Fatal $16 Million Maintenance Errors (Sundance Helicopters AS350B2 N37SH)
A jury in Las Vegas awarded $16 million to the families of 4 passengers killed in a December 2011 helicopter sightseeing accident, caused by a series of maintenance errors. The National Transportation Safety Board (NTSB) made safety recommendations on maintenance human factors and fatigue after this accident.
The Accident
Airbus Helicopters AS350B2 N37SH, operated by Sundance Helicopters, suffered a Loss of Control (LOC) accident in mountainous terrain east of Las Vegas on 7 December 2011. The helicopter, en route to overfly the Hoover Dam, was destroyed by the impact forces and post-crash fire. The pilot and four passengers were killed.

The day before the accident a team of three mechanics and one inspector had completed a 100 hour inspection on the aircraft, along with replacement of the engine, the tail rotor servo and the main rotor fore/aft servo. In their report the NTSB state:
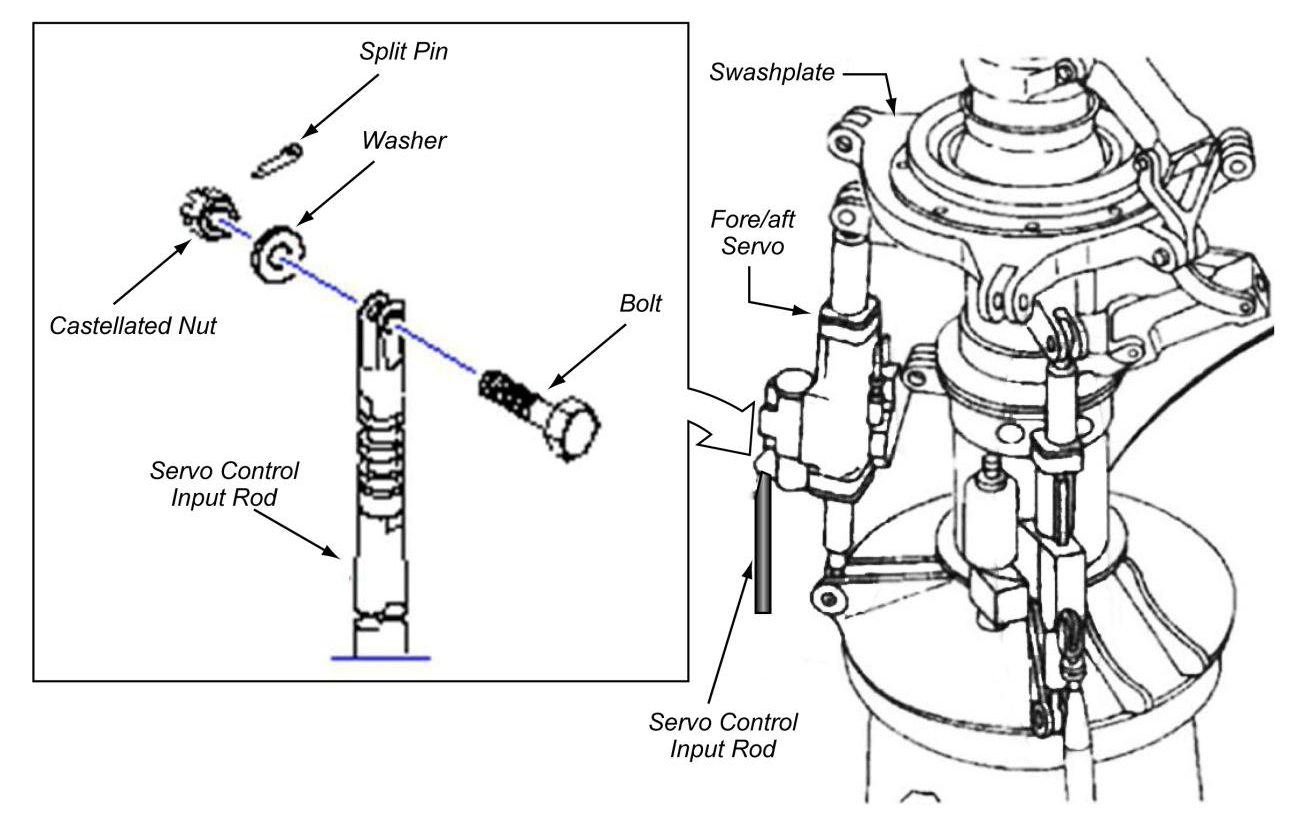
During examination of the wreckage, the main rotor fore/aft servo, one of the three hydraulic servos that provide inputs to the main rotor, was found with its flight control input rod not connected. The bolt, washer, self-locking nut, and split pin (sometimes referred to as a “cotter pin” or “cotter key”) that normally secure the input rod to the main rotor fore/aft servo were not found. The investigation revealed that the hardware was improperly secured during maintenance that had been conducted the day before the accident.
