USAF F-16C Crash: Engine Maintenance Error
Improper assembly of the Main Engine Control unit caused a USAF Lockheed Martin F-16C Block 30H 87-0306 to be destroyed in a crash SW of Joint Base Andrews, Maryland, on 5 April 2017, according to the USAF Accident Investigation Board. The pilot ejected safely 10s before impact.

The F-16C was from the Air National Guard 113th Wing, 121st Fighter Squadron at Joint Base Andrews and was one of four departing on a basic surface attack training mission.

During take off the aircraft experienced an uncommanded GE F110-GE-100C engine acceleration, followed by a loss of thrust and engine fire and so the pilot jettisoned the external fuel tanks (one landed between two houses and the other landed in a wood, fortuitously neither hitting anything) and then shut the engine down.

A severe engine overspeed and engine over-temperature had occurred, followed by the engine fire and, ultimately, a catastrophic engine failure.
The AIB found…
…the cause of this mishap was the incorrect assembly of the main engine control (MEC) differential pressure pilot valve, which was missing a required 600-degree retaining ring and the anti-rotation pin.
The misassembled differential pressure pilot valve caused the MEC to malfunction and to incorrectly meter abnormally high fuel flow to the engine.
A substantially contributing factor to the mishap was the 552d Commodities Maintenance Squadron, MEC Overhaul Shop, Oklahoma City, Air Logistics Complex, lack of an adequate procedural requirement for MEC parts accountability.
The loss to the US Government was valued at $22 million.
Maintenance History and MEC Investigation
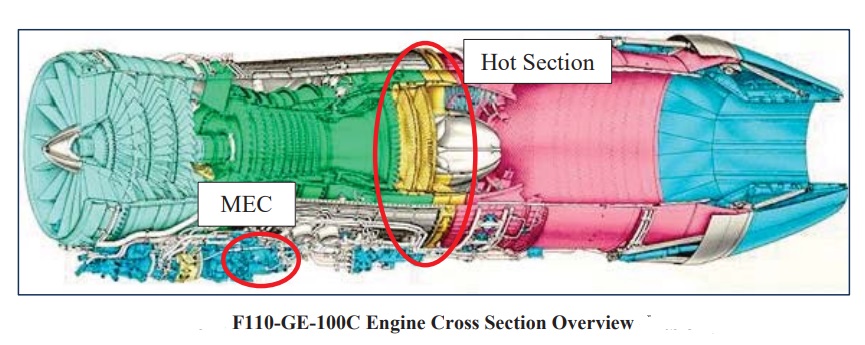
The MEC is designed to regulate fuel flow and the variable stator vane position of the engine. The MEC senses the engine core speed and adjusts fuel flow as necessary to maintain the desired engine speed in accordance with pilot input via the throttle.
The MEC overhaul process consists of complete disassembly, solvent wash, and inspection. After inspection and any ncessary component replacement, the MEC is reassembled and tested.
After overhaul, the MEC of 87-0306 underwent test on 31 January 2017 but failed to meet acceptance criteria. It was re-inspected and found to have a fuel cam spline misaligned. That error was corrected and it was retested on 16 February 2017. It again failed test, being rejected with comments “check FDT [fan discharge temperature] spring and VSV [variable stator vane]; VSV not repeating”.
The MEC was again returned to the overhaul shop. The FDT spring was found serviceable, the governor servo valve was changed due to a broken tang, and O-ring foreign object debris (FOD) was found in the VSV. The MEC passed a third test on 8 March 2017.
The MEC was fitted to the engine of 87-0306 the day before the accident on 4 April 2017 in unscheduled maintenance.
When stripped at Woodward Governor after the accident the MEC was found to contain FOD (a piece of backing ring) that potential prevented sealing of the unit, an incorrect Vitron seal (rather than the specified fluorosilicone seal) and the absence of both the 600-degree retaining ring and anti-rotation pin.

