Wayward Window: Fatal Loss of a Fire-Fighting Helicopter in NZ
28 July 2018
Wayward Window: Fatal Loss of a Fire-Fighting Helicopter in New Zealand
On 13 February 2017 a fire-fighting helicopter was lost in a fatal accident in New Zealand. In their accident report investigators describe how the sudden loss of a window, as a consequence of flying in an unapproved configuration, may have made the pilot pitch up to slow down, allowing the empty under-slung fire-fighting bucket to strike the tail rotor.
History of the Flight
On the afternoon of 13 February 2017, wildfires broke out in New Zealand between Lyttelton Harbour and Christchurch in the Port Hills. A major firefighting effort began the following day. It involved large ground parties, 12 helicopters and two fixed wing aircraft.
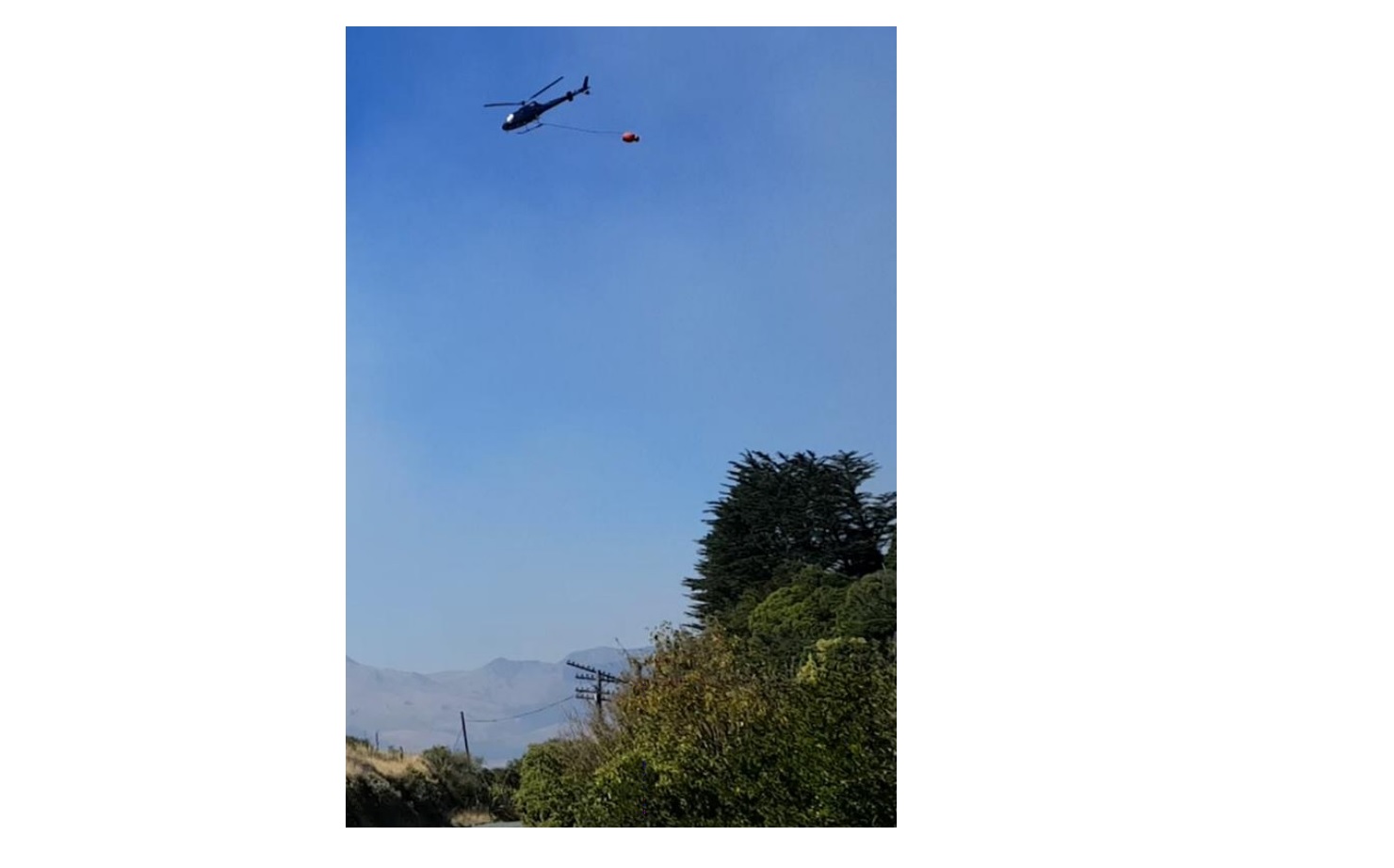
Way To Go Heliservices’ Airbus Helicopters AS350BA ZK-HKW (Credit: TAIC)
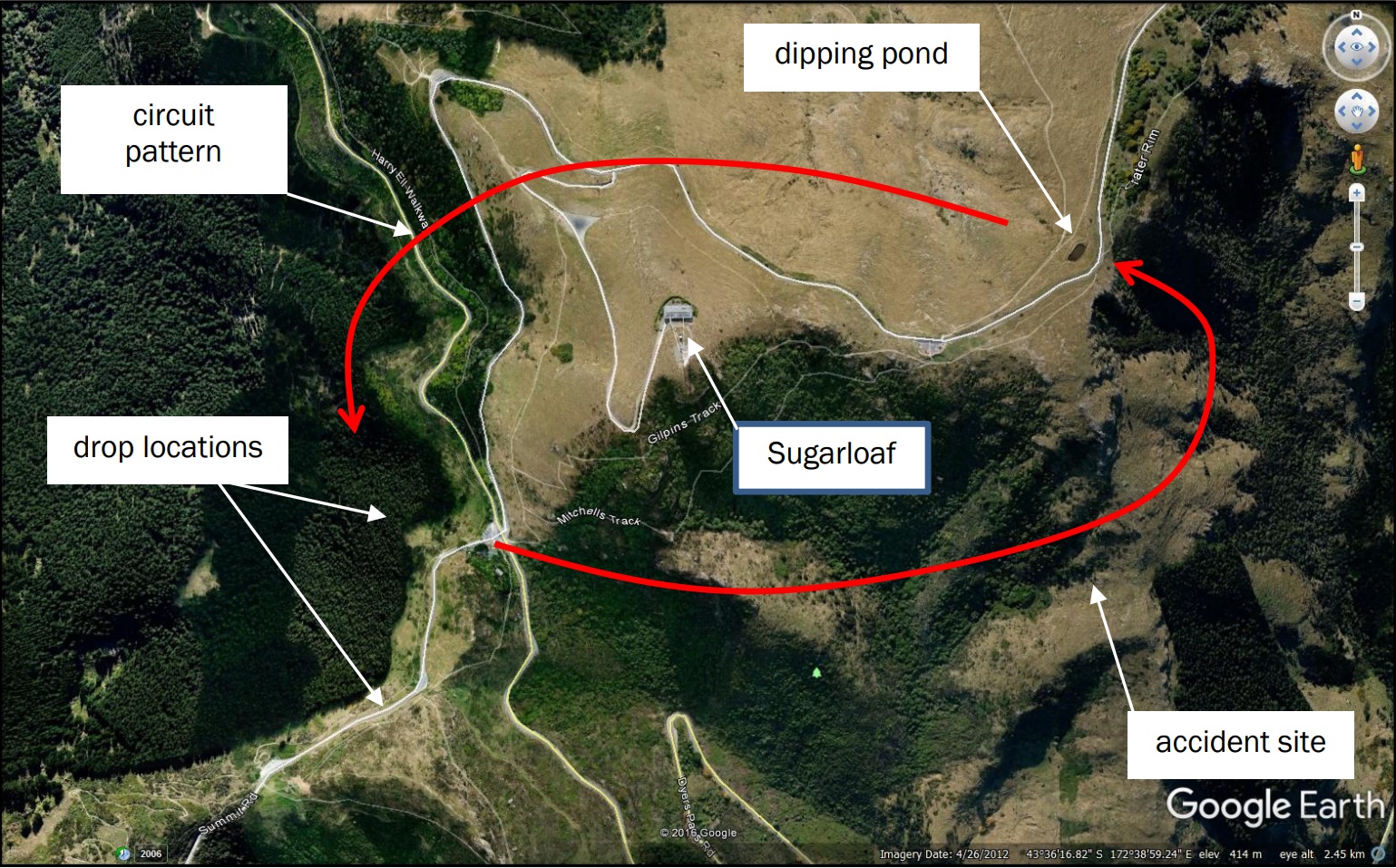
Operating Area of Way To Go Heliservices’ Airbus Helicopters AS350BA ZK-HKW (Credit: TAIC)
It was equipped with a 1000 litre under-slung ‘Cloudburst 1000’ ‘monsoon bucket’ (an alternative to well known ‘bambi bucket‘). This was slung approximately 10m below the helicopter.
