A Maintenance Error Preceded a Fiery Fatal AS350B3 Accident (CC-ETF, Policia de Investigaciones de Chile)
On 31 January 2024 a police Airbus Helicopters AS350B3 CC-ETF of the Policia de Investigaciones de Chile (PDI) crashed shortly after take off from Pichidangui, Chile. Two of the five occupants died in the post crash fire.

The Directorate General of Civil Aeronautics (DGAC) Chile published their safety investigation report (in Spanish) in March 2026.
The Accident Flight
At 14:00 Local Time the helicopter landed at Pichidangui Aerodrome to refuel. It then departed at 14:40 with 460 litres of fuel, two crew, three passengers and two small plastic drums, containing a total of 35 liters of Jet A1, stowed in the cabin.
The helicopter was engaged in a narcotics eradication mission. The fuel containers in the cabin were to allow a controlled burn of the crop. As a police aircraft, the operation was exempt certain civil aviation regulations, including those related to transport of Dangerous Goods (DG).
Shortly after take off the crew…
…heard strange noises, prompting the decision to land.
There, the aircraft suddenly yawed sharply to the right and descended rapidly, impacting the ground in an area where a perimeter fence…was located.
A post crash fire broke out. The occupants all managed to egress the aircraft but the aircraft commander and one passenger succumbed to their burn injuries.
The DGAC Safety Investigation: The Failure Mode
