NZ Firefighting AS350 Accident: Role Equipment Design Issues
15 January 2021
NZ Firefighting AS350 Accident: Weaknesses in Role Equipment Design and Distribution of Key Operating Data (Airbus AS350BA / FX2 ZK-HEX of Reid Helicopters Nelson)
Wreckage of Airbus Helicopters AS350BA / FX2 ZK-HEX of Reid Helicopters Nelson (Credit: NZ TAIC)
The Accident Flight
The New Zealand Transport Accident Investigation Commission (TAIC) explain in their safety investigation report that fires had been burning throughout the region over the preceding two weeks. ZK-HEX was one of several helicopters assisting using an external fire-fighting bucket, that TAIC refer to as a monsoon bucket.
The [66 year old] pilot had been flying helicopters with monsoon buckets in fire-fighting operations since the mid-1970s [having 14,980 flying hours in total, c4,000 on type].
After dropping a load of water on the target area, the helicopter was returning to a nearby pond to refill the monsoon bucket.
The pilot stated that while dipping the bucket normally into the dipping pond immediately before the accident the bucket “looked soft” and did not fill correctly. A second attempt was made to lower the bucket into the water, after which, the pilot observed, a weight of 800 kg displayed on the load cell. This confirmed to the pilot that the bucket was filled sufficiently. The pilot recalled the shape of the bucket looking normal and then continuing with the flight as intended.
The pilot reported that after reaching cruise airspeed, the helicopter unexpectedly yawed violently one way and then the other. The pilot then heard a loud bang and the helicopter commenced an un-commanded turn to the left.
The pilot initiated a descent for a forced landing, jettisoned the bucket and transmitted a Mayday radio call. The pilot descended towards an area of light bush close to a forest access road, but the helicopter started to spin near the ground.
The pilot recalled following the recommended procedure for a loss of tail rotor control by closing the throttle, shutting the engine down to stop the helicopter spinning, and conducting an autorotative landing.
A number of fire service personnel…arrived at the accident site within a few minutes and were able to assist the pilot out of the wreckage. The pilot received a minor ankle injury.
The TAIC Safety Investigation
TAIC does not appear to have any recorded flight data to examine. Examining the wreckage revealed:
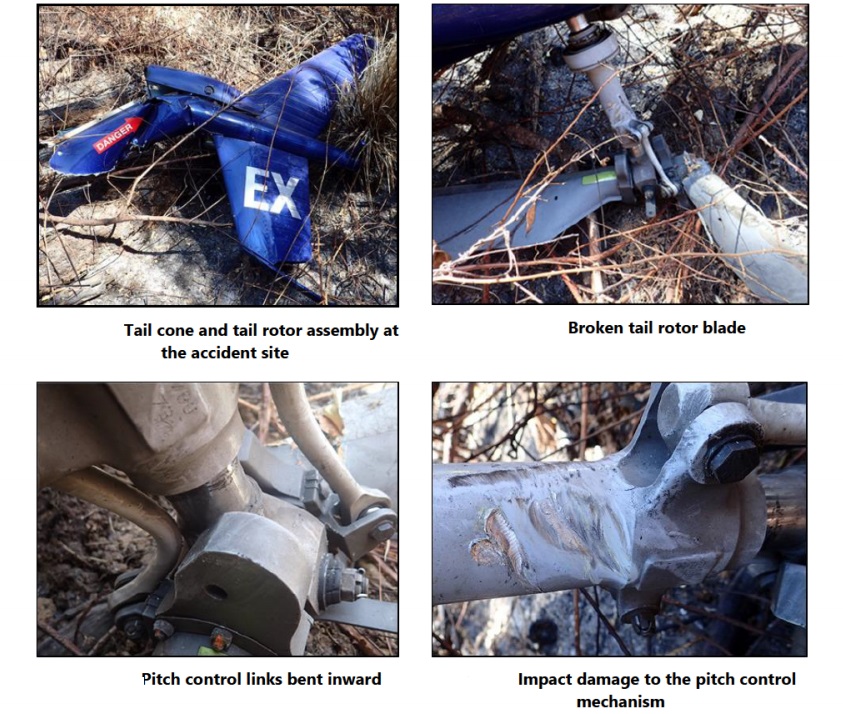
One tail rotor blade was broken at its root end but remained attached by its internal structure. The opposing tail rotor blade exhibited no external damage. The tail rotor drive shaft had failed at its forward coupling.
