training flight, the helicopter was equipped with material and fuel for a potential mission. In addition, it was necessary for the exercise to take place close to the standby crew so that the helicopter could be handed over quickly in the event of a potential mission.
The aircraft mass was 5809 kg. This training exercise is recommended to be conducted at 5650 kg or below in the RFM.
The instructor was sitting in the right front seat and the student pilot was sitting on the left, both were using the installed safety belts. The accompanying student pilot was sitting on a bench by the front wall of the cabin, without a safety belt.
SHK describe how…
The training began with the student having to handle practiced engine failure from hovering at heights 5, 10, 20 and 30 feet…
Wind speed was low, 5 knots gusting 8 knots. The instructor then demonstrated a take-off and landing of the flight profile with a simulated engine failure before TDP, then…
…the student pilot began performing an equivalent take-off and landing profile involving a simulated failure of one engine. The exercise was performed perpendicular to the runway direction because the wind was westerly and and the exercise requires headwind or very limited crosswind component.
During the exercise, there was a tendency for the helicopter to land a little too far forward. Consequently, the instructor decided to perform an additional exercise.
During the introductory demonstration by the instructor take-off began with a 13-degree yaw. FDR data from the demonstration also shows that the take-off profile was performed by the book, with the engine output and attitude being adapted during the climb.
During the student pilot’s first exercise, the yaw was slightly lower and began at a later stage than specified in the manual.
There was no yaw during the student pilot’s second attempt. The initial reverse became problematic [and] the student pilot was not able to maintain a constant visual reference of the landing site in the chin window in accordance with the description in the RFM.
During the continued reversing climb towards the TDP, the instructor made the assessment that the angle had become too sharp to allow the helicopter to return to the take-off point in the event of an aborted take-off. As a result, the instructor extended the procedure slightly in order to give the student pilot the opportunity to correct the angle and return to the intended flight profile. This resulted in the helicopter continuing past the maximum recommended altitude of 400 feet up to 430 feet.
The climb took 42 seconds.
When they reached the decision altitude, the rate of climb had decreased slightly and when the decision was made to simulate one engine in-operative, the helicopter was not climbing but descending a little while continuing to reverse.
When the instructor activated the training mode for simulating flight with one engine inoperative, the indicator for engine output showed a simulated loss of power in one engine. The student pilot reported `torque split’ and pushed the collective [sic] forward so that the nose was dropped markedly with the aim of transitioning from reverse motion to forward motion.
However:
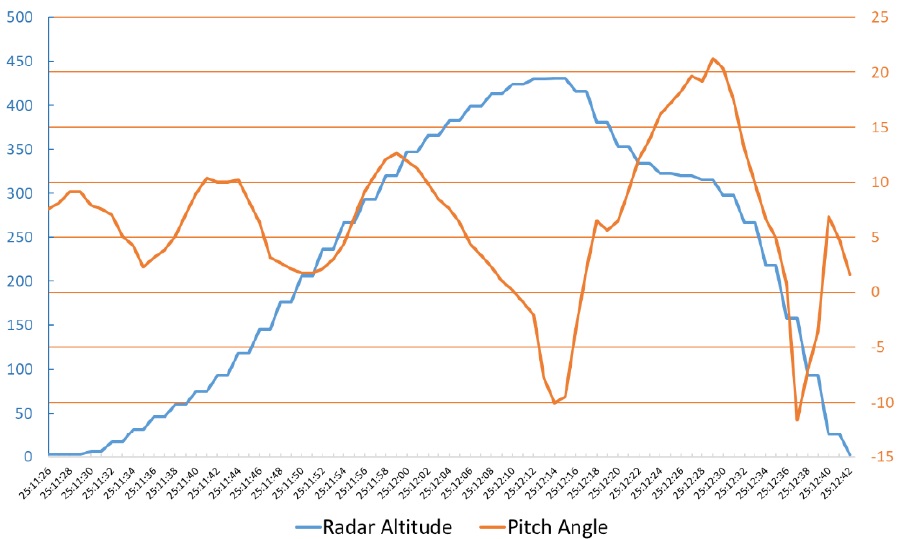
The rate of descent increased and soon after the pilot raised the nose markedly, up to 20 degrees nose up, in order to reduce the effect of the preceding manoeuvre. At this stage, the student pilot again lost sight of the landing site. Immediately after this, the crew felt a large and unexpected descent.
[T]he instructor had his left hand on the collective. There is a button on the collective called the ‘torque limiter’, which reinstates the power output from the engine when pressed. The instructor has stated that the way he was gripping the collective did not allow him to activate this function and that he made an immediate instinctive decision to focus on manoeuvring the helicopter using the limited engine output that was available. He did not want to move his gaze to the collective to look for the button, which under the prevailing circumstances could result in a loss of valuable seconds.