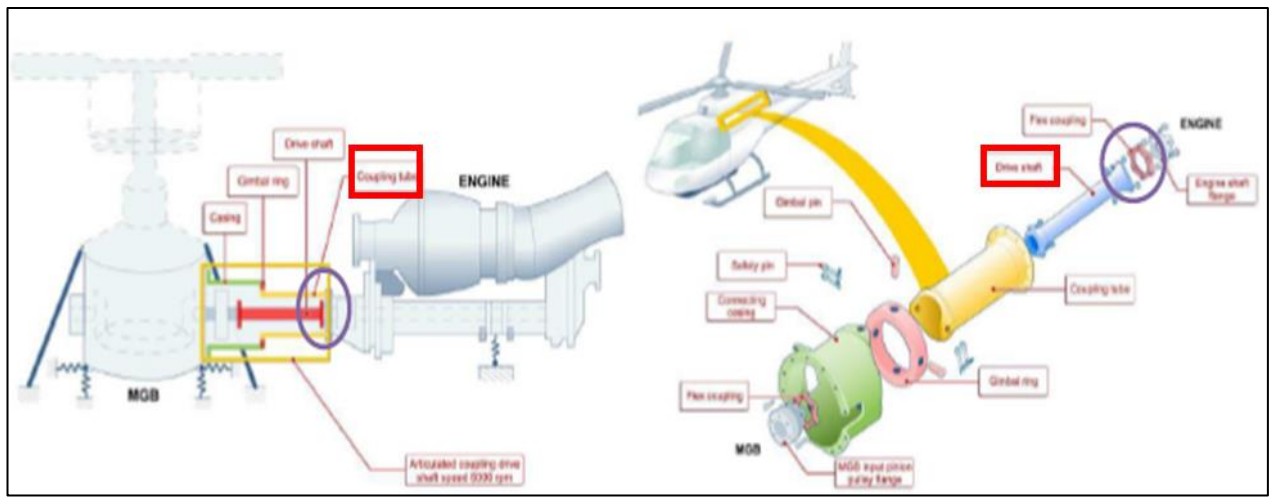
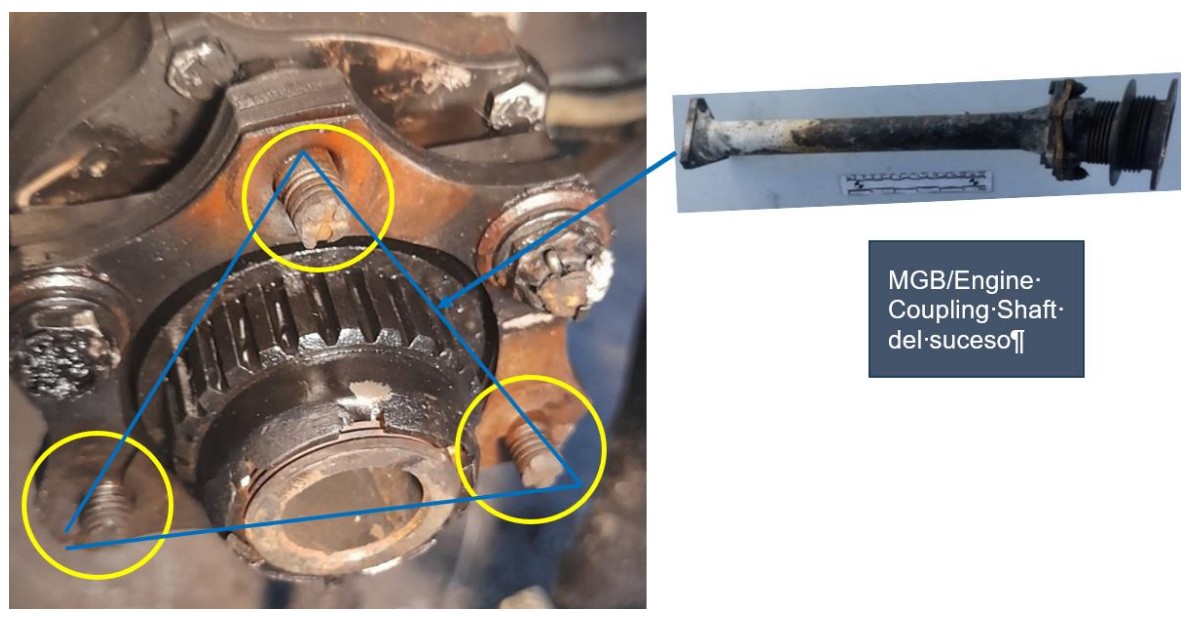
While examining the wreckage at the accident site, investigators discovered that the MGB/Engine Coupling Shaft (highlighted below) had disconnected at the engine end.
The connecting bolts between the Engine Shaft Flange and MGB/Engine Coupling Shaft were found damaged, and their respective nuts, washers and cotter pins, were not found at the scene…
A spectral analysis of an eyewitness video showed…
…a sudden increase in the tail rotor RPM frequency, which reached a maximum of 132% in 0.3 seconds and then decreased. This sudden increase is associated with…a sudden loss of connection between the engine and the MGB. [At] that moment, all the engine’s power was delivered only to the tail rotor, which explains its sudden increase in rpm, and its subsequent decrease indicates normal behavior of the engine control system.
Laboratory examination confirmed…
….that the loss of continuity between the engine and the MGB was a consequence of the disconnection between the flexible coupling on the engine side and the drive shaft.
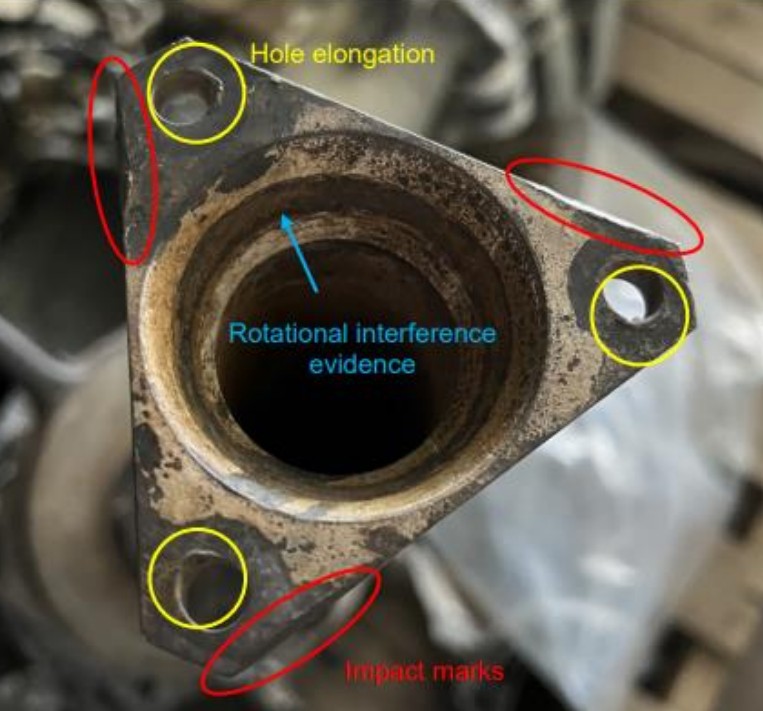
It also noted:
Evidence of elongation of the fixing holes (occurred before disconnection). Impact marks on its sides (occurred after disconnection). Rotational interference with the end of the splined output sleeve of the motor (occurring after disconnection).
