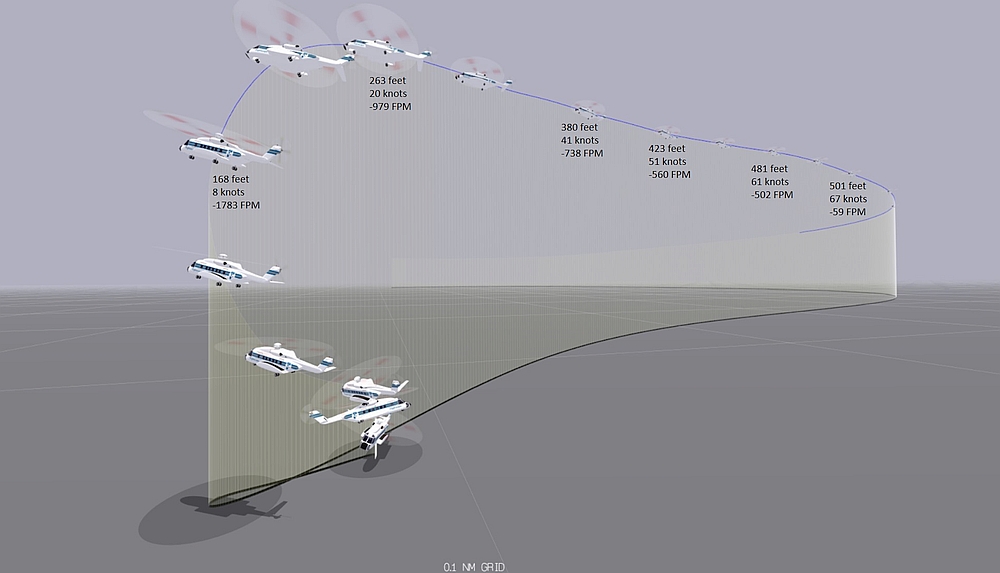
A high-rate-of-descent and low-airspeed condition developed in low-visibility conditions. As the helicopter descended below 250 feet it was in a steep, 800 fpm descent, at very low airspeed. When the Pilot Flying (PF) instinctively increased the collective, the helicopter’s rate of descent rapidly increased to 1800 fpm. At just 40 feet the helicopter yawed through 845° and the offshore helicopter, with 13 persons on board, came within just 13 ft of the sea before starting to climb.
Descent LOC CHO Sikorsky S-92A C-GICB (Credit TSB)
There was then a second loss of control during the subsequent ascent with the aircraft unintentionally descending from 1350 ft to 480 ft.
The Serious Incident Flight: First Two Approaches
The Transportation Safety Board of Canada (TSB) explain in their safety investigation report (released on 27 April 2021) that the flight had originally been scheduled for 22 July 2019, but was postponed due to low clouds and poor visibility at the destination.
CHO Sikorsky S-92A C-GICB (Credit: Ryan Sharpe)
The crew reported at 0545 on 24 July 2019 for a 0700 scheduled departure from Halifax/Stanfield International Airport (CYHZ). Low clouds and poor visibility resulted in a further delay.
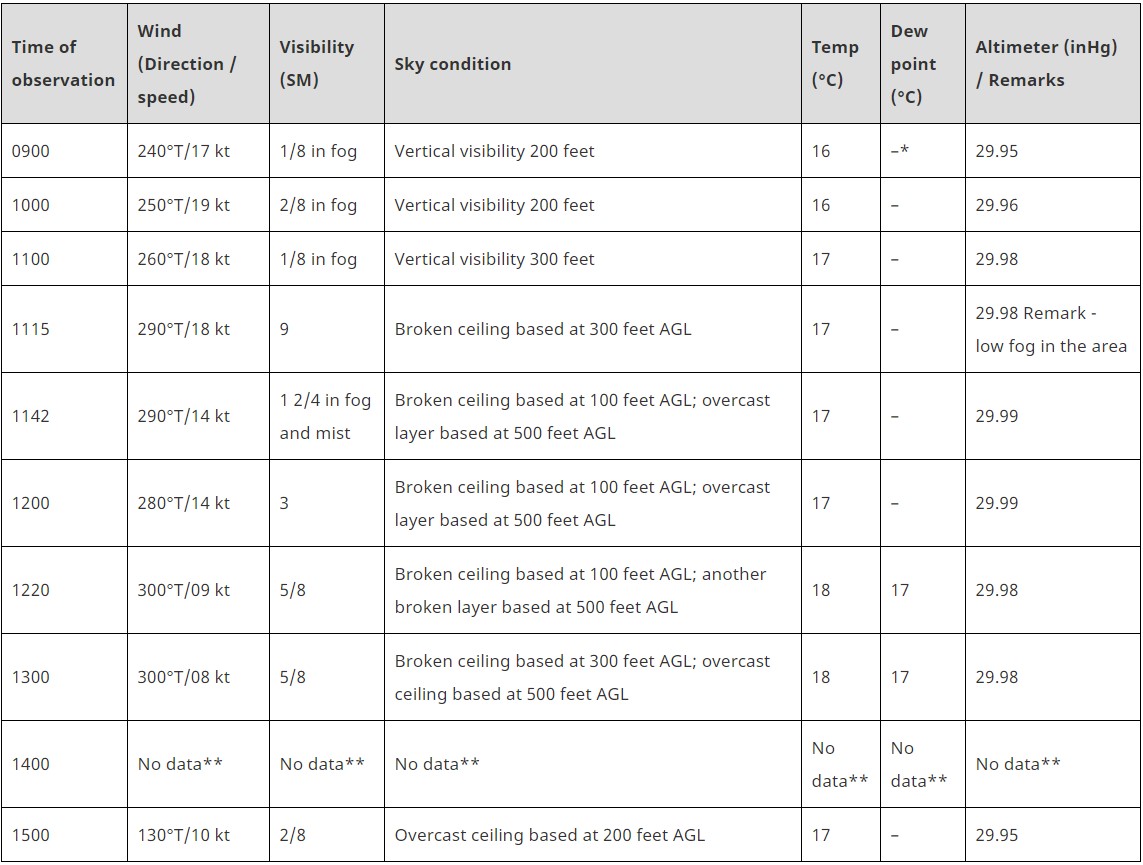
Weather reports issued for the ExxonMobil Thebaud Central Facility on the day of the occurrence (Credit: TSB)
The flight finally departed at 1154 to TCF, approximately 155 nautical miles to the east-southeast. On board were the two flight crew and 11 passengers. The aircraft commander had flown 6713 hours, 2242 on type. The co-pilot was also a captain and had flown 7742 hours, 3196 on type. Oddly the TSB refer to the co-pilot as a ‘first officer’ throughout.
