Wrong Engine Shutdown Crash: But You Won’t Guess Which!
12 April 2019
Wrong Engine Shutdown Crash: But You Won’t Guess Which!
A British airliner, an engine problem and the crew inadvertently shutting down the wrong engine, crashing close to the airfield. Kegworth in 1989 right? Well sorry for the click-bait title but that is not thishuman factors case study, which predates that accident by almost exactly 20 years.
BUA BAC One-Eleven G-ASJJ 14 January 1969: The Accident Flight
On the evening of 14 January 1969, British United Airways (BUA) BACOne-Eleven, G-ASJJ was due to depart Milan Linate bound for London Gatwick. According to the Italian investigation report (published in English as CAP347 and in ICAOCircular 118-AN/88) the aircraft had been due to have landed in Genoa. However, due to bad weather it had been forced to divert to Milan Linate, landing at 14:30. The crew, who had also flown a Gatwick-Rotterdam-Gatwick service earlier in the day, were been forced to wait 5 hours for the outbound passengers to arrive by coach from Genoa. They had been on duty since c 06:30 local time (c 05:30 UK time), i.e. 14 hours when the passengers arrived.
There were three flight deck crew, all experienced Captains:
Captain A occupied the left-hand seat as ‘pilot-in-charge‘ (who had 10973 flying hours in total and 497 hours on type).
Captain B was in the right hand seat as co-pilot (12135 hours total, 33 hours on type).
Captain C, a Training Captain, was in the centre supernumerary seat as ‘pilot-in-command‘, ultimately responsible for the safe operation of the aircraft (13360 hours total, 2153 hours on type).
There was no requirement in the UK Air Navigation Order for the commander to be seated at the controls.
The investigators note:
Before leaving Gatwick Captain A briefed Captain B concerning the co-pilot duties assigned to him. Although Captain C, as pilot-in-command, did not himself formally brief Captains A and B there was no doubt that they were aware of their respective tasks.
At 2018 hours, after clearance from Linate ATC, the engines were started and engine anti-icing selected “ON”. There was a considerable layer of snow along the sides of the taxiways and runway, but they themselves were clear…
V1 and Vr had been calculated as 117 kt and V2 at 127 kt with the chosen 18° flap setting. The aircraft was cleared for take-off at 20:31 hours.
V1 and Vr were called and the aircraft was rotated into the initial climbing attitude.
BAC One-Eleven Cockpit (Credit: Mike McBey / CC BY 2.0)
Immediately after…a dull noise was distinctly heard by all the crew members. This noise was variously described by them as: “not like a rifle shot, not like the slamming of a door or something falling in the aircraft but more like someone kicking the fuselage with very heavy boots, an expansive noise covering a very definite time span with a dull non-metallic thud”.
The bang was immediately associated by the crew with the engines. After looking at the TOT gauges, and observing that No. 1 engine was indicating a temperature 20°C higher than that of No. 2 engine, Captain C said: “I think it’s number one” or words to that effect, and after a brief pause “throttle it”.
On receipt of Captain C’s comment Captain A closed the power lever of No. 1 engine.
During or just after the explosion, he had completed the rotation manoeuvre and the aircraft was climbing at 12º of pitch with reference to the flight director. As a precaution, after closing No. 1 power lever he reduced the angle of climb to 6º. At the same time the co-pilot (Captain B) who had reached for the check list and was looking for the page relating to an engine emergency, became aware of a sharp reduction in the aircraft’s acceleration; he noticed that the undercarriage was still down and he retracted it immediately.
According to the crew the aircraft reached a maximum height of 250 ft, after which a progressive loss of momentum became evident. A maximum speed of 140/145 kt was achieved immediately after rotation, but it fell to 127 kt after No. 1 engine had been throttled back. These figures were consistent with those subsequently derived from the flight recorder. The crew said that the stick-shaker operated three times between 125 and 115 kt.
The co-pilot [Captain B] had a vague recollection that the stick-push and the warning klaxon operated during the critical phase before impact. The pilot-in-charge [Captain A] remembered vaguely that someone said “raise the flaps”, but no crew member remembers doing so or making the retraction.
On looking out of the aircraft the crew saw the ground and the obstructions close at hand and realized that contact of the aircraft with the ground was inevitable and imminent.