…their corresponding washers and cotter pins…were not found at the scene of the incident, so it was not possible to inspect them.
Metallurgical analysis of the remaining nuts did not identify any non-conformities.
It was also noted that the bolts at the other end of the shaft were installed in the opposite direction to that required in the maintenance manual, though that would not have influenced the decoupling of the other end of the shaft.

Investigators concluded that…
…the cause is suspected to be more likely the loss of the bolted coupling between the engine-side baffle and the drive shaft is an incorrect installation of bolts 1, 3 and 5.
A fault tree analysis identified four possible scenarios:
- Missing nuts
- Missing cotter pins
- Insufficient tightening torque of the bolts
- Nuts tightened by hand
Airbus had previously issued Safety Information Notice (SIN) 3695-S-63 on 6 October 2021. This followed a prior maintenance error installing the MGB/Engine Coupling Shaft and provided a pre-print of revised and enhanced work card. It noted that:
The coupling between the engine and the MGB includes two types of flexible couplings: one is crimped (front flexible coupling) while the other one is removable (rear flexible coupling).
To limit the risk of assembly errors and/or FOD, Airbus Helicopters now recommends the disassembly of this coupling on a work bench and not on aircraft.
The new Work Cards…therefore include a new removal/installation procedure that favours the uncoupling of the MGB / engine coupling from the front and then the extraction of the shaft in order to finish the disassembly on a work bench. This new procedure also has the advantage of facilitating the detailed inspection of the flexible couplings.
The DGAC Safety Investigation: Past Maintenance
The helicopter had completed a 12 year inspection May-December 2023 during
which the MGB/Engine Coupling Shaft was disassembled and reinstalled.
The investigators interviewed ‘Mechanic 1’ (who became involved in the check part way through and had 20 years of experience), ‘Mechanic 2’ (who had 12 years experience and was allocated several tasks during the check) and a Maintenance Quality Control Officer. They also spoke to the ‘Maintenance Supervisor’. He indicated:
…the personnel who started the dismantling were not the same as those who continued, because he had to move from this aircraft to another and continued with 2 other mechanics, 2 avionics specialists and 2 aircraft structure specialists and himself, as Maintenance Supervisor and Flight Engineer.
This is partly because the winter is busier with base maintenance and partly because the operator wanted another of their aircraft prioritised. A third aircraft was also undergoing a check at the same time.
In order to achieve the delivery date, overtime was worked during November and December 2023 (77 hours in total in December for example). In practice…
…in the first two weeks of December, they completed the equivalent of three and a half weeks’ worth of work. The pressure to deliver the aircraft before the end of the year was significant and came from management and, of course, from the client.
The investigators observed that…
…the work would have been carried out in an environment with interruptions, operational pressure and extended working hours, conditions that could have influenced the existence of human error during complex technical activities.
After the Chilean accident SIN 3695-S-63 was reissued on 9 February 2024 to reemphasise the recommended precautions.
The DGAC Safety Investigation: The Post Crash Fire
One of the passengers reported that they saw fuel flowing outside the aircraft (not from inside) moments after the impact.