At approximately 1240, the weather observer on the TCF informed the pilots that the winds were approximately 300° true (T) at 8 knots, the visibility was 1 statute mile (SM), and there was an overcast ceiling based at 300 feet above ground level (AGL); however, the cloud layer and visibility were fluctuating rapidly.
Two instrument [Airborne Radar Approaches (ARA)] approaches were attempted at the platform but both were unsuccessful due to low clouds and poor visibility.
For these two approaches, the captain (occupying the right seat) was the pilot flying (PF) and the first officer (occupying the left seat) was the pilot monitoring (PM).
Thebaud Complex in Good Visibility (Credit ExxonMobil via TSB, with TSB annotations)
The Serious Incident Flight: The Visual Approach and Loss of Control
Approximately 15 seconds after initiating the second missed approach, at approximately 300 feet RADALT, the helicopter exited the cloud, horizontally.
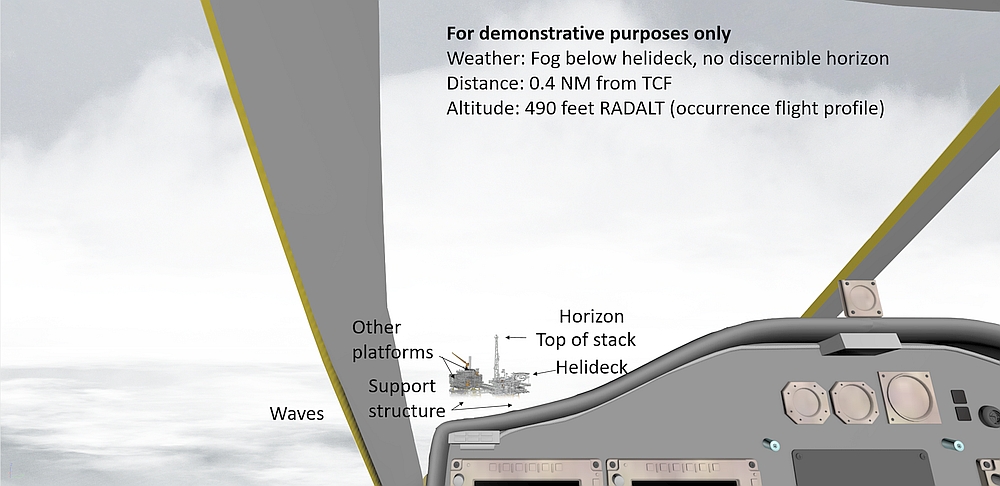
The PM informed the PF that the helideck, which is 174 feet above the water, was visible above the ragged layer of fog beneath them. Although the TCF was in sight, there was no discernible horizon. As the helicopter climbed away, the PF looked across the cockpit [to the left] and also observed the helideck above the fog layer.
…the pilots levelled off (engaged RADALT hold at 500 feet) and commenced a right-hand turn, using the heading hold autopilot mode, to assess the feasibility of conducting a visual approach. While the aircraft was in the turn, the airspeed, which was coupled to 80 KIAS in the climb to 500 feet RADALT, was reduced to 66 KIAS.
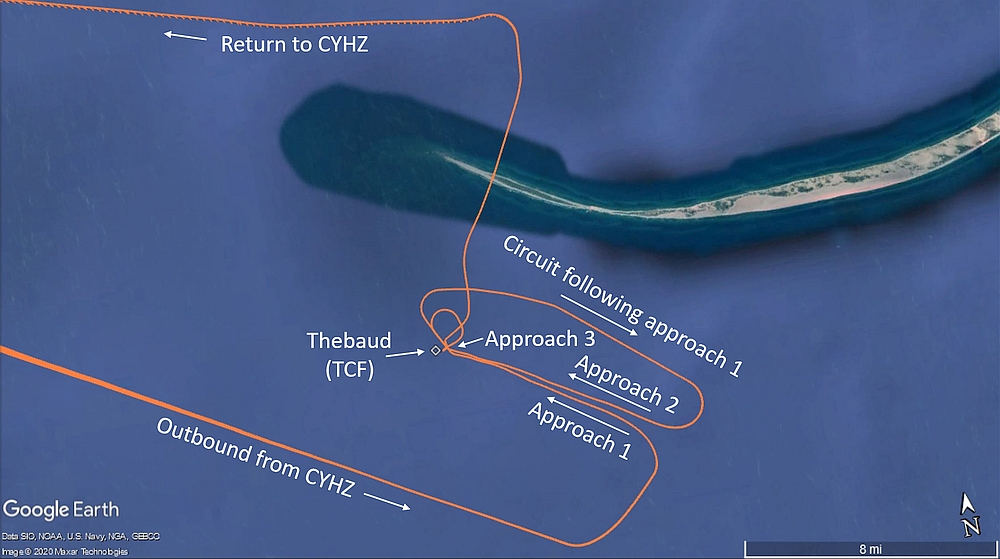
At 1332:15, approximately 1.1 nm from the TCF, the helicopter rolled out on a heading of 182°M and the crew planned their third approach.
As the wind was light the flight crew agreed that rather continuing to orbit and come out on a inbound track of 320°M they would turn right early to roll out on an inbound track of approximately 240°M. Since the TCF would be on the left-hand side of the helicopter it was decided the co-pilot would be PF for this approach. The crew also decided to remain at 500 feet RADALT.
There was a ragged layer of fog below the helicopter and a scattered-to-broken layer of cloud at least several hundred feet above it. The pilots could see the water through the fog, directly beneath the helicopter.
Flight Path CHO Sikorsky S-92A C-GICB (Credit TSB)
At approximately 1332:23 the helicopter commenced a right turn andthe aircraft commander, stated he would be ready to transition to instrument flight if fog rolled in and the co-pilot lost sight of the helideck.
At 1332:55, when the helicopter was 0.6 NM from TCF, it rolled out on final approach, on a heading of 271°M. The helicopter was level at 46% engine torque, coupled to RADALT at 500 feet and 61 KIAS. The airspeed and groundspeed were approximately the same.