Probable Cause
The NTSB determines that the probable cause of this accident was Sundance Helicopters’ inadequate maintenance of the helicopter, including:
(1) the improper reuse of a degraded self-locking nut,
(2) the improper or lack of installation of a split pin, and
(3) inadequate post-maintenance inspections, which resulted in the in-flight separation of the servo control input rod from the fore/aft servo and rendered the helicopter uncontrollable.
Contributing to the improper or lack of installation of the split pin was the mechanic’s fatigue and the lack of clearly delineated maintenance task steps to follow.
Contributing to the inadequate post-maintenance inspection was the inspector’s fatigue and the lack of clearly delineated inspection steps to follow.
Maintenance Safety Issues
The NSTB specifically highlighted four maintenance safety issues.
Issue 1: Improper reuse of degraded self-locking nuts
Certification requirements FAR 27.607 and CS-27.607 state that “Each removable bolt, screw, nut, pin, or other fastener whose loss could jeopardize the safe operation of the rotorcraft must incorporate two separate locking devices”. This requirement is designed to give redundancy. In this case the first locking feature is provided by using a self-locking nut and the second by use of the split pin. The NTSB found during their interviews and inspection of a sample of the operator’s aircraft that during maintenance nuts were being routinely re-used that did not meet the published criteria for re-use. That meant the nuts were no longer self-locking and one line of defence was eliminated.
Issue 2: Maintenance personnel fatigue / alertness
The NTSB concluded that both the mechanic and the inspector, who worked on the helicopter the day before the accident, were likely fatigued, with a consequential reduction in alertness. This was in part, because they had insufficient time to adjust to returning to work earlier than normal. Both were on a 4 days-on, 3 days-off shift pattern, from 12:00 to 23:00. They were due to be off 4-6 December, but were both called on the afternoon of 5 December and asked to work on 6 December, starting prior to 06:00. The mechanic managed just 5 hours sleep that night, the inspector 7 hours. Furthermore, the inspection was completed near the end of a 13 hour 24 minute shift. The NTSB believe this disrupted shift pattern contributed to 1) the improper securing of the fore/aft servo connection hardware, 2) the improper installation of a hydraulic belt (detected by a pilot on the first pre-flight after the check and corrected by the dayshift), and 3) the inadequate inspection. The NTSB state: “If the work shifts of the maintenance personnel had been consistent, a major source of their fatigue could have been mitigated”.
Issue 3: Need for work cards with delineated steps
The manufacturer’s Maintenance Manual task card for fore/aft servo replacement had delineated sequential steps to follow. This included several steps installing what Sundance procedures referred to as a ‘safety device’ (for example, a split pin or a safety wire), which in their maintenance procedures required a specific inspection. However, Sundance’s 100 hour inspection paperwork had only one place for the inspector to sign off the fore/aft servo installation, with no intermediate steps. NTSB state “Using work cards that clearly delineate the steps to be performed and critical areas to be inspected to support both the maintenance and inspection tasks is one way to mitigate inadvertent errors of omission in the performance and verification of maintenance tasks, especially tasks involving critical flight controls.”
Issue 4: Lack of human factors training for maintenance personnel
The NTSB comment that the Federal Aviation Administration (FAA) has developed substantial guidance for the industry about maintenance human factors (the FAA issued Advisory Circular 120-72 on Maintenance Resource Management Training in 2000). However, the NTSB note that unlike other in some other countries, there are no FAA regulatory requirements for training in maintenance human factors. In Europe such a requirement was introduced in January 2003, along with other HF related changes, in what was then JAR-145 Amendment 5. In March 2004, as a result of a 2003 fatal accident involving a Beech 1900D at Charlotte, North Carolina, (discussed here) NTSB issued Safety Recommendation A-04-16, to the FAA to require “…Part 121 air carriers implement comprehensive human factors programs to reduce the likelihood of human error in aviation maintenance”. This remains open. In May 2012, the FAA did issue a notice of proposed rulemaking (NPRM), which included a short, proposed requirement for Part 145 repair stations provide human factors training (145.1163(b)(2)). A final rule has not yet been issued. Whereas in Europe Part 145 covers thirds party or in-house, line, base and component maintenance, this FAA proposal would not apply to maintenance conducted inside air operators (including Part 121 operators as in the B1900 case or Part 135 operators as in the AS350 case). The NTSB believe that “This investigation has shown that providing human factors training, including training on the causes of fatigue, its effects on performance, and actions individuals can take to prevent the development of fatigue, to all maintenance personnel would help reduce the likelihood of human error in aviation maintenance.”