Captain A controlled the aircraft extremely well during the touchdown; the aircraft slid along the snow-covered surface, passing over small obstructions, and came to a halt 470 m from the point of first contact with the ground.
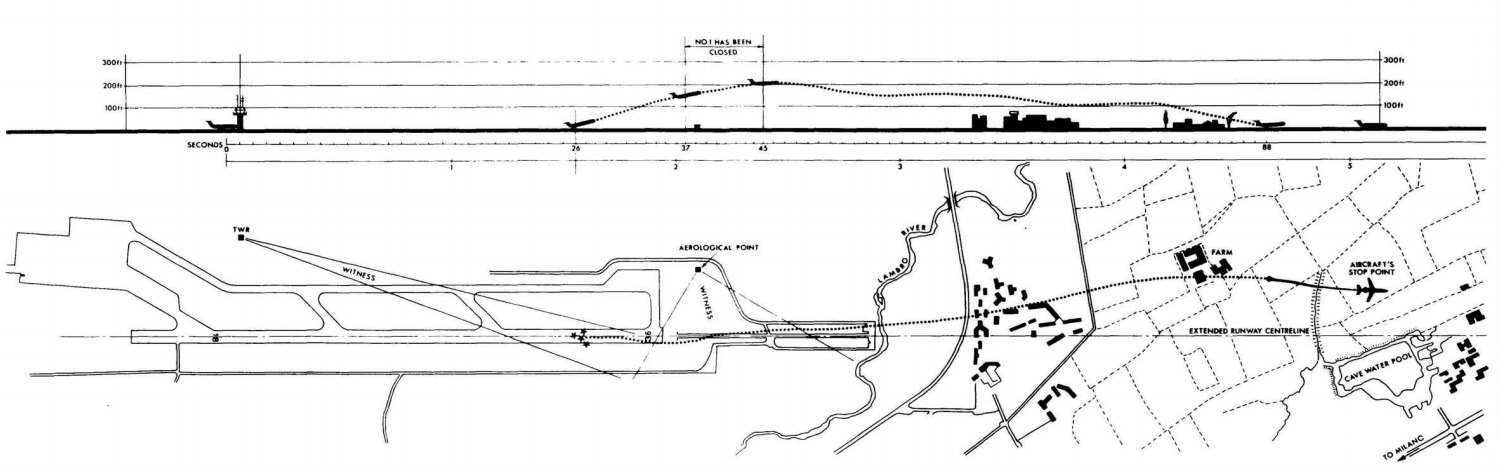
BUA BAC 1-11 G-ASJJ Flight Path (Credit: Italian Investigation Report via ICAO)
The co-pilot [Captain B] operated both engine fire-extinguishers and Captain C ordered the pilots to leave the aircraft immediately via the side windows.
The aircraft fortuitously force landed in open farmland that was covered in snow and sodden from recent winter weather (photo). Six passengers were injured but the other 26 occupants escaped injury.
The evacuation was described by investigators as “exemplary” although as no distress call had been made and no one witnessed the landing, it took rescuers an hour to find the wreckage in the dark and rain.
Flight Data
The aircraft was equipped with a Sperry Airborne Data Acquisition System (SADAS) flight data recorder (FDR). This recorded Indicated Airspeed (IAS), pressure altitude, magnetic heading, normal acceleration and pitch attitude.
Examination of the initial part of the flight showed that acceleration during the take-off run, up to rotation speed, was normal for a BAC 1-11 with 18° flap and that there was no deficiency in thrust up to the time of rotation. For about 10-12 seconds after unstick, which occurred about 26 seconds after release of brakes, the thrust exceeded the drag and the energy increased. The energy reached a maximum at about 37 to 38 seconds from release of brakes and then decreased steadily, showing that the drag exceeded the thrust.
The data [was] consistent with an acceleration up to rotation speed with both engines at maximum thrust and a normal take-off, followed immediately by a rapid reduction of about 30 per cent in the total thrust.
About 37 seconds from release of brakes, there was another reduction in thrust, compatible with the throttling back of No. 1 engine, and the undercarriage was retracted, after which the aircraft lost height and/or speed so that the total energy decreased during the remainder of that period of time.