Monsoon Bucket Filmed Under Airbus Helicopters AS350BA ZK-HKW (Credit: TAIC)
In the early afternoon ZK-HKW crashed while returning to refill its 1000 litre under-slung ‘Cloudburst 1000’ ‘monsoon bucket’ (an alternative to a ‘bambi bucket’).
The pilot died in the crash.
Safety Investigation
The New Zealand Transport Accident Investigation Commission (TAIC) say in their accident report that:
The tips of the glass-fibre tail rotor blades were missing.
Tail Rotor Blade (TRB) Damage on Way To Go Heliservices’ Airbus Helicopters AS350BA ZK-HKW (Credit: TAIC)
The end of the tail boom, complete with the upper and lower vertical stabilisers, had separated from the helicopter. It was found in vegetation approximately 300m before the main wreckage. All [other] major components of the helicopter were accounted for, except for the window panel from the left rear sliding door. The rubber window seal was retained in the door panel.
TAIC comment that:
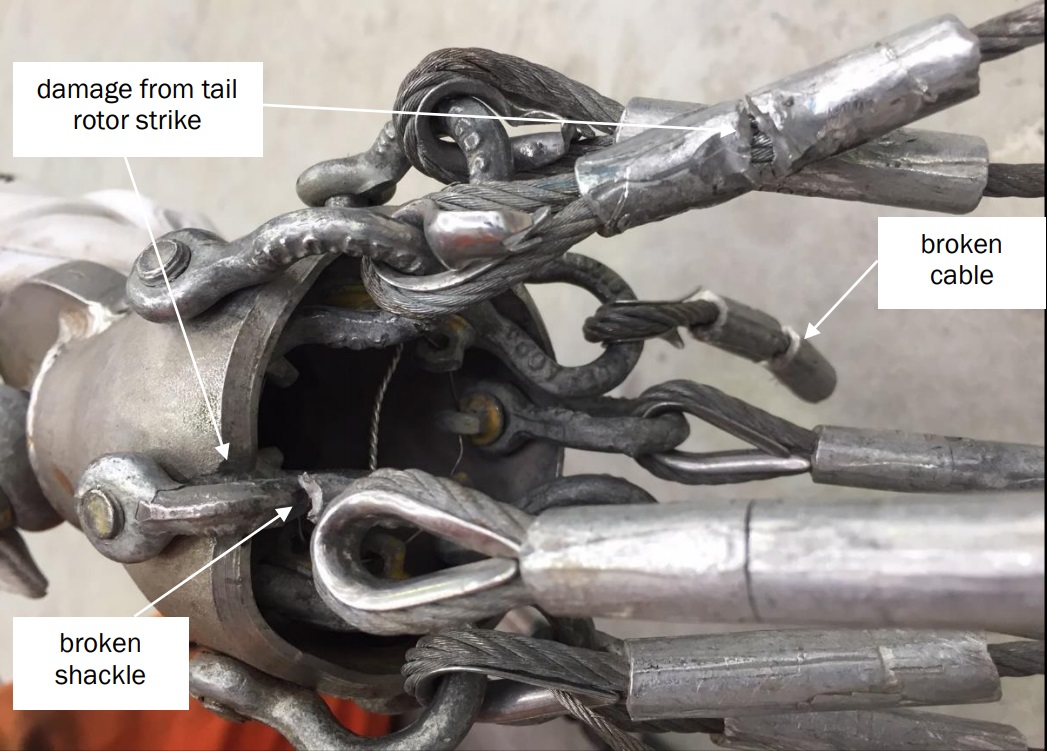
The damage to the tail rotor blades was consistent with their having struck the wire suspension cables of the monsoon bucket where the cables were joined to the lifting strop. There was corresponding damage on the cable cluster. The bucket and the strop remained attached to the helicopter’s fixed hook.
