Fatal US Helicopter Air Ambulance Accident: One Engine was Failing but Serviceable Engine Shutdown
31 January 2021
Fatal US HAA Accident: One Engine was Failing but Serviceable Engine Shutdown (Air Methods / Duke Life Flight, Airbus Helicopters BK117C2 / EC145 N146DU, North Carolina)
Wreckage of Air Methods / Duke Life Flight, Airbus Helicopters BK117C2 / EC145 N146DU near Hertford, NC (Credit: NTSB)
The Accident
The NTSB explain in their safety investigation report (issued in late January 2021), that during the flight:
…the No. 2 [SafranHelicopter EnginesArriel 1E2 turboshaft] engine experienced a bearing seizure; the engine continued to run. It is likely that the pilot then errantly shutdown the No. 1 engine and continued to fly for a brief period utilizing the No. 2 engine.
Several witnesses reported smoke trailing behind the helicopter.
It is likely that the No. 2 engine subsequently lost all power.
The helicopter then impacted a shallow turf drainage pathway between fields of tall grass on a farm, and a postcrash fire ensued, which consumed most of the helicopter structure.
The lack of any ground scars leading toward or away from the main wreckage indicated that the helicopter was in a near-vertical descent before impacting the ground. One rotor blade was found intact [and] consistent with little or no rotation of the main rotor system.
Wreckage of Air Methods / Duke Life Flight, Airbus Helicopters BK117C2 / EC145 N146DU near Hertford, NC (Credit: NTSB)
The manufacturer of the device indicated that its internal replaceable battery might have expired, which would have prevented new data from being properly stored on the memory card.
NTSB don’t examine the maintenance or ay flight data monitoring (FDM) conducted by AMC on the system. The aircraft was not fitted with nor required to carry a crashworthy recorder. NTSB note that:
The helicopter was equipped with a Honeywell Sky Connect Tracker II system that transmitted data to the DLF communications center and the [AMC Operational Control Center] OCC [in Greenwood Village, Colorado].
At the time of the accident, AMC had the Sky Connect Tracker II system configured for data transmissions emitting from the helicopter every 120 seconds. [This was not] a sufficient frequency to determine the helicopter’s track, speed, and descent profile before impact. [I]t is possible that the pilot was attempting an emergency OEI landing when the loss of power in the No. 2 engine occurred.
[T]he helicopter might have been at an altitude that was too low and/or an airspeed that was too slow to allow for a successful autorotative landing when the loss of power in the No. 2 engine occurred.
A reconstruction of witness statements using the innovative Immersive Witness Interview application from IWIindicated that “that the forward speed almost completely consumed before the vertical descent started” and “the final, almost vertical descent, started at about 500 ft AGL. This means initiation of an autorotation would have been possible at this point.”
The NTSB Safety Investigation: The Engines
Consistent with a deliberate shutdown of the No. 1 engine:
Examination of the wreckage at the accident site revealed that the No. 1 engine twist-grip throttle control in the cockpit was found in the OFF position.
