Night Offshore Training AS365N3 Accident in India (VT-PWF, 2015)
The Indian Aircraft Accident Investigation Bureau (IAAIB) has issued their report into the fatal loss of Airbus Helicopters AS365N3 VT-PWF, operated by Pawan Hans, while conducting night training in the ONGC Bombay High oil field on 4 November 2015.

The Accident Flight: 319 seconds to Disaster
The helicopter took off with just the two crew aboard from the WIS Offshore Installation at 19:10 local time, heading for the Ron Tappmeyer drilling rig, alongside the EE Offshore Installation, 82 nm East of Mumbai. The pilot flying needed to regain his night currency to be on night medevac stand-by, having last flown offshore at night 11 months earlier on 30 November 2014.
The IAAIB states:
- The pilot on controls was flying during dark phase of moon at night after break of nearly a year.
- 56 secs after takeoff…the autopilot was engaged in ALT and HDG modes. In these modes, the pilot adjust{s] power by the movement of collective stick. The helicopter was in cruise for about 3 minutes. The cruise altitude was between 550ft and 650ft AMSL with Auto-Pilot engaged. About 98 secs prior to the crash, the autopilot (upper modes ALT and HDG) was disengaged.
- The helicopter made a tail wind approach with speed of approximately 79 kts for Ron Tappmeyer which is to the south extremity of the South field with no other rigs nearby to provide ambient lighting which caused an abrupt loss of visual reference.
- …the pilot slightly moved the cyclic stick backward and the collective stick downward. Consequently, the pitch increased and the power decreased. This maneuver looks like a standard approach procedure to decrease the speed. Thereafter, the pilot moved the cyclic stick slightly to the left and began a left turn.
- The left turn was 50 seconds long with slight variations in roll attitude. The lateral acceleration remains between -0.03 and +0.09. The corrections did not lead to a roll attitude less than 12° to left.
- After the Autopilot disconnection, the pilot was “hands on” and the attitude of the helicopter was consistent with the inputs on the flight commands.
- No specific pilot inputs were recorded, except actions on the collective pitch in the last second of the recording.
- The pilot flying has probably entered conditions ideal for black hole phenomenon because of loss of horizon wherein he was not aware about the direction he was proceeding to i.e. up or down / turning right or left. [Note we have discussed this phenomena before: HEMS Black Hole Accident: “Organisational, Regulatory and Oversight Deficiencies” and Deadly Combination of Misloading and a Somatogravic Illusion: Alaskan Otter]
- The instructor cautioned, (though delayed), the pilot flying twice.
- No audio warnings were recorded…except the “Decision Height” warning which triggered 4 seconds before the end of the recording and is consistent with the height of the helicopter at that moment (200 ft).
Both crew died after the helicopter impacted the sea at 116 knots. The flight lasted just 5 minutes 19 seconds. the Emergency Flotation System was not armed.
Operational Issues
The IAAIB observed:
There is no SOP [Standard Operating Procedure] for carrying out night offshore training. There are some references in the SOP issued for Night Ambulance Operation [medevacs].
Medevac is defined in the contract signed between ONGC and PHL, and PHL is providing the helicopter for medevac purposes but, it is not one of the explicit requirements of the contract.
We discuss some of the issues contracting for medevac in our article: The Tender Trap. Also:
There is no document indicating procedure of taking weather (offshore) and transmitting the same to flight crew. The flight crew operating in offshore is not provided with accurate information on the visibility, cloud ceiling and cloud base.
There was also no mechansim to review comments made by instructors in training records.
Crew Resource Management (CRM)
The IAAIB states:
Having decided to go around, the flying pilot needed to get on to instruments and if he was disoriented, should call out so that the non-flying pilot can take over. This aspect is also emphasised in special points in the Medevac SOP.
The CVR readout brings out a lack of adherence to standardized checks and procedures and communication protocol between the crew. While the pilot on controls decided to go around, both pilots, perhaps, continued to fly VFR. Pilot monitoring displayed lack of situational awareness by not taking over controls. The crew thereby failed to engage in the important process of CRM.
There is a shortage of pilots and situation …aggravated due [to a] higher attrition rate of flight crew.
Safety Management Systems (SMS)
The operator’s SMS Manual has not been revised since it was issued the previous year nor had the required annual review been conducted. The IAAIB say the DGCA accepted SMS Manual did…
…not contain “How to do” [instructions dor] the various functions mentioned therein. The Manual just remains a document without performance of any function at working level.