Because the first officer was seated in the left seat it was only now he had visual contact with the TCF. As the helicopter rolled out, commander transferred control to the co-pilot.
The helicopter was still flying above the fog layer, and both pilots had a clear line of sight to the helideck. The estimated flight visibility was approximately 3 statute miles in the direction of the TCF; however, there was no discernible horizon behind the TCF.
At 1333:02, when the helicopter was 0.5 NM from the TCF, the captain (who was now the PM) disengaged the airspeed mode, then the heading hold mode at the PF’s request.
At 1333:04, the PF depressed the cyclic autopilot disengage button to disengage the RADALT hold, then depressed and held the cyclic trim release button to hand-fly the approach. At the same time, the PF lowered the collective (decreased from approximately 45% engine torque to 27% engine torque), using the collective trim release trigger, to commence the descent.
TSB explain that:
The descent commenced when the helicopter was 0.43 NM from the TCF, on a 7.1° approach angle to the helideck. The PM recognized that the approach was steeper than the company’s standard 4.7° approach angle; however, it did not alarm the PM because some company pilots preferred flying a steeper visual approach profile. The PF asked the PM for the helicopter’s groundspeed, to which the PM replied it was approximately 60 knots.
However, 7.1° is less than the maximum in the S-92A RFM procedure for landing on an elevated helideck. That specifies a maximum rate of descent of 600 fpm at 40 knots indicated airspeed (KIAS) i.e. a maximum approach angle of approximately 8.4°.
At 1333:06, when the helicopter was 0.4 NM from the TCF, its rate of descent was 500 feet per minute (fpm) and increasing. To reduce the helicopter’s forward speed, the PF applied aft cyclic, causing the helicopter’s pitch attitude to increase to 12° nose-up. The PM informed the PF that the groundspeed was about 40 knots, which he considered to be slightly high given the light winds and the helicopter’s proximity to the TCF.
The PF did not acknowledge this call. At the same time, left cyclic and right pedal inputs were being progressively applied, creating lateral drift to the left (i.e., south) of the intended track and right yaw, which kept the nose of the helicopter pointing in the direction of the helideck (so that the helicopter was side-slipping left).
At 1333:14, when the helicopter was within 0.3 NM of the TCF, at 415 feet RADALT, its pitch attitude increased to 15° nose-up. Two seconds later, the pitch attitude increased to almost 17° nose-up, and the helicopter briefly banked 6° to the right.
During that time, the PF’s attention was focused outside, looking at the helideck. The PM, who had been primarily focused on the helideck, shifted his attention inside the helicopter and onto the flight instruments because he was losing sight of the helideck, (given that he was occupying the right-hand seat). The PM recognized the nose-up pitch attitude and, in accordance with company SOPs, called “15 degrees”. As this was happening, the airspeed decreased below 40 KIAS. The rate of descent was 670 fpm and increasing. Neither pilot was aware of the increasing rate of descent, the low engine torque setting of 27%, or the increasing left sideslip.
At 1333:20, the PF increased collective to 36% engine torque and the pitch attitude decreased to approximately 12° nose-up, even though the PF was applying increasing aft cyclic. Pedal input moved momentarily toward neutral, then increased to the right again. The PM continued to monitor the helicopter’s pitch attitude as it was reduced. The helicopter was at 350 feet RADALT, at low airspeed (i.e., less than 30 KIAS), descending at approximately 850 fpm.
Below 35 knots airspeed indication is considered unreliable.
At 1333:26, at 250 feet RADALT with the helicopter at approximately 12° nose-up, all forward motion had been lost, and the rate of descent was 1200 fpm, and increasing. The sideslip angle reached approximately 40° nose right, with 18 knots lateral groundspeed.
The PF recognized the helicopter was getting low and slowly increased collective to 45% engine torque, then rapidly increased to 103% engine torque, and applied cyclic opposite to the right bank (caused by sideslip), peaking at 22° right bank. As engine torque increased from 45% to 103%, at low airspeed, the rate of descent increased from 1200 to 1800 fpm as the helicopter descended below the helideck height; about 3 seconds after the engine torque reached 100%, the descent rate began decreasing (below 1500 fpm).
The PF did not verbalize that he had lost visual contact with the helideck. The PF shifted his attention to the flight instruments and observed the low airspeed and high rate of descent. The PM, who was initially unaware that the helicopter had descended into the fog and that the PF had lost visual contact with the helideck, observed the increasing rate of descent and informed the PF. At that point, the PM recognized that the helicopter was in the fog. The PM was just about to call for a go-around when the PF stated that he was commencing a go-around. During this time, the helicopter’s pitch attitude increased to almost 17° nose-up. The PM directed the PF to position the nose of the helicopter on the horizon, using the attitude indicator on the PFD.
The PM became aware of the proximity to the surface as they descended below 100 feet. Recognising the severity of the situation he “placed his hands and feet on the flight controls and made control inputs to help the PF establish a wings-level attitude in anticipation of water impact”.
At 1333:33….passing through 70 feet RADALT, the collective lever was rapidly raised to the full up position and engine torque increased to 146% [so called ‘blowaway power’].
Descent LOC CHO Sikorsky S-92A C-GICB (Credit TSB)
The “LOW ROTOR” aural alert activated at 95% Nr (main rotor rpm). Nr drooped to 77% and was below 95% for 20 seconds. The low Nr also resulted in a reduction of tail rotor thrust so directional control was lost. At just 40 feet the helicopter yawed right through 845° over a period of 55 seconds, despite full left yaw pedal input. The peak yaw rate was about 80°/second.
In this perilous situation the low Nr had another side effect, namely the main generators dropped offline…
…causing the automatic flight control system (AFCS) to revert to stability augmentation system (SAS) mode, the helicopter’s attitude and heading reference system (AHRS) to drop offline, and the helicopter’s centre and left-side (first officer) multi-function displays (MFDs) to display blank screens. As a result of these system failures, both pilots reverted to using the standby flight instruments.
At 1333:39, with the helicopter yawing to the right (greater than 60°/second), and Nr slowly increasing through 89%, the generators came back online and the pilots were able to arrest the descent within 13 feet or less of the water…
Water spray was visible on the helicopter’s windows.
