HEMS S-76C Night Approach Loss of Control – In-flight (LOC-I) Incident
A Helicopter Emergency Medical Service (HEMS) SikorskyS-76C+C-GHHJ operated by Helijet on behalf of the BC Ambulance Service was on a VFR approach to the coastal Tofino/Long Beach Airport (CYAZ), British Columbia, Canada at 02:39 Local Time on the dark, moonless night of 15 November 2015. It suffered a Loss of Control and cleared the ground by just 3ft.
Flight Path of Helijet HEMS Sikorsky S-76C+ C-GHHJ Night Approach into Tofino, BC (Credit: TSB Final Report Issued 20 Dec 2017)
…after flying an autopilot coupled approach (RNAV29) to an altitude of 600 feet MSL in the vicinity of the threshold to Runway 29, the crew uncoupled the autopilot and continued to maneuver visually for the planned landing area. While on final approach, a high rate of descent (1100 [feet per minute] fpm) and low airspeed developed, accompanied by a violent left and right movement. The crew applied collective and forward cyclic input and the aircraft recovered at low level and airspeed. Subsequent engine and airframe indications appeared to be normal and the crew completed a second approach for an uneventful landing. A post landing inspection revealed the presence of oil on the rotor blades and airframe. A maintenance inspection confirmed that the rotor hub spindles and a damper were damaged.
A press report in December suggested the main rotor speed (NR) dropped so low that the AC generator dropped off line. They also state the patient the helicopter was due to collect, a stroke victim, was collected by a fixed wing air ambulance later in daylight. Bill Yearwood of the Transportation Safety Board of Canada (TSB) said in a TV interview:
Below 600 feet there were some excursions in heading and evidence of a high rate of descent, as much as 2,500 feet a minute for a very short time. After examination of the Flight Data Recorder we were able to determine the main rotor transmission was most likely over-torqued. That concern was raised and the company grounded the aircraft and changed all the drive train components.
This is significantly greater than the initial maintenance action reported (changing the main rotor spindles). Its not clear from the interview if the aircraft had continued flying before the FDR was analysed. However an occurrence update dated 21 December 2015 on a subsequent, 25 November 2015, occurrence involving C-GHHJ states the helicopter was:
…preparing to depart Vancouver, BC (CYVR) on a MEDEVAC flight to Chemanius, BC. Upon raising the collective to lift off from the helipad, the flight crew detected a high frequency vibration in the flight controls and an abnormal noise. When the collective was lowered the vibration and noise ceased. Another attempt to takeoff was conducted with a similar vibration and noise observed. The aircraft was taxied back to the hangar and maintenance personnel were consulted. Drivetrain components, including the aircraft’s transmission, were replaced and helicopter was returned to service.
It would be uncomfortable or disturbing to find out that actions were taken based on our investigation or the data that’s provided for our investigation.
Helijet supports and will exercise a non-punitive environment for individuals who are intending to prevent an injury or accident or are reporting any accident, incident or hazard.
And then shortly later:
Non-compliance of adhering to safety procedures and processes will not be tolerated.
The incident remains under TSB investigation but this is likely to be an investigation with many lessons both on the conduct on night approaches and handling of occurrences.
As the helicopter approached CYAZ, the crew decided to deviate from the night visual flight rules (NVFR) route and conduct a practice instrument flight rules (IFR) approach to maintain a safe profile above terrain and obstacles during the approach to the airport, as well as to maintain proficiency on an IFR approach.
On several occasions during the flight, while discussing the approach, the crew referred to “the runway” at CYAZ, and the expectation of the pilot flying (PF) was to conduct an approach to a runway environment, rather than to the temporary night helipad.
Before the occurrence flight, the crew did not discuss the Helijet TOFLZ landing plate, nor did they discuss their individual experience with landing at CYAZ. The crew did not perform any pre-flight risk assessment concerning night flying, IFR, or visual cues. By takeoff, the crew had not established a correct shared understanding of the landing site, nor did they have a shared understanding that this would be both pilots’ first approach to CYAZ at night.
The aerodrome at CYAZ was unlit, with the exception of an illuminated windsock and a ring of Turboflares on the compass rose that defined the temporary night helipad. At no time before or during the approach did the crew discuss the absence of aerodrome lighting at CYAZ.