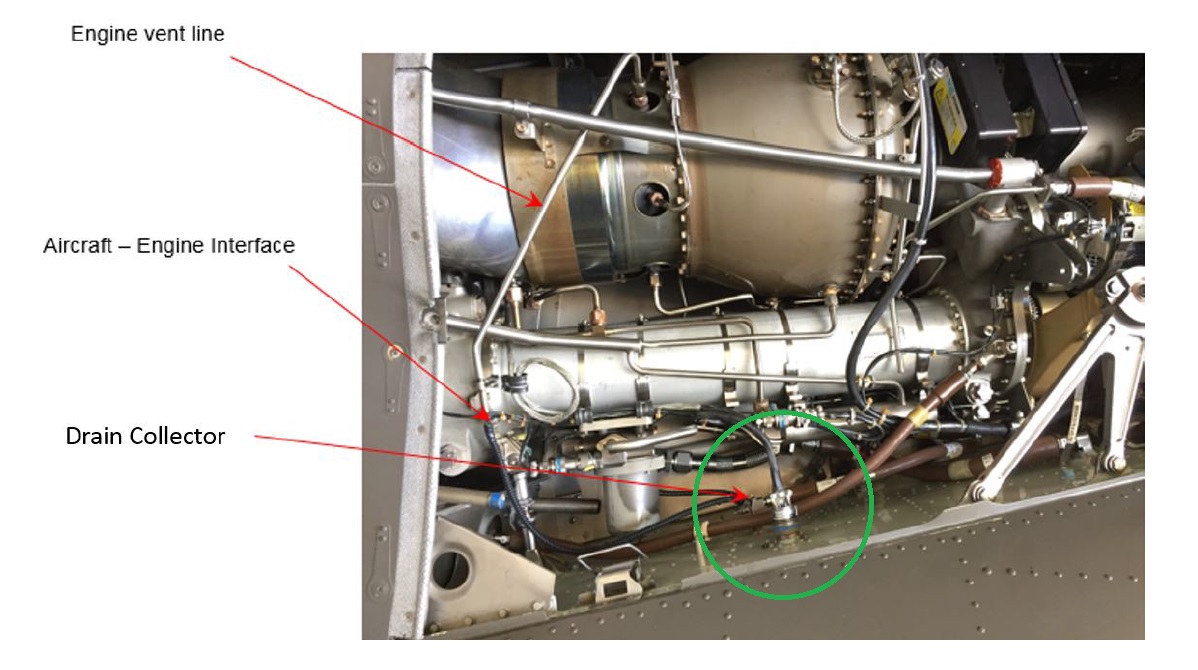
No technical issue was identified with the No. 1 engine that would have necessitated it to be shut down. It was noted that excess shrink tubing material was found obstructing the ports in the No. 1 engine 3-way deck fitting (part of the aircraft oil drain system).
Airbus Helicopters BK117C2 / EC145 3-Way Drain Fitting Highlighted (Credit: Airbus via NTSB)
Shrink tubing is allowed to be used on the deck fitting nipples before the drain tubes are attached.
Since the accident Airbus has introduced a requirement for ultrasonic cleaning of the 3-way union every 400 flying hours.
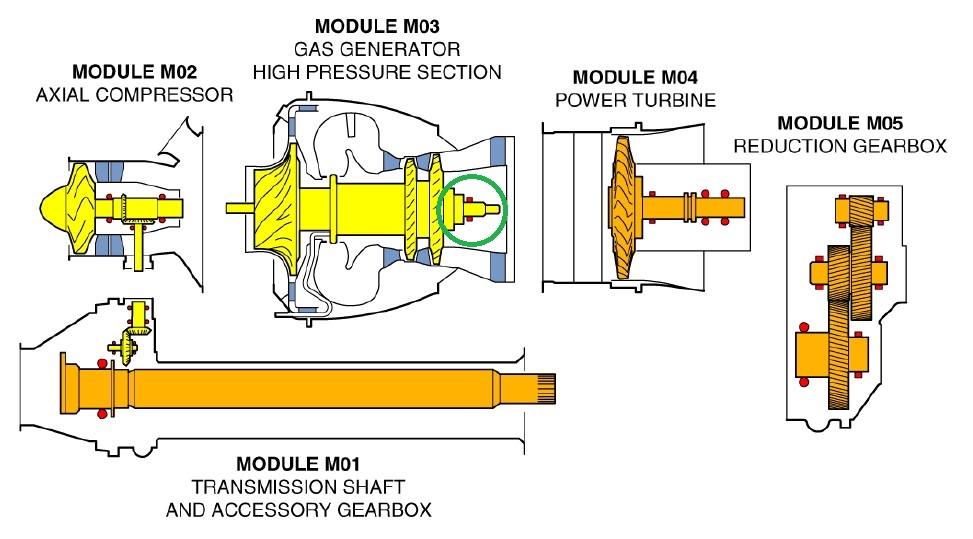
Examination of the No. 2 engine determined the gas generator shaft rear bearing was seized and damaged. Such a failure would result in smoke from the rear of the engine (although due to the damaged sustained post-impact, NTSB were unable to conclusively determine if an engine bay fire had occurred prior to impact). A bearing deterioration would also be consistent with progressive deflection of the gas generator spool and ‘grooves’ observed to have been cut in labyrinth seals by the gas generator.