This suggests a manual we would call ‘shelfware‘.
Despite previous accident investigations recommending the formation of a “strong safety department” it was observed that…
…the operator has not established the safety department in true letter and spirit [of the recommendations]. Even actions taken on recommendations have withered away with passage of time due [to] complacency and non supervision. It is still continuing on ad-hoc basis and full fledged department is yet to be established.
Various organisational changes had occurred but no Risk Assessment was found by IAAIB for any of those changes. No safety circulars or bulletins had been issued in the previous 2 years and safety training required by the SMS Manual for all employees had not been completed. The operator’s SMS defined 18 key performance indicators but data was not being collated or shared.
ONGC’s SMS also lacks aviation specifics:
There is no documented safety system or procedure with ONGC to ensure Safety Assurance particularly for helidecks audits, certification and periodic inspections.
Although Pawan Hans had reported helideck problems to OGNC “no closed loop system exists to make these good in a timely effective manner”.
These short comings are disappointing as a 2012 accident involved ONGC tasking a new operator with a new 17D helicopter type to operate to 14D helidecks. A non-fatal tail rotor strike promptly followed.
AAIB’s Analysis
The IAAIB comment:
As discussed earlier, disorientation or black hole approach Illusion can happen during a final approach at dark night over water beyond which the horizon is not visible. These conditions may produce the visual illusion of a high-approach perspective.
The position of Ron Tappmeyer was to the south extremity of the South field with no other rigs nearby to provide ambient lighting. As per the AIS and FDR the tail wind approach was made with speed of approximately 79 kts. This high speed approach would have caused an abrupt loss of visual reference.
The pilot on controls was flying during night after break of nearly a year. The fact that it was a dark phase of moon made this even more challenging. Some amount of dusk flying on instruments would have prepared the pilot flying for undertaking the night flying profile/ maneuvers.
As soon as he got airborne and set course for Ron Tappmeyer, the pilot flying has probably entered conditions ideal for black hole phenomenon because of loss of horizon as is corroborated by CVR replay. Under such conditions he was not aware about the direction he was proceeding to i.e. up or down / turning right or left.
The pilot flying probably continued to fly visually instead of getting on to instruments. Therefore on initiating the go around after realizing that he was high he entered into spatial disorientation extremely quickly.
The instructor was not disoriented and was aware that the helicopter was low. He had cautioned, (though delayed), the pilot flying twice. He however did not realize that the pilot flying was in total state of spatial disorientation and was unable to react to his caution. Nor did he take over controls.
Safety Recommendations
For Offshore Flying
- The Helidecks from where night currency training are to be carried out may be identified by ONGC in association with the Helicopter operators and these helidecks should be provided with minimum landing aids for night offshore operations. DGCA may develop procedures for landing and takeoff utilizing these aids.
- As far as practicable night flying to/from the floating vessels should not be carried out.
- The existing SOP on offshore departure and arrival for Bombay High should be immediately reviewed.
- DGCA may review the requirements regarding flight rules for offshore night operations and corresponding training and recency requirement.
- ONGC should develop system and procedure for carrying out periodic audit of the helidecks from safety point of view. This audit should be linked to continued certification of the helidecks for operational purposes.
- In addition to the automated means of ascertaining the meteorological information, a manual means of verifying and updating the visual elements of observation, i.e. cloud amount and height of base, visibility and present weather, may be developed. The latest weather report from each installation should be made available to the helicopter operator one hour before take-off.
General: Pawan Hans
- Documentation is a weak area…. [A]ll the Manuals, procedures, processes be reviewed and amended to have cohesion of content. System of periodic review should be put in place and strictly followed.
- PHL should immediately undertake the implementation of safety management system across the whole organisation by completion of training, reviewing the manual by including the procedures for the actions to be carried…, appointing key safety personnel…
- Remedial measures should be put in place to reduce pilot attrition.
- Crew should be indoctrinated in CRM, SOPs, good aviation practices, communication and assertiveness.