NTSB Recommendations
The NTSB made the following recommendations to the FAA following this accident:
Establish duty-time regulations for maintenance personnel working under 14 Code of Federal Regulations Parts 121, 135, 145, and 91 Subpart K that take into consideration factors such as start time, workload, shift changes, circadian rhythms, adequate rest time, and other factors shown by recent research, scientific evidence, and current industry experience to affect maintenance crew alertness. (A-13-01) (Supersedes Safety Recommendation A-97-71 and is classified “Open-Unacceptable Response”)
Encourage operators and manufacturers to develop and implement best practices for conducting maintenance under 14 Code of Federal Regulations Parts 135 and 91 Subpart K, including, but not limited to, the use of work cards for maintenance tasks, especially those involving safety-critical functions, that promote the recording and verification of delineated steps in the task that, if improperly completed, could lead to a loss of control. (A-13-02)
Require that personnel performing maintenance or inspections under 14 Code of Federal Regulations Parts 121, 135, 145, and 91 Subpart K receive initial and recurrent training on human factors affecting maintenance that includes a review of the causes of human error, including fatigue, its effects on performance, and actions individuals can take to prevent the development of fatigue. (A-13-03)
External Oversight and Audits
FAA oversight of the operator’s maintenance organisation appears weak with the NTSB stating:
In the 3 years before the accident, the FAA’s principal maintenance inspector had changed four times and the principal avionics inspector had changed three times. The Las Vegas FSDO [Flight Standards District Office] manager reported that no principal maintenance inspector was assigned from April to September 2011 due to a shortage in office staffing but that surveillance was completed by other office inspectors. A review of the maintenance surveillance records showed that three administrative items, one fuel facility inspection, and one follow-up on a company incident were completed from April to September 2011.
Interestingly that incident is likely to be one that involved one of the personnel in the accident:
A review of Sundance Helicopters records revealed that in June 2011, the QC inspector (acting as a mechanic) failed to properly re-install the chin bubble on one of Sundance’s helicopters. A formal root cause analysis of the event conducted by Sundance stated that the inspector’s perception of the need to expedite the repair to avoid aircraft downtime was a contributing factor leading to this failure and that in his attempt to expedite the repair process, he failed to reference the appropriate aircraft maintenance documents that detailed the task of installing the chin bubble.
The chin bubble fell from the aircraft when commencing a hover taxy. The NTSB provide no further detail on that root cause analysis or the actions taken, but do confirm that a retrospective review of the inspectors other recent work was acceptable and state that the team doing the 100 hour inspection before the accident where under no time pressure. Coincidentally Aerossurance reported on another similar case recently where the FAA fined another helicopter operator $110k after a similar incident in 2012. Sundance Helicopters is a member of the voluntary Tour Operators Program of Safety (TOPS). TOPS members undergo annual independent safety audits against the TOPS Standard, funded by membership of the scheme. However, NTSB identified that the mechanic involved in the servo installation and two other mechanics did not meet the a TOPS Standard requirement that maintenance personnel should have 3 years of experience maintaining helicopters or have undergone helicopter manufacturer training before being employed. The NTSB concluded, perhaps rather generously, that this was due to a ‘misinterpretation’ on the standard, as the company’s Director of Maintenance stated to the NTSB that:
…the company’s understanding of the TOPS requirements was that the operator must meet the experience and factory training requirements “collectively,” rather than its staff members having to individually meet the requirements.
The Company
Bob Engelbrecht, CEO of Sundance Helicopters, who joined the company in August 2012, released the following statement:
All of us at Sundance are saddened for the families of the victims of this truly tragic accident. Today’s jury decision marks the end of a difficult time for everyone involved. We want to thank the jurors for their service and for sacrificing time away from home and work. We also want to assure all in our community that everyone at Sundance Helicopters is committed to achieving and upholding the highest safety standards.