At the time of the occurrence, the company was not using NVGs [night vision goggles], nor was it required to do so.
While conducting a visual approach to Runway 29, the crew disengaged the autopilot at an altitude of 600 feet above sea level and manoeuvred toward the planned landing area. Approximately 10 seconds after the autopilot was decoupled, the helicopter speed decreased below 60 knots indicated airspeed (approximately VMINI), and the pitch attitude increased to beyond 14° nose-up.
Once the PF recognized how close they were to the intended landing zone and determined that the landing zone was not a runway environment, the PF attempted to adjust the approach by reducing collective input to minimum power and increasing the pitch attitude to slow the helicopter further. The helicopter descended at rates exceeding 2600 feet per minute (fpm), with airspeed transitioning through 0 knots forward and entering rearward values. Control was re-established over a beach, after the helicopter had descended to approximately 3 feet above ground level, and approximately 67 feet below the airfield elevation at Tofino/Long Beach Airport.
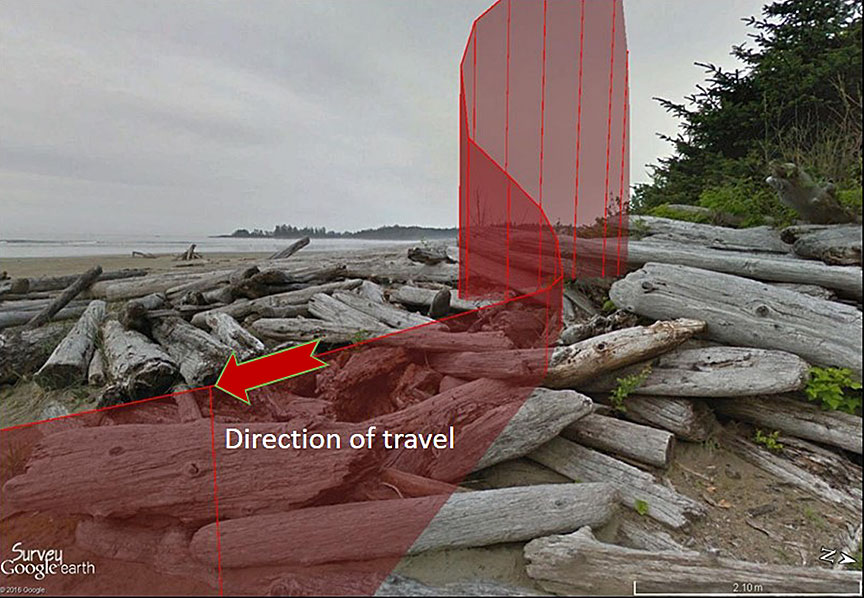
Terrain in the area where the enhanced ground proximity warning system gave the ‘TAIL TOO LOW’ alert. The approximate flight path is shown in red. The helicopter travelled from the top right to the bottom left. (Credit: Google Earth, with TSB annotations)
During the recovery attempt, the helicopter experienced a severe reduction in main rotor rotations per minute (rpm) (NR) and a loss of directional control. The pilots then observed normal engine and drivetrain parameters and climbed to 500 feet above sea level to conduct a second approach. During this approach, additional control difficulties were encountered, but the helicopter was able to land.
EGPWS
The helicopter was equipped with a HoneywellMark XXII EGPWS, which meets the Canadian Technical Standard Order C151b Class A requirements for terrain awareness and warning systems. During the occurrence sequence, modes 1 (excessive rate of descent) and 6 (altitude call-outs, excessive bank angle, tail strike) were triggered. However:
There are no emergency procedures or guidance specified in Helijet’s standard operating procedures (SOPs) or operations manual for flight crew to deal with EGPWS alerts or warnings.
Post Flight Actions (Maintenance and FDR Analysis)
In this occurrence, the helicopter experienced significant single-engine and combined torque exceedances, but this information was recorded only on the cockpit voice and flight data recorder (CVFDR), which is optional equipment.
By design, the integrated instrument display system (IIDS) did not display any exceedances or warnings after the occurrence. After landing at CYAZ, the crew checked the IIDS maintenance page for exceedances, but none were displayed, in keeping with the design of the system.
With the exceedance information unavailable in the field, the helicopter was returned to service and critical maintenance action had not been performed. There is no standard system in the Sikorsky S-76C+ to capture transmission torque exceedances with both engines operating. As a result, the helicopter was returned to service in a non-airworthy condition.