Second Loss of Control: Ascending
The captain, who could see the water and the TCF to the right of the helicopter, formally took control of the helicopter and began a near-vertical visual climb up to 150 feet RADALT, crosschecking with the standby instruments due to reduced visibility in fog. Some right yaw persisted during the climb and gradually reduced as the helicopter continued to climb. The aircraft flew in a widening right turn away from the vicinity of the upset and toward the northeast, accelerating from 30 KIAS to 80 KIAS.
A high-power setting (110–120% engine torque) was maintained during the initial climb and the Nr slowly increased, generally returning to 105% Nr at around 375 feet RADALT. As the helicopter climbed above 650 feet RADALT, engine torque was reduced to 100%, and continued steadily downward to approximately 70% as the helicopter reached 1350 feet RADALT.
At 1334:55, the helicopter’s altitude peaked at 1350 feet RADALT, then it began descending and the airspeed increased to 125 KIAS. While this was happening, the pilots attempted to engage barometric altitude hold twice; however, in both instances it failed with a master caution light. They also pressed the AFCS mode reset button on the AFCS control panel 8 times, without success.
Unbeknownst to the pilots, airspeed had increased to 148 KIAS, while descending through 650 feet RADALT at 1700 fpm. The PF recognized and arrested the descent at approximately 480 feet ASL (463 feet RADALT) as the helicopter was passing over the northwestern tip of Sable Island [ c 10 ft AMSL].
The captain then increased collective to regain the lost altitude. The pilots were unaware that the helicopter had overflown Sable Island. The helicopter was levelled off at 1500 feet ASL and the pilots assessed their options. Knowing that there were low clouds and visibility in the vicinity of the TCF and Sable Island, the pilots decided to return to CYHZ, where weather conditions would permit a visual flight rules (VFR) approach to landing.
Once the helicopter’s systems returned, several minutes later,the pilots observed the “APU GCU FAIL”, “DCU MISCOMPARE”, and “LIMIT EXCEEDED”caution lights… The pilots recognized the AFCS was degraded, which made the helicopter more difficult to fly accurately [but] did not detect any other unusual controllability problems with the helicopter. The pilots believed that the cautions were related to the engine torque during the descent, so they elected to continue back to CYHZ without additional troubleshooting.
The captain coupled the helicopter’s autopilot to airspeed, heading, and altitude for the transit back to CYHZ. The flight crew elected not to declare an emergency. The aircraft then returned to Halifax/Stanfield International Airport without further incident.
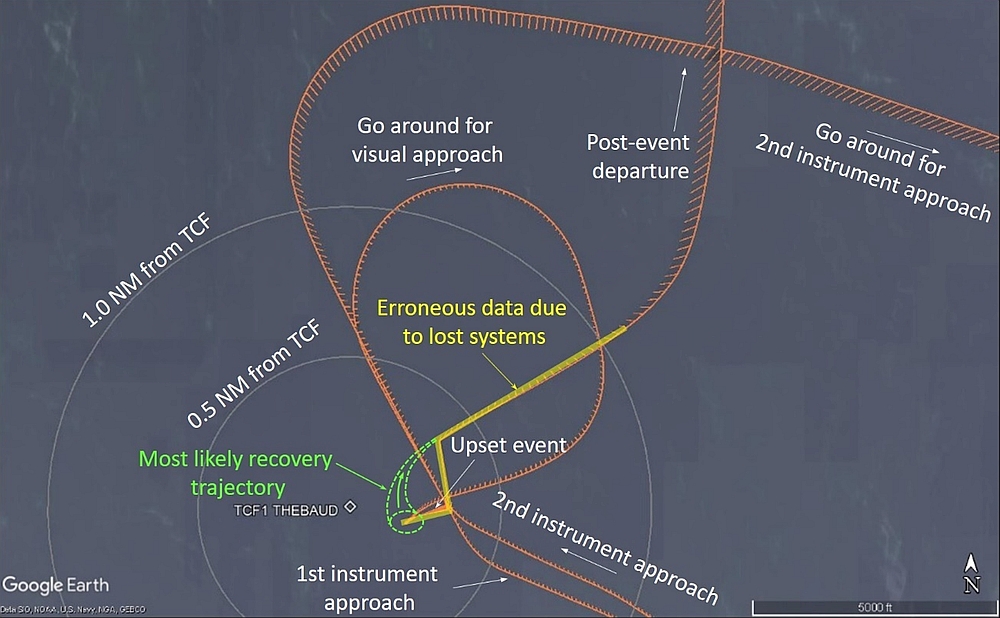
Plot showing CHO Sikorsky S-92A C-GICB’s approach paths (Credit: TSB)
However, shortly after the occurrence, CHO ceased operations. The TCF was decommissioned in 2020 after a 3-year plug and abandonment project, with the Heerema Marine Contractors heavy life vessel Thialf removing all the installations.
The TSB Safety Investigation
TSB Safety Investigation: Loss of Cockpit Voice Recording & Lack of Cockpit Video
While Flight Data Recorder (FDR) information was available, the TSB investigation was hampered by a lack of Cockpit Voice Recorder (CVR) data:
Due to the APU GCU FAIL condition, the pilots could not start the APU in accordance with the normal shutdown procedure. After some delays, the shutdown was carried out 23 minutes after landing, 96 minutes after the inadvertent descent.
In order to preserve the recording for the investigators and in accordance with the CHO Operations Manual:
One of the pilots, in conjunction with a technician, removed power from the system by pulling the CVR/FDR circuit breakers. The aircraft was moved into the hangar and placarded to indicate that it was quarantined.
However, seemingly without the permission of the TSB, the next day….
…the manufacturer requested that CHO provide them with the FDR and data for analysis. This was to be done remotely by the company that owns the occurrence helicopter. A representative from that company told CHO maintenance personnel that electrical power would have to be applied to the helicopter to carry out the required downloads.
CHO maintenance personnel questioned those instructions, out of concern for the preservation of CVR data; however, they were assured by the representative that only FDR/HUMS data would be downloaded. The circuit breakers were pushed in and the remote FDR/HUMS download was carried out.
Unfortunately while doing this:
The CVR was powered for 54 minutes during, and after, this process. During that time, the CVR was overwriting itself and all CVR data for the occurrence were lost. When the TSB received the recorders for download, the CVR audio started approximately 30 minutes after the occurrence, while the helicopter was in level flight, on the return portion of the flight.