Leonardo Helicopters AW139 Collectives with Torque Limiter (TQ LIM) Button Circled: Note Different Tactile Design to Aid Identification by Touch (Credit: SHK)
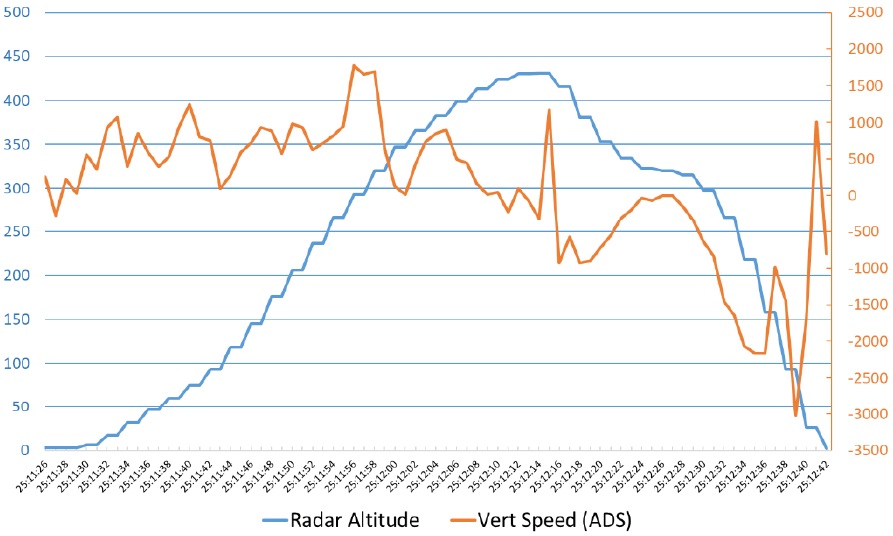
The rotor speed of 102 % was maintained down to 270 feet and the vertical speed (V/S), ‘the descent’, increased to 1,650 feet/min. For a short time the vertical speed increased to over 2,000 feet/min. A nose-down movement was initiated, which resulted in vertical speed of over 3,000 feet/min., at the same time as some forward motion was being obtained. The collective was raised and the rotor speed fell to 87.1 %, which causes the OEI training mode to deactivate automatically, at that same time, the FDR data recorded that the rotor speed was low (`Rotor Low’).
SMA SAR Leonardo Helicopters AW139 SE-JRM Flight Profile from FDR Data: Note Training Conducted Into Wind (Credit: Leonardo via SHK)
The altitude was approximately 70 feet when the nose was raised, at the same time as the collective continued being raised in order to increase power. The vertical speed decreased in the final seconds to approximately 1,200 feet/min. before the helicopter made contact with the ground and bounced before the forward motion generated was checked.
FDR data indicates contact on the left main wheel at 6.1 m/s vertical speed (20 ft/s) and a vertical acceleration of 3.38 g. The landing gear had been tested at maximum gross weight at 2.8 m/s (9.2 ft/s). As SHK point out a “13.9 % reduction in mass cannot itself compensate for the 218 % increase in vertical speed” especially as kinetic energy is dependent on the square of velocity.
The crew perceived the contact with the ground as a hard touch-down, but not so hard that it was felt to be damaging. The intention was to take-off once again when the student pilot in the cabin noticed that the helicopter’s [left hand exteral] liferaft had been released… The crew then shut down the engines and informed the tower of what had happened.
The three occupants were uninjured. The HR Smith503-16 emergency locator transmitter (ELT) did not activate.
Structural damage occurred to the left landing gear and its attachments to the fuselage. Damage also occurred to panels and beams around the fuel compartment in the cabin.
Damage to SMA SAR Leonardo Helicopters AW139 SE-JRM After Training Accident (Credit: SHK)
[A] leak from the helicopter’s landing gear hydraulics that was later detected was cleaned up by the airport’s fire and rescue service…
SHK note that analysis of the CVR revealed that while communication was normal early in the exercise, during the critical phase the dialogue ceased.
Organisational Factors
The SHK comment on the relatively high turnover on nominated managers within the SMA helicopter operation. They also comment that there had been a big reduction in the pool of instructors after a change in terms and conditions in 2018.
It has emerged during interviews that the limited availability of instructors has resulted in difficulties for training operations.
One person has kept training operations running almost single-handedly. At the same time, there has been limited insight into the details of training components for those not directly involved in day-to-day training. The training components have not been evaluated or risk assessed. Nor has any audit or similar been conducted in order to see how closely the training components adhere to the descriptions that have been drawn up or the specified curriculum.
Nevertheless…feedback suggests that the training programme had prepared the prospective pilots for their future duties in a good way.
The Maritime Administration has made various attempts to plan to get new qualified instructors approved by the Swedish Transport Agency. It has repeatedly been difficult to get this planning to correspond to the testing sessions arranged by the Transport Agency. According to the Maritime Administration, there have been too few of these sessions, and they have been too infrequent.
SHK Safety Analysis
During the student pilot’s second attempt, there was no yaw and the student pilot has stated that they lost the visual references during the initial reversing climb. This resulted in impairment to their spatial orientation, which in turn had an impact on their chances of finding an acceptable reversing profile. This resulted in the reversing climb being too steep.
Prior to the session in question, the instructor and the student pilot had not discussed or established conditions for when the exercise could be aborted. Nevertheless, there was always a basic pattern for aborting an exercise. When the instructor says ‘my controls’, the student pilot has to hand over control to the instructor or commander. No such takeover of control took place during the session in question.