In December 2012, Helicopter Emergency Medical Service (HEMS) operator Air Methods announced an agreement to purchase Sundance for $44 million (and 11 months later they purchased another helicopter tour operator, Blue Hawaiian). By 2018, Sundance Helicopters’ entire fleet of 24 sightseeing helicopters will be made up of Airbus Helicopters EC130T2s, transitioning from a fleet of from AS350B2s and EC130B4s.
Summary
It goes without saying that maintenance errors, especially in helicopters, can have catastrophic results. The reuse of self-locking nuts with less than the minimum torque value appears to have been a practice that had become a routine procedural violation at this operator, eliminating a critical safety barrier. This resulted in latent defects, awaiting an error to trigger a catastrophe. The NTSB believe that error was the misassembly of the servo. They concluded that fatigue was one performance influencing factor and the inadequate work sheets the other.
Safety Observations
It is positive that NTSB have issued a recommendation on regulations to manage maintenance fatigue. The European Aviation Safety Agency (EASA) had already proposed maintenance fatigue management in a wider Notice of Proposed Amendment (NPA 2013-01) of Safety Management Systems (SMS) in maintenance / continuing airworthiness (discussed at this seminar in 2012). Disappointingly the recommendation that addresses the work sheets is simply for the FAA to ‘encourage’ best practice (staged works sheets), that many would regard as fundamental for complex and critical assemblies. NTSB identified the lack of human factors training and the slow pace of rulemaking (compared to say Europe) as another safety issue. Of course some US companies have voluntarily introduced maintenance human factors training (as early as 1989) and those with EASA approvals have had to comply with the European regulations since 2003. Following the B1900 accident, in 2004 NTSB proposed the implementation of a more ambitious “comprehensive human factors programs to reduce the likelihood of human error in aviation maintenance”. It is disappointing that a ‘comprehensive’ approach has been watered down to focus simply on training. This is not to say that training isn’t vitally important. However, unless there is a systemic application of human factors principles in all company policies and procedures, accompanied by a management commitment to investing in eliminating adverse performance influencing and creating a positive safety culture, the benefit will be dramatically reduced. As always the greatest safety benefit comes to those who enthusiastically adopt early and continuously improve.
There is a useful 2002 UK CAA research paper: CAA Paper 2002/06: Work Hours of Aircraft Maintenance Personnel prepared by Simon Folkard DSc., Body Rhythms and Shiftwork Centre,
Department of Psychology, University of Wales (aka ‘The Folkard Report’),
UPDATE 23 March 2016: on issue 2 (fatigue), the Federal Aviation Administration (FAA) has now launched a consultation on AC120-MFRM Maintainer Fatigue Risk Management:
This advisory circular (AC) describes the basic concepts of human fatigue and how it relates to safety for aviation maintenance organizations and individual maintainers; provides information on Fatigue Risk Management (FRM) in terms of fatigue hazards and mitigation strategies specific to aviation maintainers; describes the benefits of implementing FRM methods within aviation maintenance organizations; and identifies methods for integrating FRM within a Safety Management System (SMS) (if applicable). Personnel fatigue was first identified as a critical issue in aviation maintenance by the National Transportation Safety Board (NTSB) in 1996, stemming from the ValuJet accident in Florida. Since then, it continued to gain attention as a maintenance safety risk:
1) In 2000, an FAA field study that collected 50,000 hours of ActiGraph data from maintenance personnel across multiple organizations found that maintainers were typically getting about 5 hours of sleep;
2) In 2006, an FAA survey of international human factors (HF) programs in maintenance organizations revealed that over 80 percent of those responding indicated that human fatigue was an issue;
3 In 2008, an FAA conference on human fatigue revealed that scientists, regulators, company management, and labor representatives all agreed that human fatigue poses a safety hazard in the aviation maintenance industry and that individuals, and government and civilian organizations, need to take appropriate action; and
4) In 2010, the FAA Administrator publicly committed to review all aspects of FAA regulations that address human fatigue
Comments are due 31 May 2016.