Engine Strip Reports
No problems were found with the No. 1 Rolls-RoyceSpey Mk 506 engine (the engine shut down).
Inspection and testing of No. 2 engine showed that a segment of the HP turbine seal had become detached and had fouled the turbine blades. This fouling caused the stream of sparks clearly seen by eyewitnesses. The technical examination and testing established that the displacement of the seal segment caused a surge in the low pressure compressor which was clearly heard by the aircraft’s occupants as a dull explosion.
The surge was of very short duration and any decrease in thrust would have returned to at least 97 per cent of the original power within 1/10 second. Unless the crew members had been looking at the engine instruments precisely at the time of the bang, it is highly improbable that they could have seen any fluctuation in the indications of these instruments.
Extensive tests did not reveal any fuel system issues that would account for a thrust loss.
Analysis of Power Loss and Human Factors
An analysis of the tests carried out and an accurate and detailed examination of the fuel consumed during the test programme lead to the conclusion that the loss of thrust revealed by the data obtained from the flight recorder, over and above that caused by the deliberate throttling down of No. 1 engine, might have been caused by a reduction in the flow of fuel to No. 2 engine within 10 seconds of the bang/surge.
The investigators say a a likely reason for this reduction in No. 2 engine thrust…
…could have been the inadvertent displacement of the throttle lever of when No. 1 throttle lever was pulled back, or its inadvertent displacement in some other way which cannot be established. On the other hand, the total energy calculations reveal two discrete reductions in thrust, the first of which, equivalent to about 30 per cent of the total thrust, occurred about 3 seconds after the aircraft left the ground. The effects of this reduction were greater and more prolonged than would be the case if the bang/surge were the sole reason.
After the intervention of the pilot-in-command [Captain C] and the subsequent throttling back of No. 1 engine, the crew had no reason to suspect a defect in No. 2 engine as well and in these circumstances the partial throttling of No. 2 engine passed unnoticed. The crew’s attention would have been diverted from the engine instruments by the sudden operation of the stall warning round about 125 kt, 30 seconds before impact with the ground.
Up to the time of the bang/surge, the pilot-in-command [Captain C] had played a completely passive role. The bang, distinctly heard by the crew, was immediately associated by them with an engine failure so that they were, so to speak, “preconditioned”. When Captain C looked at the engine instruments he did not notice anything abnormal except that, in his opinion, the TGT of No. 1 engine was indicating a temperature 20°C higher that that of No. 2. This convinced him that No. 1 engine was malfunctioning and he said so to the crew. When the co-pilot [Captain B] heard Captain C say “I think it’s number 1” and a few seconds later “throttle it”, he had the impression that these remarks were addressed to Captain A in a conversational tone and not as a direct and precise order. Captain A, however, interpreted these remarks as a direct order from the pilot-in-command.
The Company’s instructions stated that in the case of an engine malfunction on take-off, not accompanied by fire, nothing should be done by the pilot-in-charge or the co-pilot before a safe height is reached.
The Company’s Training Manual did not specifically define any safe height, because of the various climatic and topographical conditions under which an aircraft is operated, but each pilot was instructed during training to;
– reach V2 before retracting the undercarriage
– reach a safe height before beginning the appropriate emergency drill.
This safe height had been assessed to be about 700 ft for the weather and topographical conditions at Milan/Linate at the time of take-off.
The investigators say:
Captain A, in answer to a question as to what his reactions would have been if the pilot-in-command [i.e. Captain C] had not been present, stated that he would have left everything until a safe height [and] the co-pilot should by then have positively identified the failure. It was therefore believed that his erroneous reactions were due in no small measure to the presence of the pilot-in-command [Captain C] in the jump seat. Captain C stated:
“It is perhaps not quite correct to be ultimately responsible for the safe handling of an aircraft in an emergency unless occupying a seat from where this can be done. I feel, somehow, that had I been occupying either of the pilot’s seats I might have reacted differently; on the other hand, it is possible that had I not been present the two pilots might also have reacted differently.”
They also note that:
Although Captain C was not suffering from exhaustion, his fatigue could have affected his powers of analysis, thereby contributing to his hasty and erroneous diagnosis of an engine malfunction, which, in turn, initiated an inopportune, incorrect and wholly prejudicial course of action.