TSB also note that:
Although not required by regulation, the occurrence aircraft was equipped with a lightweight recording system. The [Outerlink IRIS] system is “a comprehensive, lightweight, monitoring, recording and next generation satellite communications system providing voice, video, analog and digital aircraft system information.” The unit provides a continuous recording loop of at least 30 hours, which is stored on a secure digital card. It records information from up to 3 high-definition internet protocol cameras and 5 audio sources.
For reasons that are not elaborated, this system…
…was not operational at the time of the occurrence flight.
TSB Safety Investigation: Organisational Background, SMS and FDM
CHO was a division of Canadian Helicopters Limited (CHL). In 2015, CHO (then doing business as Helicopters (New Zealand) Global under CHL) began operating in Halifax, Nova Scotia, providing offshore helicopter transportation to the offshore oil and gas industry. In 2018, the company began operating under the trade name Canadian Helicopters Offshore.
At the time of the occurrence, CHO operated 2 Sikorsky S-92As out of CYHZ, and employed 10 pilots, 9 maintenance personnel, 16 support personnel, and 8 management staff (pilots, engineers, safety and quality, and administration). CHO ceased operations in 2019, shortly after the occurrence.
CHO had a Safety Management System (SMS) but as an SMS is not a regulatory requirement for operators like CHO in Canada, it was not audited by Transport Canada. CHO had also implemented a helicopter flight data monitoring (HFDM) program too:
A review of the parameters monitored revealed that there were several offshore approach parameters; however, the distance for the final leg of a visual approach, or the glide path angle flown were not parameters that were monitored. As a result, the company had no way of determining if its pilots were adhering to the visual approach procedure, and adhering to the CHO’s stabilized approach criteria.
The investigation determined that some pilots did not always adhere to the prescribed visual approach final distance, nor was the 4.7° glide path always followed. The company’s HFDM program did not actively use available…data to detect these types of deviations from company SOPs.
TSB Safety Investigation: Dynamic System Condition Not Assessed
The rotor and rotor drive system components from C-GICB were sent to Sikorsky for examination to assess their condition after this serious incident but remarkably during an active safety investigation:
Because the helicopter was no longer required by CHO (which was leasing the helicopter), the owner of the helicopter elected not to conduct further inspections and the manufacturer did not complete an engineering analysis of the rotor and drive system components. As a result, the extent of the damage resulting from the over-torque was unknown at the time of [TSB] report writing.
TSB Safety Investigation: Crew Background, Decision Making and Sterile Cockpit Procedures
The flight crew…
….had known each other for several years and flew together periodically. Both pilots had a considerable amount of confidence and respect in each other’s abilities as a pilot. The investigation determined that there was a strong sense of team and alignment of mental models throughout most of the occurrence flight. The pilots interacted and coordinated activities with considerable ease and efficiency. At no time did either pilot feel that he was being put in an uncomfortable situation. There were no indications of issues related to trans-cockpit authority gradient.
Confidence in each other, experience in operating offshore in fog and the goal (i.e. landing on the TCF’s helideck) suddenly appearing achievable during the second missed approach as the helideck suddenly became visible may have all contributed to the decision to attempt the third approach say TSB. Additionally…
…the lack of comprehensive visual approach briefing criteria may have played a role in the flight crew’s decision to attempt an offshore visual approach to a helideck sitting above a layer of fog and surrounded by cloud.
….required pilots to refrain from non-essential activities during critical phases of flight or during any operational task. [It] stated that “the PM actively monitors the flight profile.
However, CHO pilots…
…interpreted this to mean that heading, altitude, airspeed, or torque information was not communicated by the PM unless there was some type of unplanned deviation, or it was specifically requested by the PF.
TSB also say:
Although not contributory to the occurrence, the investigation identified discrepancies and overlapping information in CHO’s SOPs that could have led to confusion in the cockpit.
TSB Safety Investigation: Unstable Approach and First Loss of Control
The TSB concluded that, undetected by the crew, the S-92A entered a ‘low-energy state’ during the visual approach, namely:
…it was flying at low airspeed with a high rate of descent, a nose-up pitch attitude, and at a low power setting.
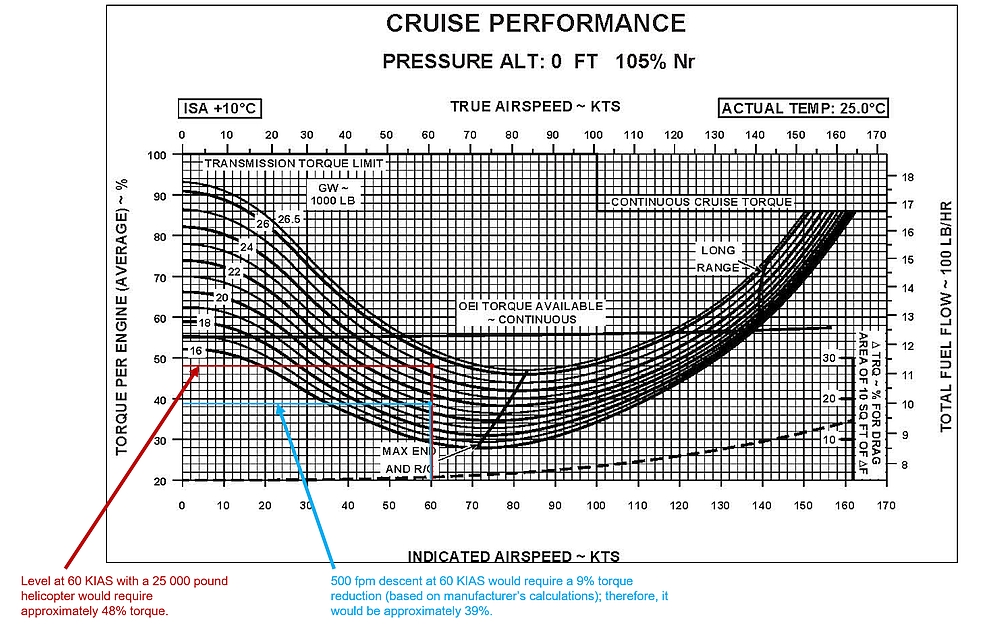
A performance study showed that:
…at the helicopter’s weight and in the environmental conditions at the time of the occurrence, an engine torque setting of 48% would have been required to maintain altitude at 60 KIAS on final for the visual approach. A 500 fpm descent (the maximum rate of descent per the stabilized approach criteria) at 60 KIAS would require a reduction of engine torque setting to 39%.