The two pitch control links on the tail rotor assembly were found deformedand the tail rotor pitch-control slider had numerous indentations. Yellow synthetic [PVC] material was found on the tail rotor assembly at various locations. The same yellow material was also found on the leading edge of the broken tail rotor blade.
The jettisoned bucket was found in a collapsed state in a forested area approximately 100 m to the south… A yellow synthetic sheathing was used to enclose the synthetic lifting line, electrical cable and pneumatic line. All of these exhibited damage at about the same point along the length of line.
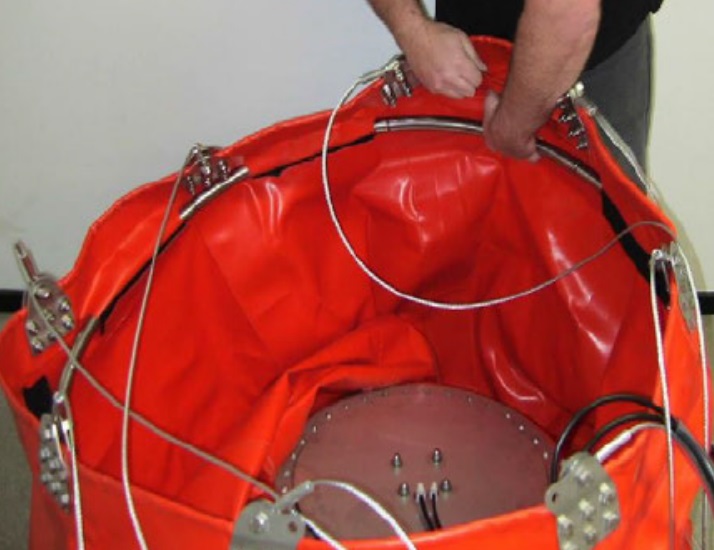
A tubular, segmented, stainless-steel ring normally held in place by hook-and-loop [commonly referred to as Velcro] fastener tabs at the top of the bucket had come apart and was displaced.
Hook and Loop Fastners in IMS Cloudburst CB1000MF Firefighting Bucket (Credit: NZ TAIC)
Stiffening Ring of IMS Cloudburst CB1000MF Firefighting Bucket (Credit: NZ TAIC)
TAIC explain that:
The monsoon bucket was an earlier version of the Cloudburst CB1000MF, manufactured in New Zealand by IMS New Zealand Limited (IMS). It had a maximum capacity of 1,000 litres. The bucket was constructed using a flexible urethane fabric.
The synthetic lifting line was 8.5 m in length and attached to the helicopter cargo hook at its upper end and to the bucket control head (containing an arrangement of electrical and pneumatic controls associated with the functioning of the bucket) at its lower end. The bucket was suspended below the bucket control head by eight, 3 m-long steel cables.
When assembling the bucket for deployment, the eight hook-and-loop fastener tabs could be opened to accept the tubular, segmented, stainless-steel ring in the upper section of the bucket, then closed to secure it. This allowed disassembly for transport and storage. The ring had the effect of keeping the top section of the bucket rigid when empty.
A small bladder was attached to the inside wall of the bucket that] could be filled with a [fire-retardant] additive. Throughout the operation on the day of the accident, the bladder was filled during every helicopter refuelling cycle. The operator’s ground crew member who had carried out this task stated..that the bucket was in good condition during the last refuelling [sic].
The investigators determined that…
…the monsoon rope assembly had been caught in the tail rotor assembly [and] the rotor/driveshaft stopped abruptly as a result. With the tail rotor disabled, the pilot was not able to maintain directional control of the helicopter and had to descend into the forested area below to conduct a forced landing.
It was likely that during the accident flight, one or more of the hook-and-loop fastener tabs came undone, allowing the ring to become insecure and the bucket to lose rigidity. This likely resulted in a sudden change to the aerodynamic stability of the bucket in the airflow, leading to the bucket trailing behind the helicopter and the lifting line contacting the tail rotor.
However, they were…
…unable to determine whether the displaced hook-and-loop fasteners were due to incorrect installation, worn material and flight loads, abnormal forces during firefighting activities such as striking a submerged object during dipping, or a combination of these.