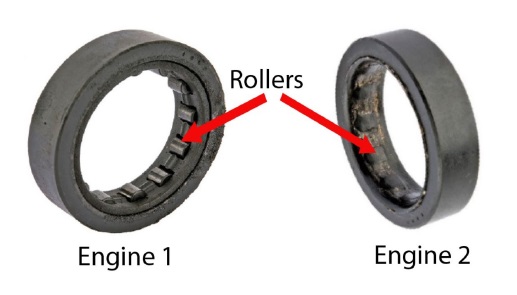
Safran Helicopter Engines (formerly Turbomeca) Arriel 1E2 Turboshaft Engine: Gas generator Rear Bearing Highlighted (Credit: Safran HE via NTSB)Arriel 1E2 Rear Bearings from Air Methods / Duke Life Flight Airbus Helicopters BK117C2 / EC145 N146DU (Credit: Safran HE via NTSB)
Coking was eliminated as a potential cause (though it had been suggested in a November 2017 FAASAIB).
The NTSB also say that:
The No. 2 engine’s oil return strainer/chip detector was partially obstructed with crystalline carbon-like and metallic debris, and debris was found downstream of the strainer in the oil pump inlet [downstream of] the rear bearing housing. The No. 2 engine 3-way deck fitting was unobstructed; however, it had been exposed to significant heat that could have decomposed the elastomeric tubing and any excess shrink tubing material, if it had been present…
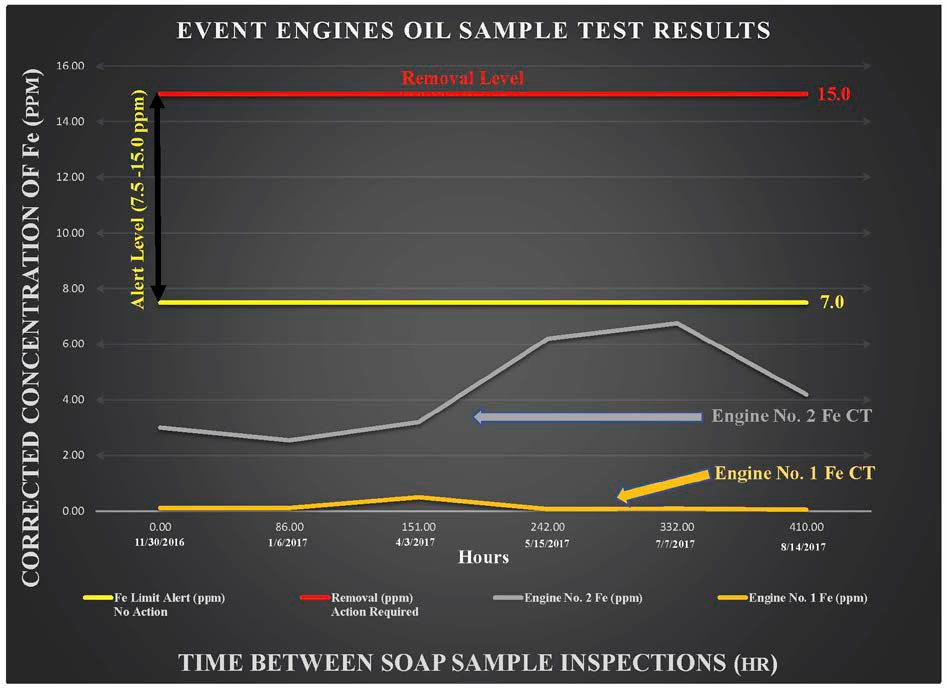
Engine spectrometric oil analysis program (SOAP) data from the 9 months preceding the accident detected contaminant levels in the No. 2 engine oil that were “considerably higher” than in the No. 1 engine albeit within limits.