Monsoon Bucket Cable Damage on Way To Go Heliservices’ Airbus Helicopters AS350BA ZK-HKW (Credit: TAIC)
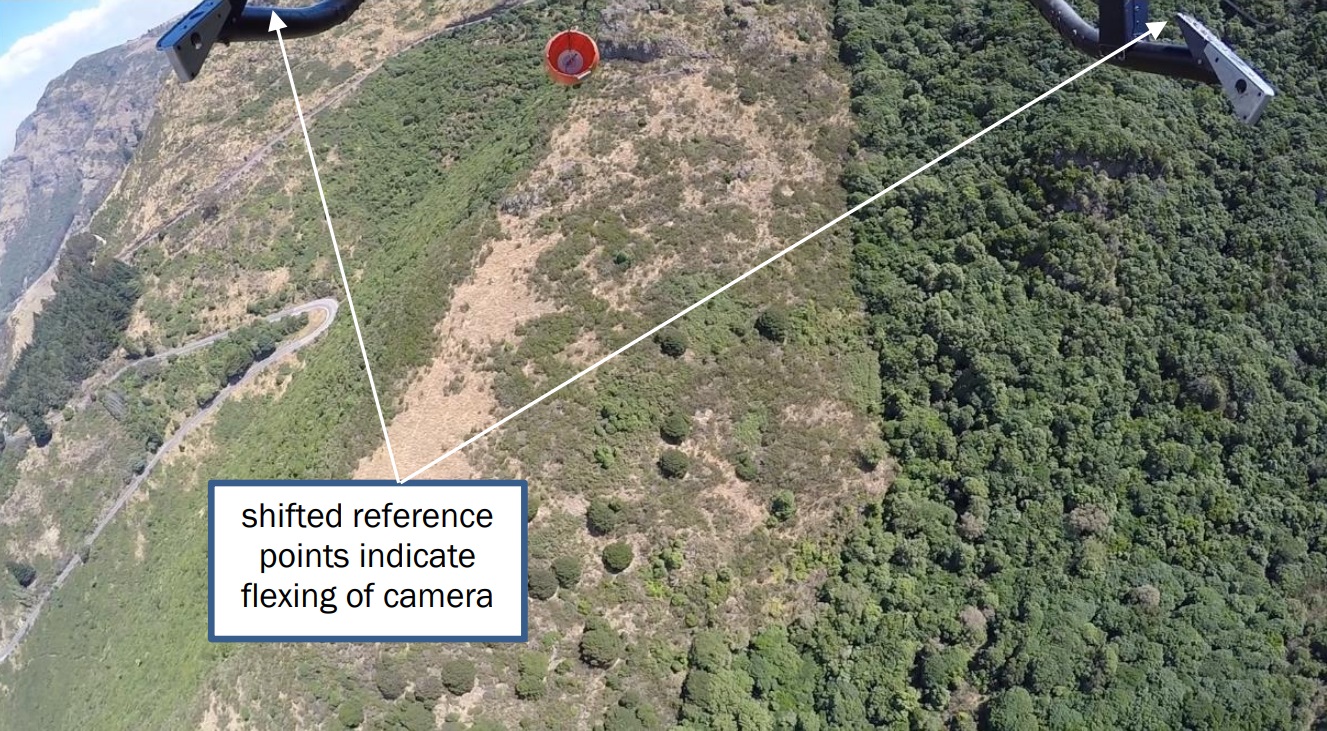
A video recording taken from a camera mounted underneath the helicopter showed the monsoon bucket rising towards the tail rotor.
Monsoon Bucket Filmed Moving Upwards Under Airbus Helicopters AS350BA ZK-HKW (Credit: TAIC)
The video recording also showed that an object fell from the helicopter shortly beforehand. A close examination of the images…determined that the object appeared to be light weight, of rectangular form, and highly reflective.
Falling Object Believed to Be a Rear Window of Airbus Helicopters AS350BA ZK-HKW (Credit: TAIC)
It is virtually certain that this was the window that had dislodged from the left rear sliding door.
The helicopter was fitted with sliding doors on the left side of the cabin and standard doors on the right side. Pilots flew the helicopter from the right seat.
To further improve the pilot’s view of the underslung bucket while firefighting, all the doors on the right side had been removed and the doors on the left side were closed.