Another past case of a misassembled helicopter control linkage can be found here. You may also be interested in:
- James Reason’s 12 Principles of Error Management
- How To Develop Your Organisation’s Safety Culture
- UPDATE 23 September 2015: Critical Maintenance Tasks: EASA Part-M & -145 Change
- UPDATE 23 February 2018: NTSB Reveal Lax Maintenance Standards in Honolulu Helicopter Accident
UPDATE 2 March 2018: An excellent initiative to create more Human Centred Design (HCD) by use of a Human Hazard Analysis (HHA) is described in Designing out human error
HeliOffshore, the global safety-focused organisation for the offshore helicopter industry, is exploring a fresh approach to reducing safety risk from aircraft maintenance. Recent trials with Airbus Helicopters and HeliOne show that this new direction has promise. The approach is based on an analysis of the aircraft design to identify where ‘error proofing’ features or other mitigations are most needed to support the maintenance engineer during critical maintenance tasks.
UPDATE 19 May 2018: If you had spent 2 years rebuilding a classic Piper PA-12 you’d make the time to check the rigging of the flying controls before first flight, right? Sadly, the pilot in this fatal case study was in a rush: Too Rushed to Check: Misrigged Flying Controls
UPDATE 24 June 2018: B1900D Emergency Landing: Maintenance Standards & Practices The TSB report posses many questions on the management and oversight of aircraft maintenance, competency and maintenance standards & practices. We look at opportunities for forward thinking MROs to improve their maintenance standards and practices.
UPDATE 25 August 2018: Crossed Cables: Colgan Air B1900D N240CJ Maintenance Error On 26 August 2003 a B1900D crashed on take off after errors during flying control maintenance. We look at the maintenance human factor safety lessons from this and another B1900 accident that year.
UPDATE 9 February 2019: Meeting Your Waterloo: Competence Assessment and Remembering the Lessons of Past Accidents: No one was injured in this low speed derailment in London after signal maintenance errors but investigators expressed concern that the lessons about maintenance errors from the fatal triple collision at Clapham in 1988 may have been forgotten.
UPDATE 19 April 2019: FAA Rules Applied: So Misrigged Flying Controls Undetected in an accident to a Cessna 172 in Bermuda.
UPDATE 5 September 2020: SAR AS365N3 Flying Control Disconnect: BFU Investigation
UPDATE 13 September 2020: Hawaiian Air Tour EC130T2 Hard Landing after Power Loss (Part 1)
UPDATE 18 October 2020: Hawaiian Air Tour EC130T2 Hard Landing after Power Loss (Part 2 – Survivability)
UPDATE 17 January 2021: Grand Canyon Air Tour Tragic Tailwind Landing Accident
UPDATE 8 January 2022: Fiery Fatal AW119 Accident in Russia After Loss of Tail Rotor Control
UPDATE 9 July 2022: R44 Ditched After Loss of TGB & TR: Improper Maintenance
UPDATE 29 July 2023: Missing Cotter Pin Causes Fatal S-61N Accident
UPDATE 25 May 2025: CHC Sikorsky S-92A Seat Slide Surprise(s)
UPDATE 18 April 2026: A Maintenance Error Preceded a Fiery Fatal AS350B3 Accident
Aerossurance has also worked with the Flight Safety Foundation (FSF) to create a Maintenance Observation Program (MOP) requirement for their contractible BARSOHO offshore helicopter Safety Performance Requirements to help learning about routine maintenance and then to initiate safety improvements: 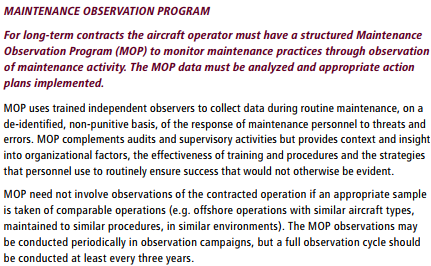 Aerossurance can provide practice guidance and specialist support to successfully implement a MOP.
Aerossurance can provide practice guidance and specialist support to successfully implement a MOP.
Aerossurance’s Andy Evans was recently interviewed about safety investigations, the perils of WYLFIWYF (What-You-Look-For-Is-What-You-Find) and some other ‘stuff’ by with Sam Lee of Integra Aerospace:
Aerossurance was pleased to sponsor this Royal Aeronautical Society (RAeS) Human Factors Group: Engineering conference on 12 May 2015 at Cranfield University: Human Factors in Engineering – the Next Generation
Aerossurance is pleased to be both sponsoring and presenting at a Royal Aeronautical Society (RAeS) Human Factors Group: Engineering seminar Maintenance Error: Are we learning? to be held on 9 May 2019 at Cranfield University.