The investigators note that:
The aircraft involved in the incident was equipped with a standard fuel tank and not a
Crash Resistance Fuel System (CRFS), which was optional equipment.
They concluded:
The fire following the aircraft crash is presumed to have been caused by the spilled fuel coming into contact with hot parts of the helicopter, among other possible causes, resulting from damage to the fuel tank when it landed on a wooden post used as part of the airfield’s perimeter fence.
The fuel carried in the cabin likely the contributed to the fire.
The Operator’s Operations Manual did not contain specific provisions regarding the transport of this type of item in the cabin.
DGAC Conclusions
The disconnection of the MGB/Engine Coupling Shaft caused the loss of power from the engine to the gearbox and the main rotor in flight, during the aircraft’s takeoff. This condition caused the aircraft to lose lift and subsequently fall to the ground, impacting a perimeter fence made of wooden posts and subsequently catching fire. The cause of the MGB/Engine Coupling Shaft disconnection was likely due to incorrect assembly during the application of the work cards. The incorrect assembly was possibly due to improper installation of bolts 1, 3, and 5 of the Engine Shaft Flange.
An operational environment (Human Factors) within the maintenance organisation could have increased the risk of staff making mistakes.
DGAC Safety Recommendations
As well as safety recommendations within the DGAC, three recommendations were made to the maintenance organisation:
- Strengthen internal control and verification procedures associated with the
assembly and mounting of critical components, ensuring strict compliance with
work cards and torques specified by the manufacturer. - Establish a cross-inspection or double-checking procedure [i.e. independent inspection procedure] for tasks whose incorrect execution could compromise the integrity of the transmission system.
- To reiterate the following:
- Manage the implementation of Maintenance Resource Management (MRM) [i.e maintenance human factors training] and manage the implementation of a SMS workshop, as a maintenance service provider.
- Promote a culture of operational safety that prioritizes compliance with technical
standards over operational or deadline pressures. - Control of working time and breaks, in terms of setting limits on overtime and
ensuring recovery periods to prevent fatigue. - Ensure that the work group is not modified by incorporating another specialist into
the same task; in short, ensure that the person who starts a job is the same person
who finishes it, ensuring that this job is dedicated exclusively to that person.
Two more were made to the operator to:
- Update your procedures and include in the Operations Manual specific instructions on the transport of fuels, flammable substances or other types of hazardous elements in the cabin, considering not transporting fuel drums inside it, they can be transported in external baskets and/or drums approved for the air transport of fuel, ensuring conditions that minimize the risks in case of impact or fire.
- Study the feasibility of installing Crash Resistant Fuel System (CRFS) type fuel tanks in their aircraft, due to the type of operation they perform.
Safety Resources
The European Safety Promotion Network Rotorcraft (ESPN-R) has a helicopter safety discussion group on LinkedIn. You may also find these Aerossurance articles of interest:
- Crashworthiness and a Fiery Frisco US HEMS Accident
- Grand Canyon Air Tour Tragic Tailwind Landing Accident
- B1900D Emergency Landing: Maintenance Standards & Practices The TSB report posses many questions on the management and oversight of aircraft maintenance, competency and maintenance standards & practices. We look at opportunities for forward thinking MROs to improve their maintenance standards and practices.