TAIC note that:
No requirement exists within the [New Zealand] Civil Aviation Rules for manufacturers of this type of role equipment to be certificated or to produce operational information to assist with the safe operation of their products.
The onus was on operators to identify risks associated with the use of any role equipment and mitigate those risks appropriately. The [NZ] CAA’s involvement with such equipment was limited to assessing, and if satisfied approving, an operator’s exposition , in which maintenance and operating procedures for the use of such role equipment were defined.
Since the Cloudburst monsoon bucket’s initial design, a number of improvements have been incorporated [and the use of] hook and-loop fastener tabs to retain the…stainless-steel ring was superseded. The new design was….a rigid composite material, in two sections, …permanently bolted into the bucket.
The change was to allow the bucket to be “more rapidly deployed on site” and not out of a safety issue. However, TAIC’s investigation identified several previous cases where hook-and-loop fasteners had come undone during flight.
IMS…had produced 128 buckets with the earlier tubular, segmented, stainless-steel ring. Of these, 33 had been sold in New Zealand. As this equipment had not been controlled or tracked after the initial sale, the status of these earlier buckets could not be determined.
IMS had developed recommended limitations regarding airspeed, line length, and empty bucket flight configuration for the Cloudburst monsoon bucket and had also published an ’Operation Manual‘. This manual provided descriptions of the bucket’s components, but contained no information relating to the aforementioned limitations.
As…there was no requirement for a manufacturer to promulgate any operational information or limitations, and IMS had not done so. By comparison, the Commission found that a Canadian manufacturer of a similar product…had produced detailed operational and service manuals that were accessible to operators.
The customer, Fire and Emergency New Zealand (FENZ) did not at the time of the accident have a requirement for lifting line length in their standard, simply stating “strop length shall be optimised with the type of bucket to counter rotor wash on the fire”. At the time of the accident the operator’s procedures did not specify what an appropriate line length was.
In contrast, in the US the National Wildfire Coordinating Group (NWCG) Standards for Helicopter Operations required lifting lines to be 50 feet (15.2 m) or longer, emphasised also in Airbus Helicopters issued Safety Information Notice No. 3349-S-25 – ‘Follow-up of recommendations and limitations associated with the use of bucket-type fire-fighting systems’.
Safety Issues and Safety Recommendations
TAIC concluded there were two safety issues:
The manufacturer of the Cloudburst monsoon bucket had not promulgated key operational information on and limitations of the Cloudburst monsoon bucket to operators.
There was insufficient guidance to pilots on the appropriate line length for monsoon bucket operations.
TAIC issued two safety recommendation on 25 June 2020 to IMS New Zealand Limited:
The operator has since incorporated the Airbus guidance into its operating procedures and FENZ has included a similar requirement in its updated supplement for wildfire operations.
On 6 April 2020 IMS issued on its website a Service Information Letter detailing a preflight checklist for the Cloudburst bucket with the tubular, segmented, stainless-steel ring and the Velcro retention tabs.
The Service Information Letter followed an email sent to a mailing list from IMS on 7 February 2020, which included a Cloudburst Fire Bucket Safety Notice. This notice explained that IMS had discovered worn Velcro retention tabs during maintenance and therefore wished to highlight the importance of equipment checks and maintenance to operators of the buckets.
[NZ CAA] issued Continuing Airworthiness Notice 05-012 on 16 April 2020. The Continuing Airworthiness Notice outlined that the CAA strongly recommended that operators and maintainers follow the instructions in the Cloudburst Fire Bucket Service Information Letter…
NZ CAA [is] in the process of developing an advisory circular to Civil Aviation Rules Part 133 – Helicopter External Load Operations. In November 2019 the CAA, in conjunction with a commercial supplier of lifting equipment, carried out a number of educational workshops for helicopter operators on how to inspect and safely use lifting equipment. Both of these programmes were in development prior to this accident, and were initiated due to an industry-wide recent increase in helicopter external-load incidents.
Aerossurance has extensive air safety, aerial fire-fighting, operations, airworthiness, human factors, aviation regulation and safety analysis experience. For practical aviation advice you can trust, contact us at: enquiries@aerossurance.com