The post-flight inspection revealed a significant quantity of oil on the helicopter’s main rotor blades and on the left side of the fuselage. On further inspection, it was determined that each of the main rotor spindles had come into contact with the elastomeric blade retention bearings on the main rotor hub and that a main rotor damper oil line had been broken. Maintenance personnel changed the main rotor spindles as well as the damaged damper oil line. The cockpit voice and flight data recorder (CVFDR) was disabled to prevent overwriting of the data from the occurrence flight.
A different crew carried out a test flight, and the helicopter was flown back to Vancouver. The CVFDR was downloaded and analysed on 16 November 2015, the day after the incident.
The information showed that both engines experienced torque values in excess of 155% per engine, for a combined total of over 310%, during the recovery from the helicopter’s initial loss of control on the first approach. Furthermore, during the occurrence, the torque value on the number 1 engine had exceeded 135% for 15 seconds, and the torque value on the number 2 engine had exceeded 135% for 13 seconds. These values indicated that the manufacturer’ maximum allowable combined dual-engine transient limit of 230% torque for 10 seconds had been exceeded.
On 25 November 2015, Helijet notified the TSB of another occurrence involving C-GHHJ involving a high-frequency vibration in the flight controls and an abnormal noise (discussed above). The TSB, contacted Sikorsky with details of both occurrences:
The manufacturer had not been informed of the torque exceedances and low in-flight rpm values that the helicopter had been subject to in the 15 November occurrence. The manufacturer subsequently deemed the helicopter not airworthy and required the helicopter to be removed from service until all dynamic components had undergone inspection and overhaul maintenance procedures.
Upon further inspection of the dynamic components for possible damage, the maintenance organization concluded that there were “no major findings due to the overtoque [sic] incident.”
The manufacturer also required each main rotor blade to be inspected and tested for bonding separation, with specific direction to ultrasonically inspect each blade at the root end where the laminates were bonded to the spar. During the course of these inspections, it was established that 1 of the 4 main rotor blades had experienced bonding separation on its lower surface.
On 26 November, the helicopter’s CVFDR was secured and sent to the TSB Engineering Laboratory for data download and analysis. The analysis revealed that incorrect conversion factors had been applied when the data was first downloaded.
The TSB laboratory analysis established that, during the occurrence flight, a maximum peak engine-torque value of 134% per engine (for a combined engine torque of 268%) had occurred. It was also determined that, during the occurrence, the NR droop from 107% lasted a total of 19 seconds, reaching a minimum of 77% NR. There is no normal or emergency in-flight procedure for a torque exceedance. The manufacturer does… require maintenance action after the flight.
Analysis
The investigation found that the night VFR flight was conducted without sufficient ambient or cultural lighting (e.g. lights on buildings and roads) to maintain adequate visual reference to the ground. In addition, the flight crew did not conduct the required briefings.
As a result, by the final approach, neither crew member had developed a correct or complete understanding of the characteristics and challenges of the landing site.
When the pilot flying realized that the location of the landing area was closer than expected, the large control inputs made to adjust the descent angle and speed resulted in a hazardous approach profile, which went unrecognized as both flight crew members were occupied with maintaining visual reference.
Further, the investigation found that company SOPs provided little guidance in a number of areas, which contributed to poor decision-making and coordination.
TSB Comment
This investigation once again highlights the risks of flying under night VFR without sufficient lighting to maintain adequate visual reference.
Transport Canada regulations do not clearly define what visual references are required at night. Many pilots believe that it is acceptable to fly at night as long as the reported weather conditions are acceptable, regardless of lighting conditions.
During the investigation into a 2013 fatal helicopter accident (A13H0001 [see also our article]), the Board made a recommendation (A16-08) to Transport Canada (TC) to clearly define the visual references required to reduce the risks associated with night VFR flight.
TC indicated that it will initiate educational activities and a regulatory amendment. However, until specific details about proposed regulatory changes are fully known, the TSB cannot evaluate if these actions will fully address this safety deficiency. As such, the TC response was assessed as Satisfactory Intent.
Safety Management
Although not required by regulation, Helijet had developed an SMS and had implemented it in 2013. At the time of the occurrence, the SMS was not yet fully developed, and it had not been assessed by TC.