TSB annotations on the Sikorsky S-92A RFM cruise performance chart for the CHO C-GICB occurrence conditions (Credit: TSB)
However, as airspeed continue[d] to decrease…more torque would be required as the helicopter slows down, to maintain a constant rate of descent (i.e., maximum 500 fpm). As a result, the 27% engine torque used in this occurrence was significantly lower than the minimum power required to remain below the maximum rate of descent of 500 fpm, during the final approach.
The investigation determined that the pilots were unaware of the torque setting (27%) during the final descent, before entering the fog bank.
The crew were focused on the helideck, which was above the fog but in an area without a discernible horizon.
The TSB determined that this degraded visual environment (DVE) made it difficult to recognise that this was an unstable approach due to ‘attention narrowing’.
Research has shown that the accuracy of pilot judgement is diminished in a DVE. When the terrain is obscured by phenomena such as fog, pilots may have difficulty assessing height, speed, and distance due to the lack of terrain features and reduced optic flow. Likewise, without additional references such as the horizon or other structures surrounding the helideck (i.e., peripheral visual cues), a pilot’s judgement of attitude and height can also be diminished, and vertical or lateral deviations can go undetected, increasing the risk of spatial disorientation.
If the sight picture of the helideck is the only external visual reference, pilots can become fixated on it. However, if pilots become fixated on the outside cues “…changes on instruments can be missed. These missed changes can lead a pilot to believe that their knowledge of their position and trajectory in space is accurate. This belief leads to a reduction in the search for new information or information to the contrary.”
As outside visual cues diminish, workload increases and pilots must progressively rely on their flight instruments and/or stability systems, backing up visual manoeuvres by cross-checking flight instruments to ensure the accuracy of visual perception.
TSB comment:
The lack of explicit direction [in the CHO Operations Manual] with regards to operating in a DVE may have made it difficult for pilots to fully understand the risks associated with attempting the visual approach in IMC.
TSB explain:
CHO’s SOPs identified 6 conditions for a stabilized approach. Of those 6 conditions, the only 2 criteria that could be objectively applied to a visual approach were that the helicopter must be configured for landing, and it must have a maximum rate of descent of 500 fpm, unless a higher rate had been briefed.
Unlike some operators that specify minimum torque values during the approach (e.g., minimum 40% by 300 feet above the landing spot), CHO’s SOPs made no reference to energy state in its stabilized approach criteria. As a result, CHO’s procedures did not address one of the critical elements of a stabilized approach identified by HeliOffshore, an organization of which CHO was a member.
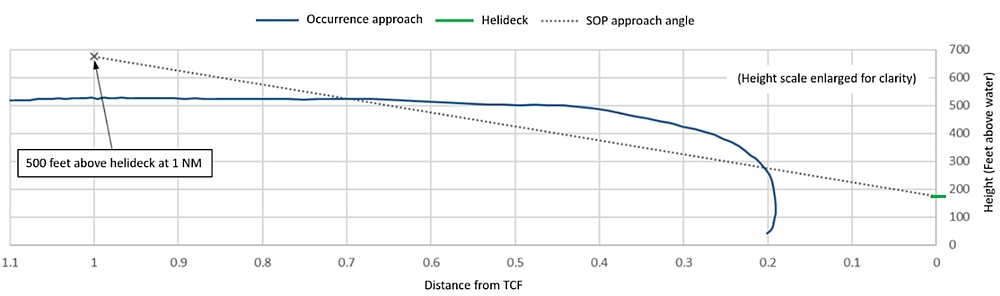
According to the company, a constant-angle (4.7°) descent was flown until just prior to reaching the helideck. When conducting a visual approach to the TCF, the SOPs required the helicopter be established on final 1 NM from the facility, at 675 feet RADALT, at a speed of 75 KIAS, depending on the winds.
In this occurrence, the visual approach began at 500 feet RADALT. Six seconds after the descent commenced, the helicopter was 300 feet above the landing elevation and the rate of descent was 520 fpm, increasing up to a maximum of 1800 fpm. Based on these descent rates, the occurrence flight exceeded CHO’s stabilized approach criteria.
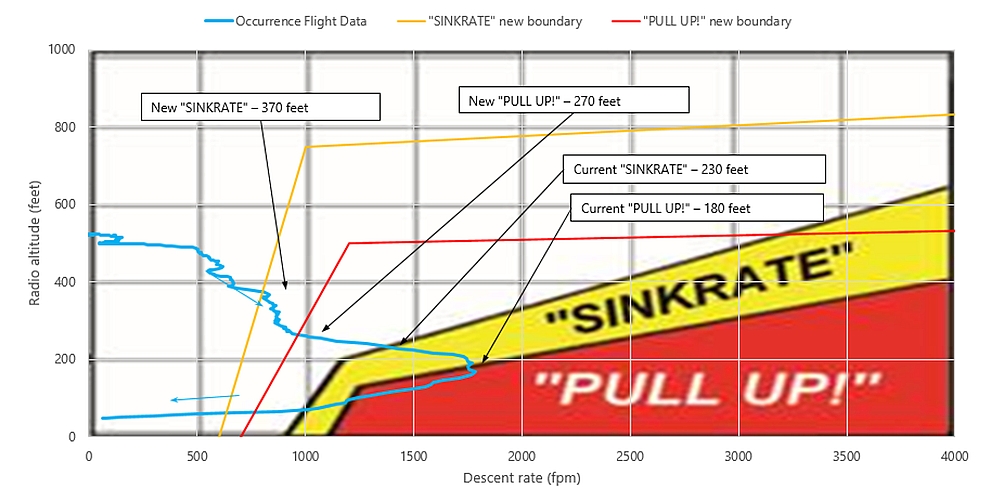
The investigation determined that some CHO pilots flew steeper visual offshore approaches than CHO’s standard 4.7° descent angle. A comparison of the occurrence descent profile with the SOP descent profile is shown below.
At 0.7 NM, while in the turn to final, the occurrence helicopter flew through the 4.7° descent angle; however, the descent was not commenced until the helicopter was 0.43 NM from the TCF, resulting in an initial approach angle of 7.1°.