Pin – note small size (Credit: USAF)
The investigation found that the personnel involved were appropriately trained and there were no “major” documentation errors. However, USAF Technical Order (TO) 6J3-4-131-3 requires “parts accountability and emphasizes the critical importance of such procedures” but “does not specify a methodology for parts accountability”. The investigators found:
During on-site observation of the MEC overhaul shop, it was observed that gaps exist in terms of parts accountability. WCDs [Work Control Documents] provide an auditable account of the work accomplished IAW the TOs; WCD numbers 110M1R and 110M5R do not require a technician stamp to document that all parts are accounted for during MEC overhaul and assembly.
Furthermore, there is no process to determine if all required parts have been installed after overhaul and assembly completion. It was observed that some parts remained in part trays from previous assembly kits, with no way to determine if all required parts were installed.
The technician who overhauled the MA MEC, other MEC technicians and the quality assurance supervisor…acknowledged parts accountability during MEC assembly is dependent upon individual technician efforts.
The President of the Board opined that:
…there was a lack of adequate procedural controls to ensure that only required MEC parts were provided to MEC mechanics during assembly and that no excess MEC parts were retained by mechanics after disassembly, overhaul and re-assembly.
Furthermore, it is my opinion that the lack of parts accountability by itself was not responsible for the mishap, but could have potentially decreased the likelihood of omitting required MEC parts during re-assembly.
He went on to comment that other factors must also be considered, namely:
- the MEC overhaul technician determination of whether to reuse serviceable parts
- the small size of the missing anti-rotation pin
- task complexity
- human error.
These factors led me to conclude that the misassembly of the differential pressure pilot valve could still have occurred, even if an adequate parts accountability program was in place.
In addition to the causal missing parts of the incorrectly assembled MEC differential pressure pilot valve; the MA [Mishap Aircraft] MEC teardown and post-mishap technical analysis revealed an unidentified backing ring (or foreign object debris) and an incorrect Vitron seal within the MA MEC.
Moreover, it was identified that the MEC overhaul work control documents do not address or require inventory of MEC parts post disassembly or prior to assembly of MECs.
Lastly, some MEC part kits provided to mechanics were observed to have excess parts. This fact combined with the retention of excess parts from previous MEC overhauls, results in no definitive methodology to determine that all MEC parts are used during the assembly. It is critically important to ensure that all small washers, shims, pins, clips, and retaining rings are accounted for during the MEC overhaul process, in accordance with the applicable T.O. guidance.
Omitting or improperly installing any of these items, as stated in the T.O., did result in failure of the MEC and aircraft loss. The 552d CMMXS/MSDPAA procedural requirements were not adequate and substantially contributed to the misassembled differential pressure pilot valve in the MA MEC.
UPDATE 5 February 2019: The Government Accountability Office (GAO) issue a report, ‘Strategy Needed to Improve Retention of Experienced Air Force Aircraft Maintainers’, which says while the USAF reduced the overall gap between the actual and authorised levels of maintainer staff levels from 4,016 in fiscal year 2015, to 745 in fiscal year 2017, in seven of the last eight fiscal years the USAF had staffing gaps of more-experienced maintainers. These are the people needed to train new maintainers. By hiring more novice maintainers the USAF have not addressed the experience gap. The USAF has a round 100,000 maintainers (including Reserves). They also note that “the Air National Guard has had consistent aircraft maintainer staffing gaps from fiscal years 2010 through 2017— ranging from 84 percent to 89 percent of authorized levels filled”.
UPDATE 25 April 2020: Hydraulic failure caused F-16 to crash near March base last year, Air Force says
…improper installation of two hydraulic check valves…resulted in the loss of sufficient hydraulic pressure to control the [F-16]. …an inadequate [flight-control system] overhaul process that lacked an effective procedure to identify improper installation of ISA check valves was a substantially contributing factor.
Our Comments
Meeting the defined training standard and having error free paperwork are no guarantee of success as the multiple cases of FOD, inappropriately fitted components and omitted components here show.
Internal audits therefore need to look beyond paperwork to examine work practices and both investigations and internal assurance activity need to look at the actual training and the resultant learning not just the records of completed training.