Investigator’s Probable Cause
The accident must be attributed to a combination of factors following a compressor bang/surge in No. 2 engine immediately after take-off and the aircraft crashed because the crew, after fully closing No. 1 throttle in error, failed to recognize their mistake and, in addition, were not aware that the thrust of No. 2 engine had also been partially reduced after an inadvertent displacement of the relevant throttle lever.
Safety Recommendations: Crewing, Instruments and Human Factors
Three recommendations were made:
1) The intervention of the commander, or check pilot, supernumerary to the normal crew at the controls, appears to have been a distracting factor to the pilots in the correct performance of their duties. A state of subjection resulting from the presence of a pilot with supervisory duties [Captain C] seems to have constrained the crew at the controls, and in particular the pilot-in-charge [Captain A], to accept orders or advice, without any contribution on their part of the competency of which they were certainly capable, for a calm identification of the causes of the bang which they had heard and for the application of the appropriate company drills. Attention is therefore drawn to the advisability of reconsidering the position of a supernumerary pilot and his tasks and responsibilities, with particular reference to the question of whether or not it is desirable for the aircraft commander to be seated at one set of the controls.
2) The accident to G-ASJJ once again raises the question of erroneous corrective action taken by pilots immediately after an emergency has arisen; such action is almost always prompted by equivocal reading of the aircraft’s instruments, particularly when the reading and subsequent interpretation is made under stress. Although in the case of G-ASJJ there is scant evidence to support a conclusion that engine instrument presentation misled the commander, it is thought that some indication that a temporary fault had occurred in No. 2 engine might have been of assistance to the crew and decreased the possibility of an erroneous assessment, particularly under conditions such as those which obtained when the bang/surge occurred. It is, therefore, recommended that every effort should be made to lessen the possibility of aircraft accidents occurring due to erroneous interpretation of the readings of aircraft instruments which, although seemingly rational and functional in design, still mislead reliable and experienced pilots.
3) The accident shows to what extent the human factor has a decisive effect on the sequence of events. The tragic experience of the past has provided ample evidence that it is not enough to establish adequate emergency procedures in order to cover the widest range of technical contingencies. When confronted with unexpected and difficult flight conditions, human weakness tends to prevail over the reasoning powers of experienced men, suddenly and dramatically faced with mortal danger. It is therefore, recommended that all suitable means be adopted to enable pilots to obtain an adequate knowledge of human factors which, as much experience has already shown, will be conditioned by the particular environment in which they operate.
The second recommendation is very prescient in relation to Kegworth (in particular) and recommendation three notably predates a series of accidents in the 1970s that stimulated the conception of Crew Resource Management (CRM), including:
1978: UnitedDC-8 N8082U crashed after running out of fuel over Portland, Oregon, while…fault finding a landing gear issue
On 4 February 2015 TransAsia Airways (TNA) ATR 72-600B-22816, Flight GE235, crashed in Taipei with the loss of 43 lives. About 36 seconds after takeoff the No 2 engine auto-feathered and about 46 seconds later the No 1 engine no.1 was shut down (final report).
On 6 April 2016 Arall Aerolineas Llaneras Douglas DC-3HK-2663 was destroyed by fire following a forced landing in Columbia. The Grupo de Investigación de Accidentes & Incidentes Aéreos de Colombia (GRIAA) investigation report concluded the accident was due to:
Wrong application by the crew of the emergency procedure due to engine No. 1 failure, since they reduced the RPM of the operative engine (No. 2), causing the BMEP limit to be exceeded, producing an engine stall (No. 2), making the flight of the plane impossible and forcing the execution of a forced landing.
UPDATE 18 July 2023: The NTSB has released their report into the ditching of cargo 737-200N810TA off Hawaii on 2 July 2021. The Probable Cause was determined to be:
The flight crewmembers’ misidentification of the damaged engine (after levelling off the airplane and reducing thrust) and their use of only the damaged engine for thrust during the remainder of the flight, resulting in an unintentional descent and forced ditching in the Pacific Ocean.
Contributing to the accident were the flight crew’s ineffective crew resource management, high workload, and stress.
Aerossurance has extensive air safety, operations, airworthiness, human factors, aviation regulation and safety analysis experience. For practical aviation advice you can trust, contact us at: enquiries@aerossurance.com