SOAP Data for Safran Arriel 1E2 Engines of Air Methods / Duke Life Flight, Airbus Helicopters BK117C2 / EC145 N146DU (Credit: NTSB)
NTSB opine that trend monitoring might have detected bearing wear earlier, although they do note AMC did not record oil quantity added which would prevent accurate SOAP trending. Since the accident Air Methods have changes their SOAP procedures and now one engineer reviews all reports.
Safran, in an extensive 130-page report, identified three potential contributory factors to the bearing failure: engine mishandling during engine removal / maintenance 305 hours earlier, oil contamination and oil quality. However, ultimately the NTSB concluded that:
The root cause of the No. 2 engine’s bearing failure could not be determined due to the damage it sustained while continuing to operate before impact, and due to impact and subsequent post-crash fire damage.
The NTSB Safety Investigation: Pilot Response to Engine Failure
The lack of recorded flight data hampered the NTSB’s ability to precisely determine the sequence of events and the indications to the pilot.
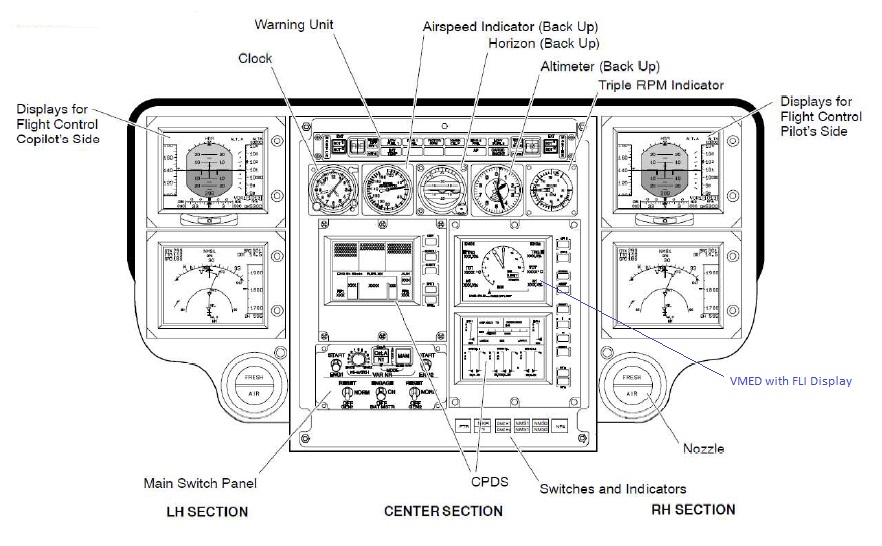
It is likely that metallic debris from the No. 2 gas generator rear bearing would have resulted in an ENG CHIP message on the helicopter’s Caution and Advisory Display (CAD) (marked as the ‘Warning Unit’ below).
Airbus Helicopters BK117C2 / EC145 Instrument Panel (Credit: Airbus via NTSB)
The helicopter’s flight manual (FLM) listed two procedures for engine chip detection: either shut down the affected engine or slowly reduce power to idle on the affected engine and monitor the engine parameters. The second option was intended to allow the pilot to potentially use the affected engine during landing.
A rear bearing deterioration would result in an increasing turbine outlet temperature (TOT) as the wear on blades and seals reduced turbine performance forcing the engine to run hotter.