In the case of Helijet, the director of safety had overall responsibility for the SMS. However, this role was combined with that of the director of flight operations. It was estimated that the director of safety / flight operations was devoting 2 hours per week to the safety role. At the time of the occurrence, other identified safety officer roles were vacant, meaning there were few additional resources that could be called upon for assistance.
Information gathered during the investigation revealed that the SMS reporting process was being used to some extent, with an estimated 70 reports being received annually. However, instances were also identified where hazards or safety concerns were not reported through the reporting process. For example, approximately 1 month before the occurrence, a Helijet air ambulance pilot had recognized that CYAZ was a difficult place at which to land at night due to its lack of cultural lighting. This hazard was discussed with the airfield manager, and more Turboflares were added in a line along the taxiway extending from the compass rose. This provided additional visual cues to facilitate the departure of the helicopter and the arrival of the helicopter that was scheduled to come in later that evening. The identification of this hazard was not discussed with Helijet management or entered in the SMS reporting system.
Prior to the CYAZ occurrence, 4 temporary night helipad locations at airports were being used by Helijet for night medevac operations. When Helijet implemented its SMS program, no risk assessments were conducted on existing helipads, and this activity was not monitored as part of the SMS. This occurrence was the result of risks of night operations not being effectively mitigated by the crew and more broadly by the company. Safety management and oversight is on the TSB Watchlist.
TSB Findings as to Causes and Contributing Factors
The flight was conducted under night visual flight rules without sufficient ambient or cultural lighting to maintain adequate visual reference to the surface.
Required briefings were not conducted. As a result, by the final approach, neither crew member had developed a correct or complete mental model of the landing site.
When the pilot flying realized that the location of the landing zone was closer than expected, the large control inputs made to adjust the descent angle and speed resulted in a hazardous approach profile.
During the approach, both crew members were occupied with maintaining visual reference to the landing zone, and the hazardous approach profile went unrecognized.
While a visual approach was being conducted to a temporary night helipad at an unlit aerodrome at night, positive control of the helicopter was lost.
Helijet International Inc.’s standard operating procedures (SOPs) provided little guidance in a number of areas, including crew briefings, night visual flight rules requirements, and black-hole approach and landing procedures. As a result, the flight crew conducted a visual approach without the benefit of effective SOPs, which contributed to poor decision making and coordination.
The flat authority gradient in the cockpit was not identified and addressed by the crew, and the corresponding assumptions of crew skill and experience directly affected the quality of resource management and communication style.
The accepted practice of not fully briefing all approaches contributed to the ineffective crew coordination in this occurrence, reducing information exchanged between 2 senior crew members.
Because the processes described in Helijet International Inc.’s safety management system (SMS) were not being used effectively, the SMS did not help the company identify and mitigate the risks associated with its night medical evacuation operations.
At the time of the occurrence, there was a lack of resources and training dedicated to the company’s SMS, limiting its effectiveness in mitigating the risks in night operations.
TSB Findings as to Risk
Canadian Aviation Regulations section 602.115 does not define “visual reference to the surface,” which has been widely interpreted by the industry to mean “visual meteorological conditions.” As a result, night flights may be conducted with inadequate visual references, increasing the risk of controlled-flight-into-terrain and loss-of-control accidents.
If Transport Canada continues to allow night flights to be carried out under visual flight rules with inadequate visual references, there is a risk of controlled-flight-into-terrain and loss-of-control accidents.
If, during night visual flight rules operations, pilots continue flight in conditions where no cultural or ambient lighting exists and there is no alternate means of maintaining visual reference to the surface, there is an increased risk of controlled-flight-into-terrain and loss-of-control accidents.
If flight crews do not receive effective training in night visual flight rules operations and the associated illusions, they are at risk of not being adequately prepared for the challenges of flying in a night environment.
There is currently no regulatory process for multi-crew Canadian Aviation Regulations Subpart 702, 703, and 704 operators to have company SOPs reviewed by Transport Canada. As a result, there is a risk that non-optimal procedures will be adopted.
Unless all operators are required to have an SMS that is assessed by Transport Canada for effectiveness, there is an increased likelihood that the risks specific to an operator will go unidentified and unmitigated.
If identified hazards are not captured by a company’s SMS, they may go unaddressed, increasing the risk of accidents.