Our Comments
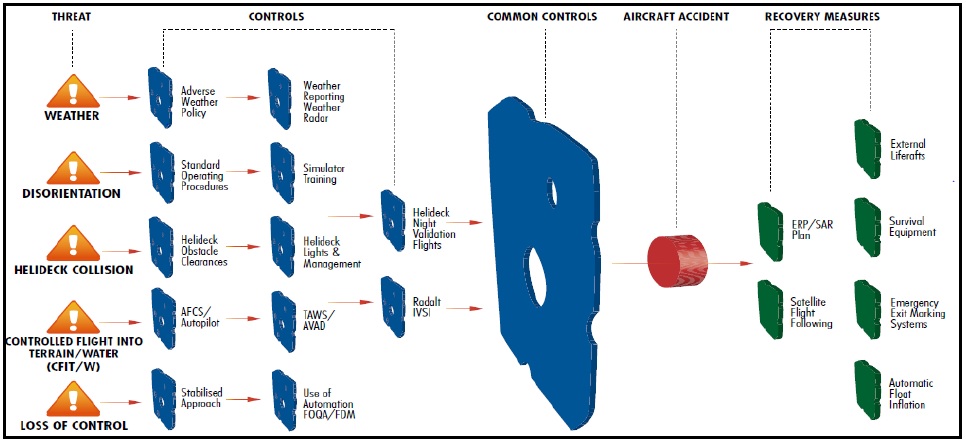
The International Association of Oil & Gas Producers (IOGP) Aviation Management Guidelines contains Guidance on Night Operations (published in August 2013 and written in 2009 and 2010 by a working group lead by Aerossurance’s founder, Andy Evans). The Night Ops Working Group:
…conducted an investigation of all known civil offshore helicopter accidents at night which occurred between 1999 and 2007. Among other things, it was determined that the likelihood of an accident is approximately six times higher at night than during the day. Two of the core accident components were Controlled Flight Into Terrain/Water (CFIT/W) and Loss of Control.
Uniquely for the IOGP AMG, this interim guidance Appendix uses a bow-tie format to clearly and concisely show threats and controls:
The Flight Safety Foundation (FSF) Basic Aviation Risk Standard for Offshore Helicopter Operations (BARSOHO), launched in May 2015, which Aerossurance helped develop, contains a full set of contractible controls for night offshore operations and medevac. This aligns with the HeliOffshore Safety Performance Model.
HeliOffshore have also produced new offshore approach path management guidelines specifically developed to improve the safety of offshore helicopter operations. heliOffshore say:
The document provides significant new insights into five key elements that can make a meaningful difference in ensuring safe stabilised approaches in the offshore environment.
Steve O’Collard (CHC test pilot) and Mark Prior (former Bristow test pilot of M Prior Consulting) oversaw completion of the guidance. Tim Rolfe, of Bristow Group, co-leader of HeliOffshore’s Operational Effectiveness workstream explains the initiative is about:
…providing crews with repeatable operating practices designed to manage flightpath control effectively and maintain awareness of the helicopter’s state [which] offers strong mitigation against any potential loss of control.
Other offshore night accidents to study include:
- AAIB Report 7/2008: AS365N G-BLUN “when preparing to land on the North Morecambe platform, in the dark, the helicopter flew past the platform and struck the surface of the sea”.
- GCAA Final Report: B212 A6-ALV struck drilling rig leg when drifted back on night take off.
-
CIAIAC Report A-002/2010: AW139 EC-KYR, crashed in a controlled flight into water at the end of a SAR exercise.
-
AAIB Report 1/2011, EC225 G-REDU “the flight crew made a visual approach to the platform during which the helicopter descended and impacted the surface of the sea”.
Also see our articles:
Pawan Hans AS365N3, VT-PWA Accident 13 January 2018
UPDATE 13 January 2018: Pawan Hans lose another AS365N3, VT-PWA, with all 7 POB off Mumbai.
UPDATE 30 January 2018: The press report twelve major accidents involving Pawan Hans helicopters took place between 2010 and 2018, during which 55 people lost their lives. The independent directors are being appointed and FDM introduced. See this ASN search: click here.
UPDATE 17 September 2019: Lapses caused 2018 Pawan Hans crash
A pilot disoriented by the altitude [sic: should be attitude], poor communication between him and the co-pilot and a malfunctioning autopilot that hadn’t been set right although a test flight indicated a problem with the system caused the January 12, 2018 Pawan Hans helicopter crash that left seven people dead, a probe by the Aircraft Accident Investigation Board (AAIB) has found.
UPDATE 24 April 2020: Spatial disorientation probable cause of fatal 2018 PHL Dauphin crash
Cockpit voice recording transcript extracts revealed that both crew were fighting for control seconds before the aircraft hit the water. The pilot-in-command (PIC) had experienced spatial disorientation and about 20 seconds before the crash, had disengaged the autopilot. He froze on the controls, and repeated callouts and attempts to take over the controls by the pilot monitoring (PM) proved futile, the report noted. The crash was not survivable.
