Safety Lessons from TransAsia ATR-72 Flight GE222 CFIT
1 February 2016
Safety Lessons from TransAsia ATR-72 Flight GE222 CFIT
The Aviation Safety Council (ASC) of Taiwan has issued their investigation report into the loss of TransAsia Airways (TNA) ATR 72-500B-22810 on 23 July 2014 during an attempted landing in poor weather. It highlights a number of important safety lessons.
The Accident
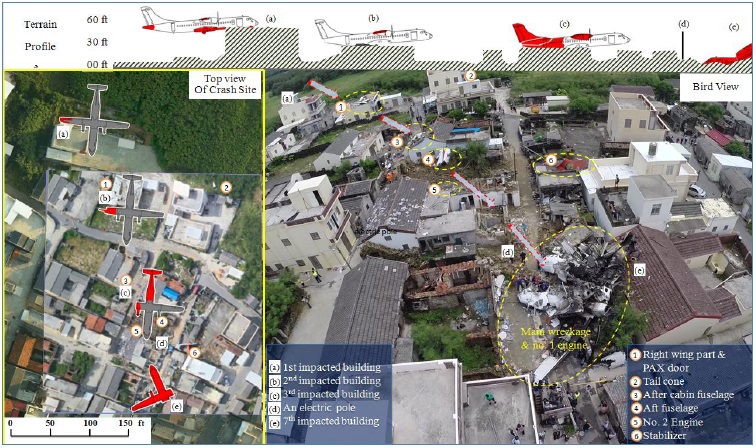
During a non-precision approach, after around 34 minutes of holding, the aircraft impacted terrain in a residential area 800m NE of the threshold of runway 20 at Magong Airport, Penghu Islands, Taiwan during a heavy thunderstorm associated with Typhoon Matmo. Ten of the 58 on board survived.
The Commander was Pilot Flying (age 60, ex-military, joined airline in 1992, ATPL, 22,994 hours total, 19,070 hours on ATR42/72) and the First Officer (FO) was Pilot Monitoring (age 39, direct recruit by the airline in 2011, CPL, 2,393 hours total, 2,084 hours on ATR42/72).
There was no approach briefing before commencing descent and the FO “proposed that he conducted the before landing check by himself without a cross-check”, which the Commander approved.
The ASC say the Controlled Flight Into Terrain (CFIT) occurred because:
The crew continued the approach below the [330ft] minimum descent altitude (MDA) when they were not visual with the runway environment contrary to standard operating procedures.
GE222’s altitude and track deviations (due to the PF’s left control inputs and crosswind) while attempting to visually locate the runway (Credit: ASC)
When the aircraft had descended to 249 feet, the first officer illustrated the position of the [Missed Approach Point] MAPt by saying “we will get to zero point two miles”. At 1905:44, altitude 219 feet, the captain disengaged the autopilot. Four seconds later, the captain announced “maintain two hundred”. The captain maintained the aircraft’s altitude between approximately 168 and 192 feet in the following 10 seconds… The flight crew intentionally operated the aircraft below the MDA…while attempting to visually sight the runway so they could land the aircraft.
Neither flight crew member recognised the need for a missed approach until the aircraft was at just 72ft, 0.5 nm beyond the MAPt, where impact with the terrain was “unavoidable”.
Having discussed the effect of a cockpit gradient, the ASC note that in interviews with other TransAsia crews the consensus was that “the occurrence first officer would accommodate the captains’ flying habits, and tended not to challenge captains’ landing decisions”. We have previously discussed whether it is better for the Commander to be the Pilot Flying or the Pilot Monitoring and this accident re-emphasises that question. However, we do note below that the FO did intervene after several course, mode and communication errors by the Commander.
According to the flight recorders data, non-compliance with standard operating procedures (SOPs) was a repeated practice during the occurrence flight.
The ASC also say the Commander was “likely overconfident in his flying skills”, potential the reason for pressing on below MDA. We do note however a Uni Air ATR72-600 aircraft had successfully landed on Runway 20 just 8 minutes earlier which may have influenced the Commander’s behaviour.