The student pilot was very experienced on the helicopter type and felt confident in the cockpit. He was well acquainted with the handling of the instruments and controls. The instructor also had great confidence in the student pilot’s ability to complete the training component. In advance, there was nothing to suggest that the student pilot would have any specific difficulties completing the component in question.
Both…stated that the reversing climb was perceived as acceptable and… they did not believe there was any need to abort the exercise. However…the helicopter was outside of the exercise profile in question throughout pretty much the entirety of the reversing climb. During this part of the flight, the instructor also gave the student pilot several instructions with the aim of trying to correct the profile and speed.
When the instructor activated training mode in order to simulate one engine inoperative they had already passed 400 feet, the recommended upper limit for performing the exercise, the helicopter was descending slightly while still reversing and the student pilot had already lost visual references to the take-off site. Continuation of the exercise…
…may be explained by the confidence the instructor had in the student pilot…[as they]…had completed the previous exercises in an excellent and rapid manner.
When “training mode” was activated and the nose was immediately dropped markedly in order to transition to forward motion, at a stage where there was no longer upward movement, the height gain (`ballooning effect’) in which the kinetic energy upwards is utilised during the transition, and on which the procedure is based, was absent. Instead, the descent and the speed increased in an undesirable way.
In order to correct this, the nose was raised markedly, which resulted in a nose-up attitude of approximately 20 degrees. With the nose as high as this, with close to the maximum mass for the exercise and one engine in training mode, the result was a sudden and rapidly accelerating descent.
The silence in the communication between the instructor and the student pilot that occurred and the failure to inactivate training mode indicates that the crew was not prepared for the manoeuvre to have this outcome. Both the student pilot and the instructor have stated that it was only at this time that they felt the exercise went outside of what was expected, but neither the student pilot nor the instructor felt the nose-up attitude was as radical as it actually was.
The instructor had his left hand on the collective, but was not prepared to quickly inactivate training mode by, for example, pressing the torque limiter button. Activating the torque limiter or inactivating the training mode switch at an early stage would probably have resulted in a safe end to the exercise.
At a late stage, when the pilots increased the collective pitch in order to reduce the rate of descent close to the ground, and the rotor speed fell to 87 %, training mode was inactivated through the inbuilt safety function. The rate of descent decreaesd but the altitude was too low to avoid a hard landing. The fact that the rate of descent decreased with the increased power output and lift confirms that this was not a vortex ring state…
…there were several occasions when it would have been reasonable to abort the exercise… However, it is easy to draw this conclusion in retrospect, especially given the outcome. It is…SHK’s opinion that ahead of every exercise component, there is a need to run through which abort criteria that should apply and how various situations are to be managed.
The SHK then go on to opine on the value of phased training, slowly building up the exercise scenario.
[T]he Swedish Maritime Administration should review how the procedures are described in the training documents and identify if and in such a case what deviations occur in relation to the type certificate holder’s flight manual, RFM. Such a review should include the current education and focus on whether concrete interruption criteria need to be formulated, both from a learning and a safety perspective.
They also comment on the importance of measures taken to ensure adequate resourcing for the organisation and the challenges of ensuring the aircraft is available at an adequate mass for exercises.
SHK Determination of Causes and Contributory Factors
The cause of the accident was that the exercise was performed too far outside the exercise profile without the risks of this being identified.
A contributing factor was that there were no clear criteria indicating when and how the exercise was to be aborted.
An underlying cause at the systemic level was that the ancillary aviation safety organisation, including the safety and monitoring functions, did not have sufficient insight into how various elements were to be practised and had not conducted any assessment of risks in conjunction with the performance of the exercise as a result of a lack of staff and staff turnover, including the nominated persons.
SMA Safety Actions
This exercise is not longer carried out in the helicopter and is only conducted in the simulator.
A review and reworking of operational manuals OM-A, OM-B and OM-D was expected to be completed in September 2020.
A new Nominated Person Crew Training (NPCT) was recruited and appointed sin April 2020.
More Instructors were recruited and appointed in May 2020. There are currently 4 Pilot instructors and 2 each for Hoist Operators and Rescue Swimmers.
The Accountable Manager and Aviation Manager have quarterly reviews of the flight safety situation with SMA Senior Managers.
As a result of these actions the SHK noted they would refrain from raising any further safety recommendations.
Other Safety Resources
In 2004 the UK Air Accidents Investigation Branch (AAIB) reported on an occurrence to SikorskyS-76C G-JCBJ of JCB during a similar exercise. This was the third accident in the UK involving damage to an S-76 during practice of rejected vertical or short field take-off profiles. All three occurred during very light wind conditions. In August 2004, the UK CAA issued a communication that recommended that operators of the S-76 “conducting vertical and short field rejected take-off manoeuvres carry out an analysis of the risks associated with these manoeuvres with a view to mitigating the risks as much as possible”.
You may also be interested in these Aerossurance articles:
Aerossurance has extensive air safety, flight operations, SAR, airworthiness, human factors, aviation regulation and safety analysis experience. For practical aviation advice you can trust, contact us at: enquiries@aerossurance.com