Also:
…by levelling off at 500 feet RADALT and beginning the right turn to assess the conditions, the pilots lost sight of the TCF behind them during a portion of the turn.
This resulted in the helicopter rolling out at approximately 1 nautical mile (NM), with the TCF off the helicopter’s right side. When the turn to final was completed and the descent commenced, the helicopter was at 0.43 NM from the TCF at a higher-than-normal airspeed. This significantly reduced the time available…to ensure a stable approach.
When the descent was initiated, pilot workload increased quickly as more aggressive handling was required to acquire the appropriate sight picture in close proximity to the TCF. Shortly after commencing the descent, the rate of descent exceeded 500 fpm, indicating an unstable approach according to CHO’s SOPs. The approach remained unstable until the helicopter descended into the fog bank.
Furthermore:
Contributing to the difficulties encountered, CHO standard operating procedures (SOPs) made no reference to energy state in its stabilized approach criteria, increasing the risk of a low-energy state developing and going undetected. Unlike some operators, CHO’s stabilized approach criteria did not include formal nose-up or nose-down pitch attitudes when in VMC or IMC. Additionally, CHO had not adopted the [HeliOffshore] recommended practice of requiring crews to check and verbally confirm that the approach was stable at specific intermediate progress targets (typically referred to as gates) on final approach.
As a result, the SOPs provided flight crew with insufficient guidance to ensure that approaches were being conducted in accordance with industry-recommended stabilized approach guidelines.
TSB explain that:
As the helicopter descended below 250 feet RADALT, it was in a steep, 800 fpm descent, at very low airspeed, with power being applied. When the pilot flying (PF) instinctively increased the collective to reduce the helicopter’s rate of descent, that action exacerbated the situation and the helicopter’s rate of descent rapidly increased to 1800 fpm. This left the pilots with very little time (about 3 seconds) to recognize what was happening and to attempt to recover before the helicopter descended into the fog.
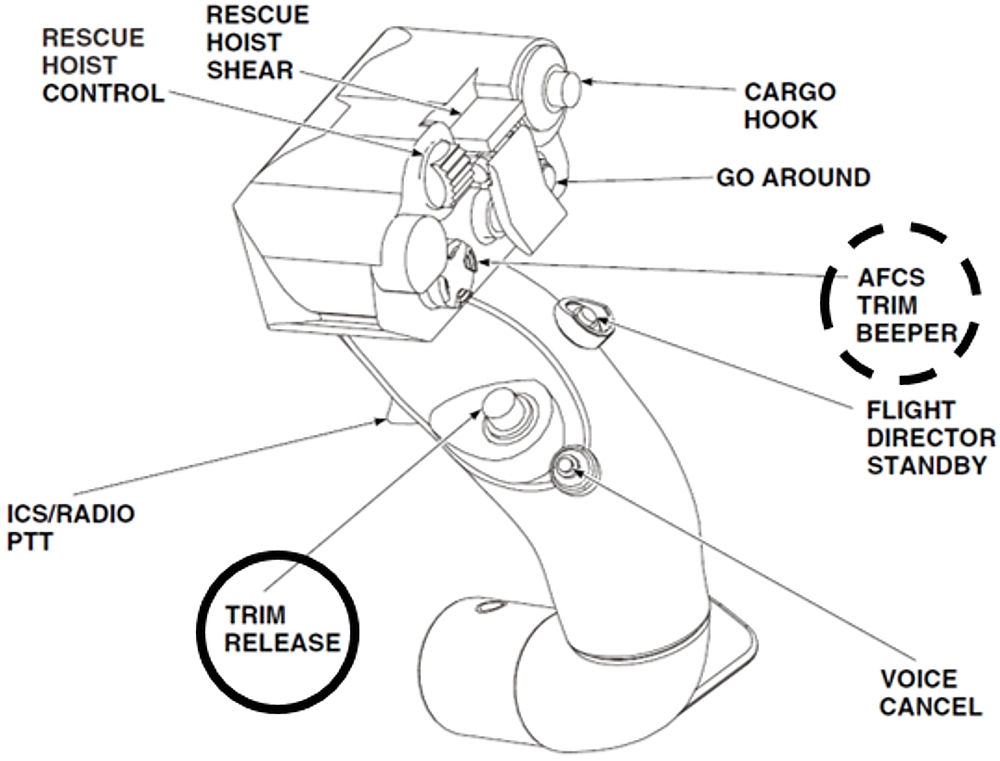
During the approach the Pilot Flying had depressed and held the cyclic trim release.
Neither the S-92A rotorcraft flight manual (RFM) nor CHO’s SOPs warned of the potential hazards associated with, or offered recommendations for, the use of the trim release button under conditions such as DVE.
Sikorsky S-92A cyclic stick, trim release (solid circle); trim beeper switch (dashed circle) (Credit: Sikorsky RFM via TSB, with TSB annotations)
Pressing and holding the cyclic trim release button disengages the magnetic brake, which provides artificial feel. This allows the pilot to move the cyclic with very little resistance. However, it also eliminates the flight control’s referenced detent to the trimmed pitch and roll attitude. As a result, with the button depressed, the stick will not return to its previously trimmed position if the pilot reduces pressure on the cyclic. In essence, depressing and holding the cyclic trim release button reduces the level of AFCS augmentation, since the pilot is required to interpret the external visual cues and/or instrument indications and then manually manipulate the controls to make any attitude changes, without the benefit of any type of attitude hold function.
CHO…considered this a pilot technique issue, and allowed pilots to decide whether or not they wanted to make maximum use of ATT mode and the beeper trim switches or to depress and hold the cyclic trim release. Some CHO pilots preferred to conduct non-coupled visual manoeuvres with the trim release button depressed. Others preferred to make maximum use of the force trim as a way of reducing pilot workload during visual approaches. Some of the pilots using the force trim would set an attitude of approximately 7.5° nose-up, using ATT mode, then either make small inputs against the force trim force gradient, or use the beeper switch for minor adjustments during the descent.
As seen in previous occurrences [e.g. AS365N G-BLUN in Morecambe Bay 27 December 2006,S-92A C-GQCH departing Sea Rose , this technique reduces the overall effectiveness of the automatic flight control system (AFCS). In this occurrence, the helicopter reached a nose-up attitude of 17°, an excessive rate of descent, and an increasing left sideslip while on final approach.