However, it would be no surprise to any aviation safety professional that the ASC report revealed a range of systemic factors.
Systemic Factors – Fatigue
The ASC used QinetiQ’s System for Aircrew Fatigue Evaluation (SAFE) biomathematical fatigue model in their analysis, although they were limited by what data on the flight crew sleep patterns was available . This well-validated model suggested the Commander was “a little tired” and the FO was “not being unduly affected by fatigue”. The ASC however note:
The captain stated he was very tired and his yawning was detected by the CVR. In addition, lapses in radio communications with ATC, incorrect VOR approach course selection, and incorrect automatic flight control system (AFCS) mode selections, all requiring the first officer to intervene. Furthermore, the captain’s real-time roster indicated an elevated flying activity where he routinely completed 6 sector days and had accumulated a total flight time of 278 hours in the last 90 days.
The ASC therefore concluded the Commander’s performance was “probably degraded by his fatigue accumulated from the multiple sectors/day flown and flight and duty times during the months preceding the occurrence”. They note the airline did not have data-driven fatigue risk management system (FRMS), nor was it required to.
Systemic Factors – EGPWS
The aircraft was equipped with a Honeywell Enhanced Ground Proximity Warning System (EGPWS), Mark VIII. The ASC say:
…the occurrence aircraft’s approach profile was outside the EGPWS terrain warning zone, which meant that the crew did not receive a warning of an impending collision with terrain.
During the investigation, the EGPWS manufacturer advised that a software update for newer EGPWS computers would have generated a “Too Low Terrain” warning because of the revised runway field clearance floor and terrain clearance floor envelopes.
The new -022 software was an evolution and is currently not compatible with the current EGPWS fitted on ATR72-500 fleet from a hardware point of view and there is no capability to upgrade…
Systemic Factors – Flight Ops Standards
Observation flights and interviews conducted by the ASC identified “prevalent tolerance for non-compliance with procedures within the airline’s ATR fleet”.
Most interviewees stated that deviations from SOPs mostly occurred when crew made several return trips between the same ports or felt fatigued. The SOP deviations included absence of cross checks, lack of call outs, briefings without using the briefing card, and overlooking some of the procedures, etc.
SOP non-compliances observed by the ASC during simulator training sessions “were not corrected by the instructors” and were evident in occurrence investigations [such as the May 2012 Flight GE515 incident], line observations, simulator observations, internal and external audit reports.
The tolerance for or normalization of SOPs non-compliance behaviors was symptomatic of an ineffective check and training system with inadequate supervision by the airline’s flight operations management.
The Head of the Standards and Training “was an assistant manager without a flying background”. The airline lacked a Standards Pilot for the ATR fleet.
The airline had implemented Crew Resource Management (CRM) training, Threat and Error Management (TEM) training but had not implemented a Line Operations Safety Audit (LOSA) programme. The ASC adding:
…the systemic safety problems at the airline indicated that their TEM training program was not effective otherwise they might have been more cognizant of the risks confronting the crew on the day of the occurrence.
The airline did have a Flight Operations Quality Assurance (FOQA) programme, but:
…settings and analysis capabilities were unable to readily identify those events involving SOP non-compliance during approach…. The FOQA events were not analyzed sufficiently or effectively, leaving some safety issues in flight operations unidentified and uncorrected. …trend analyses were not investigated further.
Non-compliances were “an enduring, systemic problem and formed a poor safety culture within the airline’s ATR fleet”. Non-compliance with SOPs had been identified as a risk by the airline but stated mitigation was simplistically “to remind crews to follow procedures”.
There is a view, as for example expressed by Sidney Dekker, that in practice procedures must be interpreted by front-line personnel and that non-compliances should be viewed in context of the circumstances the crew find themselves. This might be a relevant to some non-compliances observed but is unlikely to be relevant to descending below MDA on the accident flight, for example.