- BA B747 Landing Gear Failure Due to Omission of Rig Pin During Maintenance
- What a Difference a Hole Makes: E-8C JSTARS $7.35 million Radar Mishap
- USAF Tool Trouble: “Near Catastrophic” $25mn E-8C FOD Fuel Tank Rupture
- Inadequate Maintenance, An Engine Failure and Mishandling: Crash of a USAF WC-130H
- USAF Engine Shop in “Disarray” with a “Method of the Madness”: F-16CM Engine Fire
- Inadequate Maintenance at a USAF Depot Featured in Fatal USMC KC-130T Accident
- When Down Is Up: 747 Actuator Installation Incident
- Maintenance Human Factors in Finnish F406 Landing Gear Collapse
- Lost in Translation: Misrigged Main Landing Gear
- Cessna Citation Excel Controls Freeze
- B214ST Tail Rotor Drive Shaft Coupling Misassembly
- Crossed Cables: Colgan Air B1900D N240CJ Maintenance Error
- Crazy KC-10 Boom Loss: Informal Maintenance Shift Handovers and Skipped Tasks
- Frozen Dash 8-100 Landing Gear After ‘Improper Maintenance Practices’ Say NTSB
- ATR 72 Rudder Travel Limitation Unit Incident: Latent Potential for Misassembly Meets Commercial Pressure
- Loose B-Nut: Accident During Helicopter Maintenance Check Flight
- USAF RC-135V Rivet Joint Oxygen Fire
- CHC Sikorsky S-92A Seat Slide Surprise(s)
- Attention on Engine Shop Assembly of a S-92A CT7-8 after North Sea IFSD
- SAR AS365N3 Flying Control Disconnect: BFU Investigation
- In-Flight Flying Control Failure: Indonesian Sikorsky S-76C+ PK-FUP
- AAR Bell 214ST Accident in Afghanistan in 2012: NTSB Report
- Misassembled Anti-Torque Pedals Cause EC135 Accident
- EC130B4 Accident: Incorrect TRDS Bearing Installation
- Ungreased Japanese AS332L Tail Rotor Fatally Failed
- R44 Ditched After Loss of TGB & TR: Improper Maintenance
- Missing Cotter Pin Causes Fatal S-61N Accident
- Emergency S-76D Landing Due to Fumes
- Engine & Emergency Flotation Failures – Greenland B206L4 Ditching
- The Missing Igniters: Fatigue & Management of Change Shortcomings
- FAA Rules Applied: So Misrigged Flying Controls Undetected
- BEA Point to Inadequate Maintenance Data and Possible Non-Conforming Fasteners in ATR 42 Door Loss
- BA A319 Double Cowling Loss and Fire – AAIB Report
- BA A319 Double Cowling Loss and Fire – AAIB Safety Recommendation Update
- ANSV Report on EasyJet A320 Fan Cowl Door Loss: Maintenance Human Factors
- Tiger A320 Fan Cowl Door Loss & Human Factors: Singapore TSIB Report
- Human Factors of Dash 8 Panel Loss
- Fuel Tube Installation Trouble
- How One Missing Washer Burnt Out a Boeing 737
- Flying Control FOD: Screwdriver Found in C208 Controls
- Cessna 208 Forced Landing: Engine Failure Due To Re-Assembly Error
- Meeting Your Waterloo: Competence Assessment and Remembering the Lessons of Past Accidents
- Cold Comfort Conference Call: USAF F-35A Alaska Accident
- The Loss of RAF F-35B ZM152: An Organisational Accident A £81 mn fighter is downed by FOD, one of its own intake blanks. This case study illustrates James Reason’s concept of Organisational Accidents and how just asking “who left the intake blank ?” misses the real reasons behind this accident.
You might find these safety / human factors resources of interest:
- James Reason’s 12 Principles of Error Management
- Back to the Future: Error Management
- This 2006 review of the book Resilience Engineering by Hollnagel, Woods and Leveson, presented to the RAeS by Aerossurance’s Andy Evans: Resilience Engineering – A Review and this book review of Dekker’s The Field Guide to Understanding Human Error: The Field Guide to Understanding Human Error – A Review
- Airworthiness Matters: Next Generation Maintenance Human Factors
FSF Maintenance Observation Programme (MOP)
Aerossurance worked with the Flight Safety Foundation (FSF) to create a Maintenance Observation Program (MOP) requirement for their contractible BARSOHO offshore helicopter Safety Performance Requirements to help learning about routine maintenance and then to initiate safety improvements:
MOP was subsequently adopted by IOGP in their Recommended Practices. Aerossurance can provide practice guidance and specialist support to successfully implement a MOP.