This likely triggered an engine parameter discrepancy (ENG PA DIS) caution message that would have appeared in both the left (engine 1) and right (engine 2) columns on the CAD, indicating that a discrepancy was detected in one of the parameters between engine Nos. 1 and 2. The CAD message would not have indicated which parameter had a discrepancy; however, the affected parameter’s numeric value (TOT in this case) would change from white to yellow on the First Limit Indicator (FLI), described below.
The FLM procedure for the ENG PA DIS message was, “do not try and match needles, avoid using maximum power, compare the numeric values on the FLI to verify the affected parameter, and land as soon as practicable.” The FLM procedures did not request the pilot to shut down the engine.
Additional caution messages may have also appeared on the CAD. If a difference in torque between the two engines was detected at greater than 15%, a VAR NR caution message would appear in the center “MISC” column of the CAD, advising the pilot to manually match the engines’ torque values. If a difference in N1 between the two engines of greater that 10% was detected, the ENG SPLIT caution message would appear in both engine columns of the CAD. The FLM procedure for an ENG SPLIT caution message was to adjust the collective lever to one-engine inoperative (OEI) limits or below, turn off bleed air consumers, and analyze engine conditions.
The NTSB explain that the VMED is…
…an electronic display in the center of the helicopter’s instrument panel and is the pilot’s primary reference for engine power management. The central focus on the VEMD is the FLI displaying an analogue indication (tachometer-like) of the limiting parameter associated with the helicopter engine primary limitations.
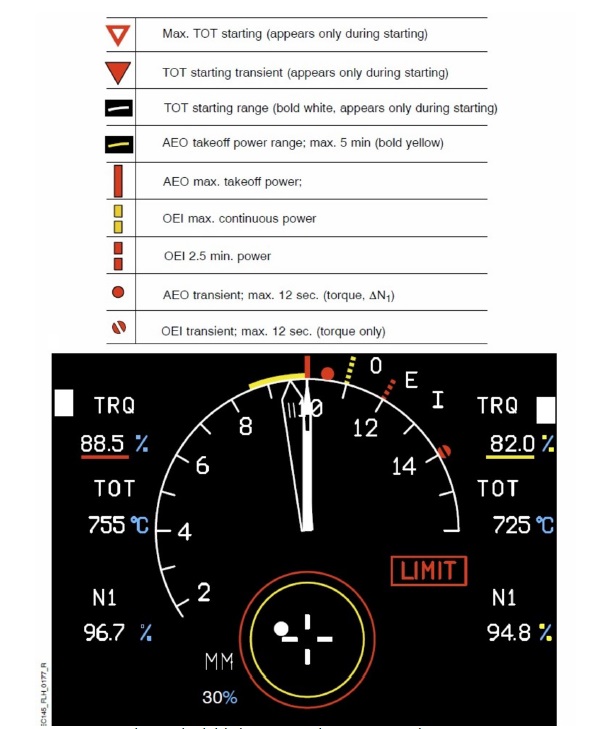
Airbus Helicopters BK117C2 / EC145 First Level Indicator (FLI) Display (Credit: Airbus via NTSB)
The VEMD’s FLI presents a needle dial gauge (needle “I” is for the No. 1 engine, and needle “II” is for the No. 2 engine) and digital numeric values for engine torque (TRQ), turbine outlet temperature (TOT), and gas generator rotational speed (N1) for each engine.
The FLI display concept is widely regarded as an extremely effective way to present the various limitations to flight crew in a concise and easily monitorable way. As the name suggests the display shows the limit the helicopter is closest to first on the basis that if the aircraft is controlled within that limit all others will be respected.