The door configuration meant that the window was likely subjected to fluctuating pressure as the helicopter encountered turbulence and wind shear while flying at the estimated 80-90 knots. It is very likely that the window panel was dislodged from the door by a sudden increase in air loading due to turbulence or a change in airspeed.
The damage to the tail rotor caused the vertical stabiliser to tear off the tail boom (see below), and the helicopter became uncontrollable and crashed.
Vertical Stabiliser Falling Away From Way To Go Heliservices’ Airbus Helicopters AS350BA ZK-HKW (Credit: TAIC)
The pilot had experienced a similar loss of the left rear window while flying the same helicopter on a firefighting mission in 2015.
The pilot had assisted in the fighting of [a] fire over a number of days, flying a monsoon bucket with the same helicopter. During that task the window panel from the left rear sliding door had fallen from the helicopter. The Department of Conservation rural fire officer in charge of the firefighting effort recalled that he had noted the missing window by chance, and that the pilot had told him that it had happened because he had been flying too fast. The rural fire officer had recorded the event on an incident reporting card, but no further investigation had been undertaken. At the briefing for all personnel the next day, the rural fire officer had referred to the loss of the window as “flying too fast” and reiterated to the pilots that their flying had to be ‘SEEL’ (safe, effective, efficient and bound by logistical limitations).
The operator’s chief pilot/chief executive had been aware of this incident, but it had not been recorded in the internal quality assurance system and no internal investigation had been conducted. The operator had not notified the incident to the CAA…
TAIC found that this door configuration was unproven and so prohibited in the Rotorcraft Flight Manual:
A supplement to the AS350BA flight manual stated that this particular door configuration was prohibited for the helicopter.
The operator said that it considered that the supplement was ambiguous and was not aware that the configuration was prohibited.
TAIC Investigation Conclusions
The investigators concluded that:
It was very likely that the monsoon bucket flew up towards the tail rotor due to a combination of forward air speed and turbulence. At the same instant, the pilot’s slowing of the helicopter in response to losing the window resulted in the tail rotor dipping and making contact with the rising suspension line for the monsoon bucket.
Although not directly contributory, TAIC found “three deficiencies that indicated the helicopter operator’s quality assurance system should be reviewed”. These resulted in a safety recommendation discussed below.
Investigators also noted the pilot had recently used cannabis. They concluded that it was very unlikely the pilot was impaired by this, but reiterated that the use of performance-impairing substances is a serious risk to aviation safety.
Safety Issues Identified
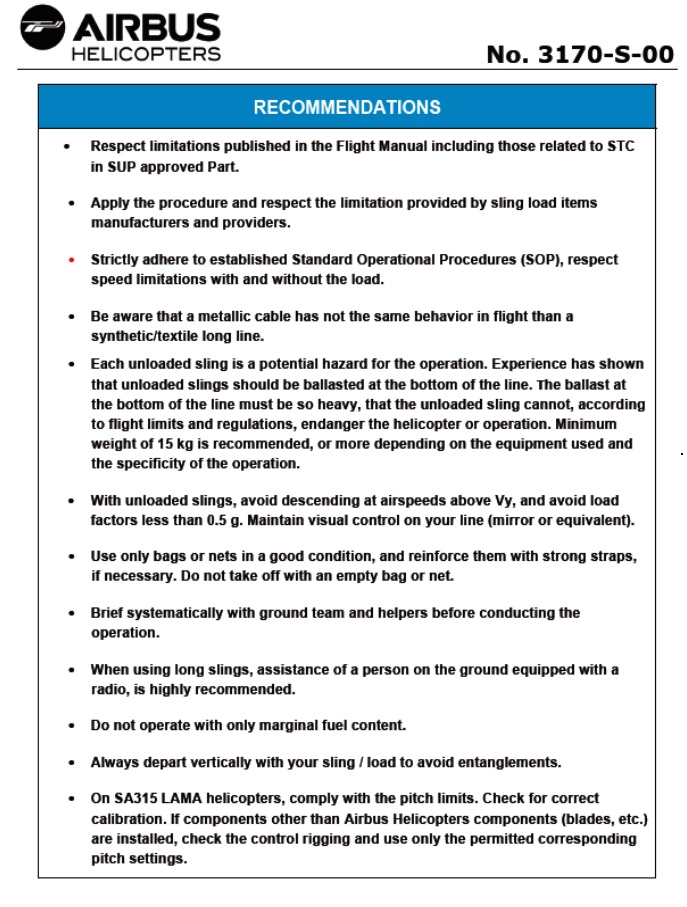
Airbus Helicopters had taken the initiative to issue 5-page Service Letter (No. 1727-25-05) in 2006 to highlight lessons from their analysis of accidents were external loads had contacted tail rotors. After this accident they issued an updated 7-page Safety Information Notice (SIN No. 3170-S-00), reproduced in Appendix 1 of the TAIC report. This included recommendations reproduced below:
Safety Recommendations Safety Information Notice No. 3170-S-00 (Credit: Airbus Helicopters )
TAIC however determined that:
There may not be a good awareness within the helicopter industry of the additional risks involved with underslung load operations, particularly with the use of monsoon buckets during firefighting operations
Additionally, as the bucket could hold 1 tonne of water but the cargo hook was rated for only 750kg, and there had been insufficient follow-up to the previous window loss, TAIC note that:
The operator did not have adequate systems available for the pilot to determine the actual all-up weight and balance of the helicopter for the firefighting operation, or to ensure that incidents such as the previous loss of a window were recorded, notified to the CAA and investigated.
They also comment that as the RFM onboard did not contain information on the Cloudburst bucket the pilots did not have access to important information.
TAIC Safety Recommendations
TAIC had previously made recommendations on substance impairment and industry awareness of underslung load risk.
TAIC made a new recommendation on 23 May 2018 to the chief executive of Way To Go Heliservices to ensure that:
There are robust systems in place for establishing the actual weight and balance of all company aircraft for all operations
Incidents and accidents are recorded, notified to the CAA and investigated, and corrective actions are taken as appropriate
Pilots are fully aware of and observe the operating limitations of all the aircraft types and variants that they fly.
TAIC Key Lessons
The Commission identified the following key lessons as a result of its inquiry into this accident:
Flight in turbulent conditions requires care in order for the pilot to avoid exceeding an aircraft or equipment speed limitation
It is important that operators and pilots understand the reasons for and observe the specific limitations applicable to each aircraft that they operate, as variations often exist between different variants of the same aircraft type
All operational incidents should be recorded and investigated by the operator so that the causes can be identified and corrective or preventive actions taken
Performance-impairing substances such as recreational drugs pose a serious risk to aviation safety. Their short- and long-term effects may be unpredictable and result in pilots being impaired when flying their aircraft.
There is evidence that a pair of over-trousers that had been packed in the cabin came out of the helicopter and became entangled in the tail rotor. Paint marks on the over-trousers matched the colour and profile of the tail rotor blades, and marks on a tail rotor blade match a zip and dome connector on the over-trousers.
…evidence also revealed three incidents in the month prior to the accident in which doors on this helicopter opened in flight. Effective safety management depends on such incidents being reported and investigated, but none of these occurrences was recorded in the operator’s incident reporting system.
UPDATE 16 December 2019: A preliminary report issued by the NZ Helicopter Association and NZ CAA on an accident to firefighting helicopter AS350BA ZK-HEX on 17 Feb 2019 said there was a sudden yaw to the left followed by one to the right and a pitch up. The pilot immediately jettisoned the monsoon bucket, and made a forced landing. Their investigation found the most likely scenario was that the top ring through which the monsoon bucket was attached to the helicopter, partially collapsed. It is reported that:
This investigation has highlighted a possible risk factor when operating the older style Cloudburst CB1000MF bucket with a collapsible top ring that is secured by Velcro. Partial collapse of the ring or if the ring comes away from the Velcro could cause an empty bucket to ‘fly’ erratically in flight and move dangerously close to the tail.
Wreckage of AS350BA ZK-HEK (Credit: TAIC)
UPDATE 17 September 2020: TAIC issue their report on ZK-HEK.
Aerossurance has extensive air safety, operations, airworthiness, human factors, aviation regulation and safety analysis experience. In 2018 and 2019 Aerossurance is supporting one government agency in contracting a number of firefighting aircraft. For practical aviation advice you can trust, contact us at: enquiries@aerossurance.com