Aerossurance worked with the Flight Safety Foundation (FSF) to create a Maintenance Observation Program (MOP) requirement for their contractible BARSOHO offshore helicopter Safety Performance Requirements to help learning about routine maintenance and then to initiate safety improvements:
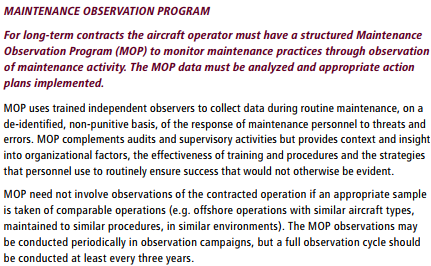
Aerossurance can provide practice guidance and specialist support to successfully implement a MOP.
Other Safety Resources
- USAF RC-135V Rivet Joint Oxygen Fire: A military accident investigation has paradoxically determined that a $62.4mn fire was due to a maintenance error but that no human factors were involved.
- Production Errors on a SAR Helicopter Full Ice Protection System
- United Airways Suffers from ED (Error Dysfunction)
- Professor James Reason’s 12 Principles of Error Management
- Back to the Future: Error Management
- Safety Performance Listening and Learning – AEROSPACE March 2017
- Maintenance Human Factors: The Next Generation
- Airworthiness Matters: Next Generation Maintenance Human Factors
- Machining Defect Cause of V2500 Failure
- Micro FOD: Cessna 208B Grand Caravan Engine Failure & Forced Landing
- UPDATE 24 June 2018: B1900D Emergency Landing: Maintenance Standards & Practices
- UPDATE 4 August: 2018: US HEMS EC135 Dual Engine Failure: 7 July 2018
- UPDATE 31 August 2018: Retired Air Force Four-Star: How to Solve Aviation Crisis
- UPDATE 22 July 2020: NDI Process Failures Preceded B777 PW4077 Engine FBO
…the best solution is for senior officials to keep the door open and have ongoing conversations on potential problems. “It’s not as much oversight as much as it is … going out and talking with [individuals] … just seeing what’s going on…”
- UPDATE 13 November 2018: Inadequate Maintenance, An Engine Failure and Mishandling: Crash of a USAF WC-130H
- UPDATE 21 November 2018: The AIB report is released into another occurrence where USAF F-16CM 92-3883, at Misawa, Japan had to jettison both drop tanks after an engine power loss: The AIB President found by a preponderance of the evidence that the cause of the accident was an obsolete part that fractured, causing the engine to overheat. In 2012, maintenance personnel ordered and installed an obsolete part, a turbine frame forward fairing, years after it was replaced by a forward fairing made of stronger material and design. A preponderance of the evidence shows that during the 2012 timeframe, when the obsolete fairing was installed, there was poor enforcement of standard maintenance protocols, which was a substantially contributing factor to the mishap. Poor enforcement of standard protocols led to a failure to follow protocols when ordering and installing the obsolete forward fairing. Specifically, poor enforcement of standard maintenance protocols created an environment that tolerated improper completion of paperwork to ensure parts accountability, severe disorganization at the shop, the improper handling of parts–including a failure to separate serviceable and unserviceable parts, and failure to follow proper procedures for cannibalization (CANN) actions. Given these significant departures from standard protocols, I [the AIB President] find that the shop had an environment conducive to failing to follow protocols when ordering and replacing parts. Discussed here: USAF Engine Shop in “Disarray” with a “Method of the Madness”: F-16CM Engine Fire
- UPDATE 29 November 2018: Video and pilot interview on the Andrew’s accident.
- UPDATE 11 December 2018: Unwinding the Maintainer Mess USAF has “fixed its maintainer shortage this year, closing a gap that had grown to 4,000—6 percent of requirements—as recently as two years ago”.
- UPDATE 27 December 2018: Inadequate Maintenance at a USAF Depot Featured in Fatal USMC KC-130T Accident
- UPDATE 26 January 2019: MC-12W Loss of Control Orbiting Over Afghanistan: Lessons in Training and Urgent Operational Requirements
- UPDATE 9 February 2019: Meeting Your Waterloo: Competence Assessment and Remembering the Lessons of Past Accidents: No one was injured in this low speed derailment in London after signal maintenance errors but investigators expressed concern that the lessons about maintenance errors from the fatal triple collision at Clapham in 1988 may have been forgotten.
- UPDATE 30 March 2019: Contaminated Oxygen on ‘Air Force One’ Poor standards at a Boeing maintenance facility resulted in contamination of two oxygen systems on a USAF Presidential VC-25 (B747).
- UPDATE 30 October 2019: ‘Crazy’ KC-10 Boom Loss: Informal Maintenance Shift Handovers and Skipped Tasks

Aerossurance is pleased to sponsor the 9th European Society of Air Safety Investigators (ESASI) Regional Seminar in Riga, Latvia 23 and 24 May 2018.
Aerossurance is pleased to be both sponsoring and presenting at a Royal Aeronautical Society (RAeS) Human Factors Group: Engineering seminar Maintenance Error: Are we learning? to be held on 9 May 2019 at Cranfield University.