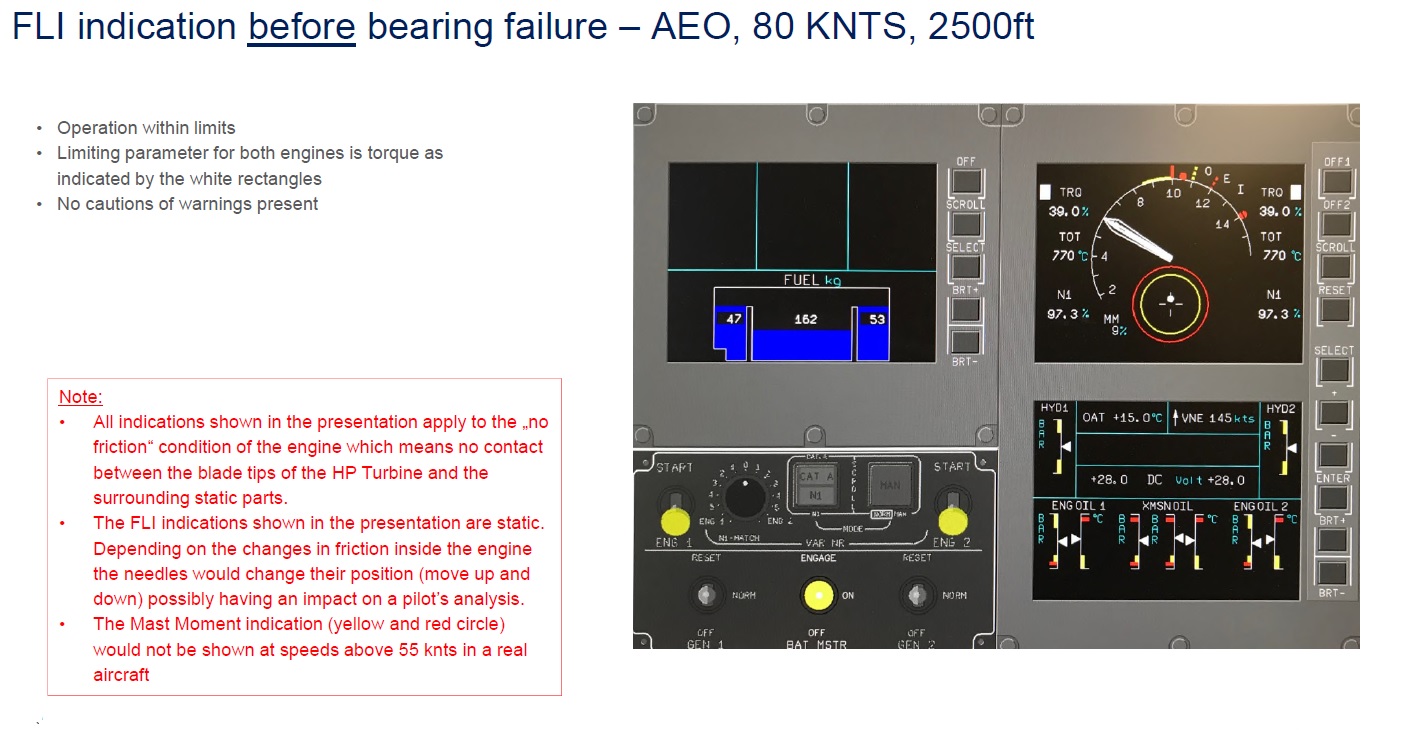
This Airbus graphic provided to NTSB shows the expected FLI display before the No. 2 engine failure became evident:
However, in this type of engine failure…
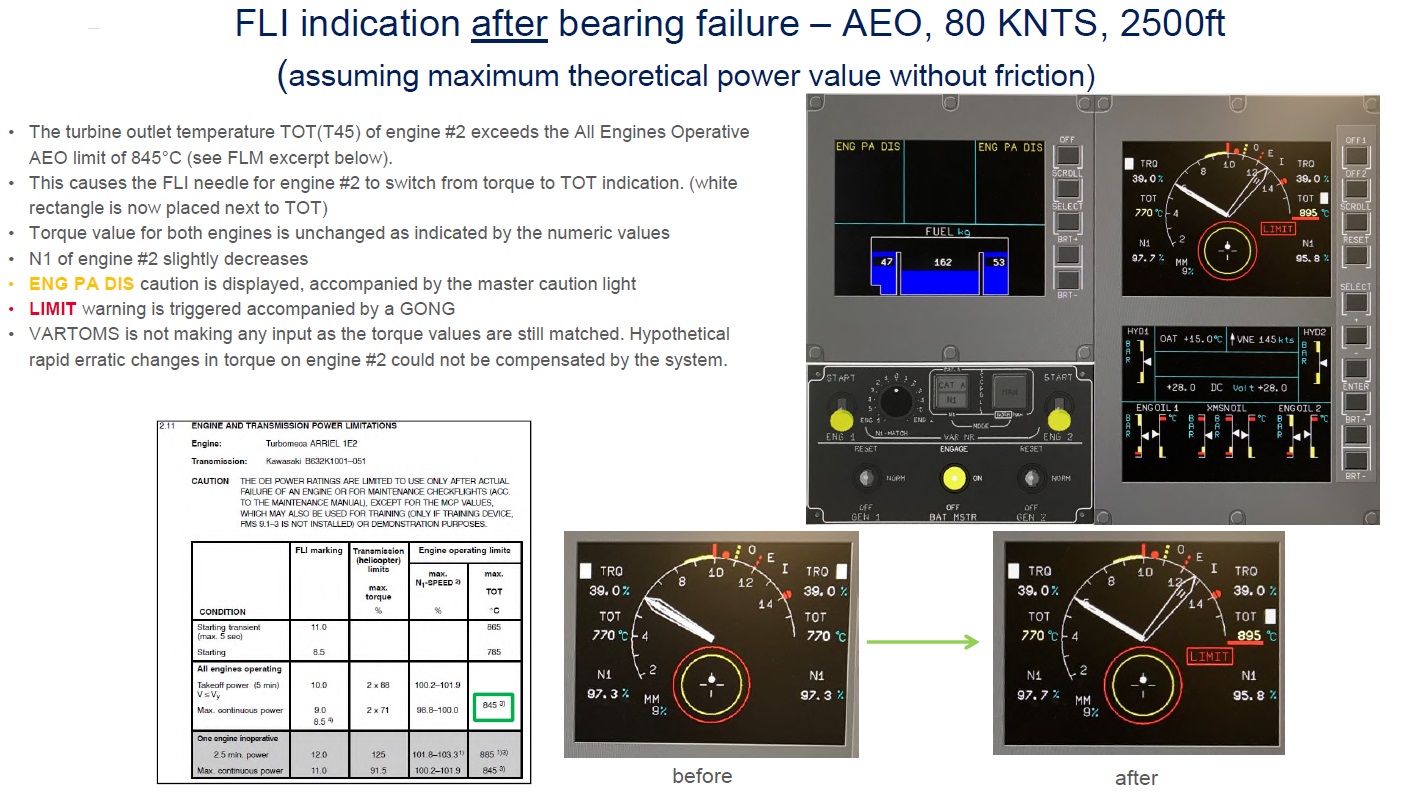
…the FLI needle for the No. 2 engine would have changed from indicating TRQ, to indicating TOT due to a sudden rise in TOT in the No. 2 engine. Such a switch would have been unusual, because the needles normally reflect TOT during engine start only. The change in the position of the No. 2 FLI needle would have resulted in a large split between both needles.
The No. 1 engine, functioning normally, would have continued to display TRQ.
In normal cruise flight, with the FLI needles both representing TRQ, a large split during cruise flight would indicate a difference in TRQ between the engines; thus, the pilot may have erroneously thought that the split was showing that the No. 1 engine was producing much less TRQ than the No. 2 engine, which might have contributed to his decision to shut down the No. 1 engine.