The 87-page accident report portrays glaring lapses at several levels, including the finding that a persistent malfunction in the autopilot’s “heading” mode went unrectified and likely contributed to the crash. The report notes that “recommendations of earlier investigations having serious operational/safety implications are yet to be implemented by PHL in true spirit.” … the organization “went into denial mode instead of taking these observations in a positive sense,” the board observed.
Helicopters are provided to ONGC through contracts executed with companies such as PHL, Global Vectra Helicorp Ltd, Heligo Charters, etc. Almost all these operators have raised concerns in the past about hourly liquidated damages (LD) clause that imposes heavy penalties for operators not being able to provide helicopters as contracted. The LD clause puts pressure on operators to suppress minor defects and cannibalize spares and rotables from other aircraft. The board grimly noted that “there is preponderance of unsafe situations due to this [LD] clause”.
UPDATE 26 March 2018: We look at another Indian air operator with a “non-existent” SMS: Indian King Air Take Off Accident: Organisational & Training Weaknesses In that case the safety investigators make the point that:
An Organisation may look compliant vis-a-vis the mandatory requirements but may still be seriously deficient in discharging its duties safely and efficiently.
We would add, that they may even be compliant but effectiveness may be weak. The investigators elaborate:
Therefore deeper analysis of the Organizational Structure & Procedures (if existing), and those practised is required to find out the answer to the circumstances leading to the accident.
UPDATE 7 April 2018: Investigators Criticise Cargo Carrier’s Culture & FAA Regulation After Fatal Somatogravic LOC-I. A Shorts 360 N380MQ, operated by SkyWay Enterprises as a Part 135 flight on contract to FedEx crashed in the Caribbean after the crew likely suffered a Somatogravic Illusion raising the flaps on a dark night in 2014. The lack of an FAA SMS regulation for Part 135, the operator’s poor safety culture and implications for the wider industry culture stand out in a thoughtful accident report.
UPDATE 15 July 2018: HF Lessons from an AS365N3+ Gear Up Landing
UPDATE 29 September 2018: HEMS A109S Night Loss of Control Inflight
UPDATE 2 November 2019: Taiwan NASC UH-60M Night Medevac Helicopter Take Off Accident
UPDATE 14 December 2019: Fatal Taiwanese Night SAR Hoist Mission (NASC AS365N3 NA-106)
UPDATE 6 January 2020: Runway Excursion Exposes Safety Management Issues
UPDATE 19 April 2020: SAR Helicopter Loss of Control at Night: ATSB Report
UPDATE 23 August 2020: NTSB Investigation into AW139 Bahamas Night Take Off Accident
UPDATE 26 September 2020: Fatal Fatigue: US Night Air Ambulance Helicopter LOC-I Accident
UPDATE 24 July 2021: Loss of Bell 412 off Brazil Remains Unexplained
UPDATE 19 March 2022: Offshore Night Near Miss: Marine Pilot Transfer Unintended Descent
UPDATE 14 May 2022: Review of “The impact of human factors on pilots’ safety behavior in offshore aviation – Brazil”
UPDATE 5 June 2022: North Sea Helicopter Struck Sea After Loss of Control on Approach During Night Shuttling (S-76A G-BHYB 1983)
UPDATE 28 December 2022: Night Mountain Rescue Hoist Training Fatal CFIT
UPDATE 7 January 2023: Blinded by Light, Spanish Customs AS365 Crashed During Night-time Hot Pursuit
UPDATE 8 July 2023: BK117 Offshore Medevac CFIT & Survivability Issues
UPDATE 16 July 2023: SAR AW139 LOC-I During Positioning Flight
UPDATE 17 February 2024: Night Offshore Take-Off Loss of Control Incident
UPDATE 18 February 2024: Night Offshore Helicopter Approach Water Impact
UPDATE 18 December 2024: Loss of Sikorsky S-76C+ 5N-BQG of Eastwind Off Nigeria 24 October 2024
UPDATE 20 December 2024: 29 Seconds to Impact: A Fatal Night Offshore Approach in the Irish Sea
UPDATE 8 February 2025: S-76D Loss of Control on Approach to an Indian Drilling Rig
Aerossurance is pleased to be supporting the annual Chartered Institute of Ergonomics & Human Factors’ (CIEHF) Human Factors in Aviation Safety Conference for the third year running. We will be presenting for the second year running too. This year the conference takes place 13 to 14 November 2017 at the Hilton London Gatwick Airport, UK with the theme: How do we improve human performance in today’s aviation business?