Flying the visual approach in a DVE while depressing and holding the cyclic trim release button increased pilot workload and contributed to control difficulties that resulted in an unstable approach.
TSB also postulated that:
The PF was likely subtly incapacitated due to spatial disorientation following the helicopter’s rapid, unexpected descent into the fog layer. As a result, recovery action was initially delayed until the pilots acquired visual contact with the water and the collective was rapidly increased to arrest the descent.
TSB Safety Investigation: Recovery and Second Loss of Control
Both pilots were making control inputs during the final portion of the descent.
Despite this, the crew was able to successfully arrest the descent, avoiding impact with the water. However, from a crew resource management [CRM] standpoint, it is important to recognize that a positive transfer of control reduces the risk of pilots making opposing control inputs. This is particularly important when one pilot may be suffering from some type of incapacitation, where it could interfere with or prevent the appropriate flight control inputs being made.
As the helicopter climbed…
…a second inadvertent descent occurred as the helicopter reached 1350 feet radar altitude (RADALT). At that time, the flight crew was attempting to reconcile what had just happened and determine what systems had been lost during the event. Because of this, the flight crew experienced a momentary lapse of attention that allowed an inadvertent descent rate to develop. As the flight crew established that the helicopter was still controllable, the pilots recognized the inadvertent descent and corrective action was taken.
TSB Safety Investigation: Absence of Terrain Avoidance and Warning System (TAWS) Warnings
When helicopter descended with a very high rate of descent the TAWS fitted, a HoneywellMk XXII Enhanced Ground Proximity Warning System (EGPWS), did not alert the crew even though EGPWS Mode 1 was designed “to detect when the aircraft is descending toward terrain at a high rate for its relative altitude above terrain.”
So why did the original Mode 1 not alert the crew? Simple, it is inhibited on all S-92As.
According to Sikorsky, Mode 1 was prone to nuisance alerts on the S-92A during initial certification testing in 2002. Consequently, Sikorsky asked Honeywell not to include Mode 1 in the S-92A configuration of the Mk XXII EGPWS. The Mode 1 envelope was subsequently updated in 2003 [Honeywell software version EGPWS-020] to address previous concerns about nuisance alerts; however, Mode 1 remained inhibited on the S-92A. The investigation determined that the Mk XXII is installed in many different helicopter types; however, the S-92A is the only Mk XXII-equipped helicopter with Mode 1 inhibited.
It was only 16 years later, that after simulator evaluation, did Sikorsky decide to begin the process to enable Mode 1 according to the TSB. This is not the only significant safety compromise made during the development of the S-92A in 2002. Another, replated to loss of lubrication testing featured in the fatal loss of an S-92A and 17 people in Newfounland in 2009.
In March 2020, Honeywell issued a Service Bulletin to introduce software version EGPWS-036 that addresses recommendations made by the UK Civil Aviation Authority (UK CAA) that will dramatically improve warning performance, including Mode 1 for offshore helicopters (where it would provide a warning 9 seconds earlier). TSB state:
Sikorsky plans on incorporating EGPWS-036…when it installs version 11 of the avionics management system (AMS), anticipated for U.S. and worldwide release in late 2021 and early 2022, respectively. The manufacturer did not specify how long it would take for AMS version 11 to be installed across the S-92A fleet.
In relation to those modes that were enabled, by design they were suppressed at low speed with the gear down so didn’t activate, disabling what should have been a valuable safety net.
TSB Findings as to Causes and Contributing Factors
At the time of the occurrence, instrument meteorological conditions existed. This created a degraded visual environment that was highly conducive to spatial disorientation and provided inadequate cues to permit a visual approach to the Thebaud Central Facility.
In an attempt to complete their assigned task within self-imposed time constraints, the pilots’ decision-making process was influenced by their past experience and comfort with each other. As a result, the pilots attempted a non-standard visual approach in a degraded visual environment, without thoroughly considering the risks or alternative options.
Canadian Helicopters Offshore’s standard operating procedures provided flight crew with insufficient guidance to ensure that approaches were being conducted in accordance with industry-recommended stabilized approach guidelines.
Depressing and holding the cyclic trim release button, while operating in a degraded visual environment, increased pilot workload and contributed to control difficulties that resulted in an unstable approach that developed into vortex ring state.
The helicopter’s approach became unstable, due to an inadvertent low-energy, high-rate-of-descent flight profile.
The pilots experienced attentional narrowing due to increased workload while attempting a non-standard offshore visual approach in a degraded visual environment. This led to a breakdown in the pilots’ instrument cross-check, which prevented the timely recognition that the approach had become unstable.
The S-92A’s enhanced ground proximity warning system provides no warning of an inadvertent descent at airspeeds below 50 knots indicated airspeed when the landing gear is down. As a result, the enhanced ground proximity warning system did not alert the flight crew of the impending risk of controlled flight into terrain.
The pilot flying was likely subtly incapacitated due to spatial disorientation following the helicopter’s rapid, unexpected descent into the fog layer. As a result, recovery action was initially delayed until the pilots acquired visual contact with the water and the collective was rapidly increased to arrest the descent.
The application of power while in a steep, low-airspeed, high rate of descent condition caused the helicopter to enter vortex ring state. This contributed to the helicopter’s rapid descent into and through the fog layer, bringing the helicopter to within 13 feet of the water.
UPDATE 11 January 2022: WARNING: It has been drawn to our attention that this incident (and indeed our article) is being used to market what is being described as ‘animated software’ [sic] . Aerossurance’s team includes former air accident inspectors, safety, HUMS & FDM managers and two helicopter test pilots. We strongly recommend that any reader in the market for flight data analysis products does a thorough due diligence to ensure the technical accuracy, integrity, usability and functionality of such software and verifies the aeronautical credentials of the product developers. Further: animations alone can be very misleading, especially to the unskilled and those with an expectation bias and consequently lead to misdiagnosis (in one classic case VRS rather than a flying control failure).
Aerossurance is sponsoring and presenting at OGUK‘s 2021 aviation seminar, this year a free webinar spread across 30 June and 1 July.
Aerossurance has extensive air safety, flight operations, helidecks, SAR, airworthiness, human factors, aviation regulation and safety analysis experience. For practical aviation advice you can trust, contact us at: enquiries@aerossurance.com