The NTSB note that the FLI highlights that the needle was now displaying TOT. Engine gas generator speeds are also displayed, with main rotor speed, on the triple tachometer located just above the FLI.
Once the No. 1 engine was shut down:
The NTSB Investigation: The Pilot and AMC Training
The pilot was 51, had 4562 hours total experience, 1027 on type, and had been employed by AMC since August 2009.
He was the lead pilot and the safety officer at AMC’s [Johnston Regional Airport] JNX base and an AMC maintenance test pilot in the BK117C2 helicopter.
He was also current and qualified on the twin-engine Airbus EC135 helicopter [with a similar cockpit display system], in which he had accrued 1,100 hours of total flight experience.
Before his employment with AMC, the pilot flew twin-engine SikorskyUH-60 helicopters for the US Army, accruing about 2,300 flight hours, and the EC135 helicopter for another helicopter air ambulance provider.
The pilot’s coworkers and managers provided positive feedback about his performance. He was described as professional, well prepared, thorough, and team oriented, and he exhibited good pilot skills
The pilot had been type trained by Air Methods. NTSB note that the circumstances of the failure encountered was not practised in their training programme.
AMC training records indicated that the pilot had completed all required training with no deficiencies.
However:
Recurrent training typically included autorotations, which were practiced to a power recovery at a 3-ft hover, but no autorotations were specifically documented in the pilot’s recurrent training records.
At the time of the accident, AMC did not have a BK117C2 simulator training program, which would allow for practice autorotations to touchdown.
The absence of simulator training also prevented practical training with a wide range of emergencies. Disappointingly, NTSB investigation do not examine pilot training and its effecviveness further.
NTSB Probable Cause
A failure of the rear bearing in the No. 2 engine, which (1) created multiple and likely unexpected and confusing cockpit indications, resulting in the pilot’s improper diagnosis and subsequent erroneous shutdown of the No. 1 engine, and (2) the resulting degraded the performance of the No. 2 engine, until it ultimately lost power. The complete loss of engine power likely occurred at an altitude and/or airspeed that was too low for the pilot to execute a successful emergency autorotative landing.
Wreckage of Air Methods / Duke Life Flight, Airbus Helicopters BK117C2 / EC145 N146DU near Hertford, NC (Credit: NTSB)
On 4 February 2015 TransAsia Airways (TNA) ATR 72-600B-22816, Flight GE235, crashed in Taipei with the loss of 43 lives. About 36 seconds after takeoff the No 2 engine auto-feathered and about 46 seconds later the No 1 engine no.1 was shut down (final report).
Prior to the morning of the accident N1QF was designated as the standby helicopter; however, the primary helicopter was scheduled for maintenance on the day of the accident, therefore essential equipment had to be moved from the primary craft to N1QF. Before the transfer could be accomplished, N1QF was required to prepare for dispatch on the accident flight. What was later described by a witness as a “hasty dispatch,” necessitated a hurried departure to accomplish the transfer of equipment, complete a preflight,and other items necessary for a medical evacuation flight.
The flight departed at 1003 to fly from the airport to the near by hospital. It crashed less than 4 minutes later.
Eyewitnesses observed the accident helicopter during the final few seconds of the flight. Two witnesses stated that the helicopter was trailing smoke from the area of the engines. One witness indicted that the helicopter was maneuvering just prior to the impact and that during the final descent which he described as “dropped like a stone,” it appeared the rotor blades were “not turning hardly at all.” Witnesses reported that the helicopter was nearly silent just prior to ground impact and that there was no engine noise at all after impact.
The NTSB probable cause was:
The pilot’s failure to obtain/maintain a successful autorotation. Factors were: a loss of engine power of one engine for undetermined reasons, and the pilot’s shutdown of the wrong engine.
Aerossurance has extensive air safety, operations, SAR, HEMS, airworthiness, human factors, aviation regulation and safety analysis experience. For practical aviation advice you can trust, contact us at: enquiries@aerossurance.com