If feedback and corrective actions are not provided to employees who report a hazard or an incident, it is less likely that employees will report further hazards and incidents.
If flight data and voice recording equipment are disabled, critical information will not be captured if the aircraft is involved in another occurrence.
If service letters issued by aircraft manufacturers are not consulted, there is an increased risk that critical maintenance tasks will not be carried out.
If aircraft that are not airworthy are released for flight with required maintenance not completed, there is a risk that components will fail in flight, putting passengers’ and pilots’ lives at risk.
If operators do not disclose the full details of occurrences to aircraft manufacturers, there is a risk that an aircraft that is not airworthy will be returned to service.
Other TSB Findings
There are no emergency procedures or guidance specified in Helijet International Inc.’s SOPs or operations manual for flight crew to deal with enhanced ground proximity warning system alerts or warnings.
The operator was unaware that cockpit voice recordings are privileged under the Canadian Transportation Accident and Safety Board Act.
At the time of the occurrence, the company was not using night-vision goggles, nor was it required to do so.
Night medical evacuation flights were being conducted to Tofino/Long Beach Airport, which was certified for daylight operations only.
There is no standard system in the Sikorsky S-76C+ to capture transmission torque exceedances with both engines operating. As a result, the helicopter was returned to service in a non-airworthy condition.
Safety Action Reported
Following the occurrence, Helijet International Inc. reviewed its SOPs and increased employee training, specifically on crew resource management, night VFR operations, the black-hole effect and unprepared landing sites. The company developed a risk management plan for night VFR operations. It will also be providing night vision goggles to its flight crews. The Tofino/Long Beach Airport installed the necessary infrastructure for night operations and was fully night-certified by TC in January 2017.
UPDATE 10 June 2018:Italian HEMS AW139 Inadvertent IMC AccidentWe look at the ANSV report on a HEMS helicopter Inadvertent IMC event that ended with an AW139 colliding with a mountain in poor visibility.
Aerossurance has extensive air safety, flight operations, airworthiness, safety culture development and safety analysis experience. For aviation advice you can trust, contact us at: enquiries@aerossurance.com
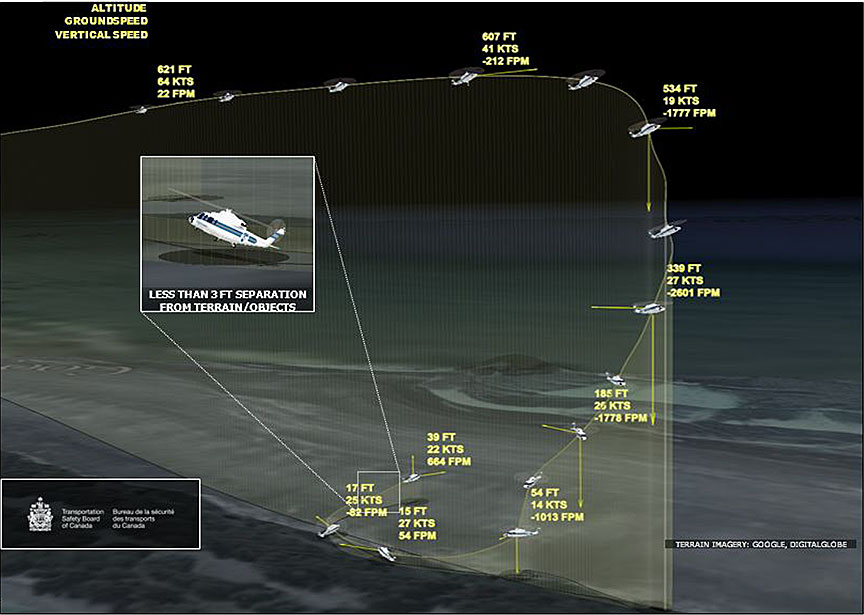
The helicopter descended at rates exceeding 2600 feet per minute (fpm), with airspeed transitioning through 0 knots forward and entering rearward values. Control was re-established over a beach, after the helicopter had descended to approximately 3 feet above ground level, and approximately 67 feet below the airfield elevation at Tofino/Long Beach Airport.

There is no normal or emergency in-flight procedure for a torque exceedance. The manufacturer does… require maintenance action after the flight.