Systemic Factors – Safety Management
Although the CAA has published an Advisory Circular on Safety Management Systems (SMS) it is not yet a requirement in Taiwan. The airline had commenced an SMS implementation but this was: “disorganized”, “non-systematic” and ” incomplete”. This may be explained by the safety office being under-resourced and not involved in the airline’s ‘flight safety action group’ according to the ASC.
The SMS was “dependent on its internal reactive safety and irregularity reporting” and so did not “develop full awareness of the airline’s safety risks”. It did not take advantage external safety information sources (something we advocate strongly). The flight operations safety risk register was last updated in March 2011. Further the ASC say:
There was no evidence that the TNA had conducted any specific CFIT risk assessments, documented the findings, implemented appropriate CFIT risk controls, and confirmed the ongoing effectiveness of those risk CFIT controls.
Based on the information about the adequacy of TNA’s corporate culture, flight standards, hazard awareness and training, previous occurrences, line observations, and interviews, the [post-accident ASC] evaluation indicated that the CFIT risk for TNA operating an ATR72 on a non-precision approach into Magong in those weather conditions with crew not complying with SOPs was a ‘significant threat’.
In June 2014 flying was around 15% higher on the ATR fleet than the previous year, with the fleet increased from 9 to 10 aircraft, with the number of pilots reducing slightly from 54 to 52. The airline however had assessed that 60 pilots were required for a fleet of 10 ATR aircraft. The ASC therefore concluded that risk assessment of change was inadequate:
…the company did not assess or mitigate the safety risks associated with the increase in ATR operational tempo as a result of the recent increase in ATR fleet size and crew shortage that, in turn, elevated crew flying activities and the potential safety risks associated with crew fatigue.
The ASC say:
…the inadequate risk management processes and assessments, ineffective safety meetings, unreliable and invalid safety risk indices, questionable senior management commitment to safety, inadequate safety promotion activities, underdeveloped flight operations quality assurance (FOQA) system, and inadequate safety and security office and flight operations resources and capabilities constituted an ineffective safety management system (SMS).
Systemic Factors – Other
The ASC go on to comment on the inadequacies of the CAA’s oversight, their lack of a mechanism to assess the relative risk of approved operators to help target attention, inadequacies with the weather data supplied and coordination on a joint military/civil airfield. We will not examine these in this summary.
Approach and landing accident reduction (ALAR) has long been among the primary goals of the Flight Safety Foundation (FSF). A major update of the FSF ALAR Tool Kit, featuring the findings of analyses of recent accident data and the findings of the FSF Runway Safety Initiative, was issued in 2010.
GE235
The ASC are going through the final approval process for their report on the take-off accident in Taipei to TransAsia ATR 72-600 B-22816, Flight GE235, on 4 February 2015 in which 43 people died. Preliminary reports indicate that about 36 seconds after takeoff the No 2 engine auto-feathered and about 46 seconds later the No 1 engine no.1 was shut down. That accident was the airline’s 5th hull loss since 1995.
TransAsia Flight GE235 Accident 4 Feb 2015 (Credit: Unknown)
TransAsia Airways arranged to disclose confidential information to the “Next Magazine”, with the intention to stir up public opinion and press through media reports in an attempt to influence the accident investigation conclusion, the ASC claims. This constituted a breach of Article 21 of the Air Traffic Accident Investigation Law, leading to a fine of $3 million New Taiwan dollars (about US $94400). ASC states that Next Magazine published contents of the draft final report on May 11, 2016 that it claims were obtained from TransAsia Airways. The airline had received a copy of the confidential draft report as it was a party in the investigation.
On the day the fine was announced, the airline’s Air Operator Certificate (AOC) was revoked by the Taiwanese authorities. TransAsia had previously announced that it was shutting down. The airline continuously lost money, with shares sliding since two fatal accidents in 2014 and 2015.
Aerossurance has extensive air safety management, safety culture development, assurance and accident analysis experience. For aviation advice you can trust, contact us at: enquiries@aerossurance.com