A Second from Disaster: RNoAF C-130J Near CFIT (Recommendations on Risk Management, Safety Culture & Independent Regulation)
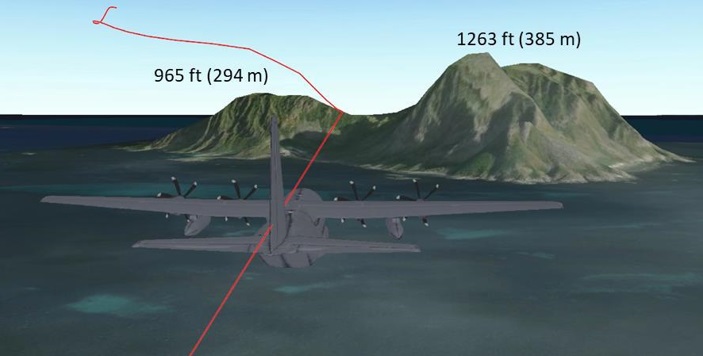
On the evening of 11 March 2020 a Royal Norwegian Air Force (RNoAF) Lockheed MartinC-130JHercules with eight people on board nearly crashed into the rocky island of Mosken in Værøy municipality, Lofoten. After a last-minute evasive manoeuvre the aircraft cleared the island by 144 ft, avoiding a Controlled Flight into Terrain (CFIT). The Norwegian Safety Investigation Authority (NSIA) say (emphasis added) :
If the manoeuvre…had been initiated less than a second later, it would have resulted in a catastrophic collision…
Flight Path of RoNAF C-130J Hercules Mustang 31 During a Near CFIT with Mosken Island (Credit: RNoAF via NSIA)
The aircraft was from 335 Squadron, the RNoAF airlift squadron, based at Gardermoen, which operated four C-130Js at the time. The C-130J was introduced to replace the C-130H in 2008/2009.
The Serious Incident
The NSIA, formerly the Accident Investigation Board Norway (AIBN), explain in their safety investigation report (c 50,000 words, issued in Norwegian on 19 April 2021) that the aircraft the lead of a pair C-130Js, Mustang 31 (MG31) and Mustang 32 (MG32), on low-level navigation exercise (navex) as part of Exercise Cold Response.
Planning and briefing followed the standard procedure which included a joint review of the mission for all participating aircraft and formations. However, the low-level navex was introduced part way through the planning at the request of 335 Squadron. The unit wanted to apply a new low-level technique using Night Vision Imaging System (NVIS). ‘Low-level’ here is relative as it was planned at 1,000 ft.
The flight was authorised by the Supervisor of Flying (SOF) on the basis the crews would ‘try and see’ if lighting that night would be sufficient to meet a regulatory minimum of 2.2 millilux of light. The crews completed a risk assessment that was counter-signed by the SOF. An instructor was Pilot Flying of MG31 and the aircraft commander sat in the right-hand seat as Pilot Monitoring.
Start-up, taxi and departure from Bodø (ENBO) proceeded normally. It was relatively bright at the departure time at 1826 and some crew members chose not to use NVGs during the first part of the trip.
It soon became clear that the weather did not allow Visual Meteorological Conditions (VMC) to fly at a planned altitude of 1,000 ft. To avoid flying into the low cloud cover, the formation chose to go down to approx. 500 ft – a height that was maintained until the incident occurred.
Lockheed Martin C-130J Hercules Cockpit (Credit: NSIA)
The C-130J has a Head Up Display (HUD), but navigation uses a digital map on one of four digital screens (the Head Down Display [HDD]) accompanied by a paper map.
The crew on the MG31 wanted to use the NVIS illumination in the cockpit, but the HUD on the left side did not have sufficient brightness in this configuration. The crew of the MG31 therefore choose to use normal cockpit lighting which they dimmed manually. In MG32, the NVIS lighting worked as intended.
NSIA note that the NVIS amplifies ambient light 5-10 000 times but has some limitations:
A critical limitation of operating with NVGs with a nominal 40° FOV is that it seriously degrades the ability to constantly acquire information from the environment, build up a mental picture of the immediate scene out of the NVGs’ FOV, and maintain adequate SA.
FOV restriction can thus result in longer spatial task completion, less precision, and degraded cognitive maps. Greater attentional resources are needed to perform with NVGs, and as a result, higher workload can account for the degraded spatial performance. …it may also result in physical and mental fatigue as well as spatial disorientation.
Furthermore, it can be a problem that the pilots have an overconfidence related to the use of NVG and how well it works.
At 2021 the formation received clearance to commence the navex. However, the instructor, who was PF MG31, proposed they should fly a more direct route back to Bodø.
At 2023, PF MG31 noticed that the weather conditions were bad, and they were starting to get terrain and some islands in front of them. PM MG31 replied that it was dark and that it looked bad. PF MG32 came shortly afterwards with input that the conditions were not sufficient to fly the impending low-flying route at Bodø.
NSIA research indicates that the lighting conditions were likely <1 millilux.
The crews of the two aircraft agreed to cancel the low-flying route and rather split up the formation and continue the flight on separate clearances. MG32 continued VFR into Bodø. PM MG31 started the coordination with the air traffic service to continue the flight on IFR clearance to Evenes.
Less than a minute before the near-collision, the crews were in the process of completing a split up of the formation. When PF MG31 ordered PF MG32 to separate the formation, he also announced that the island of Værøy was on the right.
Both aircraft were still heading directly towards the island of Mosken.
Mosken Seen in Daylight from Værøy (Credit: Jostein Torstensen via NSIA)
Several of the crew members have explained that they looked at the screens in the cockpit (HDD) on several occasions prior to the passage of Mosken, but without the island being discovered. An internal defense report describes that several factors can help to explain this, such as the chosen light intensity on the HDD that showed digital map, the size of the screen, the size of the island, location of the “cursor”, and other and more prominent symbology on the map and area boundaries.
PF MG31 has explained that almost all attention was directed out of the cockpit… PM MG31 explained that he spent a lot of capacity on communication with the air traffic service during this period.
At this time, the crew had selected the NAV RADAR display with Monopulse Ground Map (MGM) on HDD 1 and 4 in the cockpit. In this configuration, terrain is displayed in front of the aircraft, but without colour. This function is selected, among other things, when approaching the Instrument Meteorological Conditions (IMC) from the open sea to land in order to be able to confirm the aircraft’s position and distance from land.
The aircraft was about 500 ft AGL at 200 kt.
At 20:26:02, PF MG31 made a turn to the left and three seconds later he discovered the terrain in front of the plane visually with NVG and immediately started a maneuver to avoid collisions.
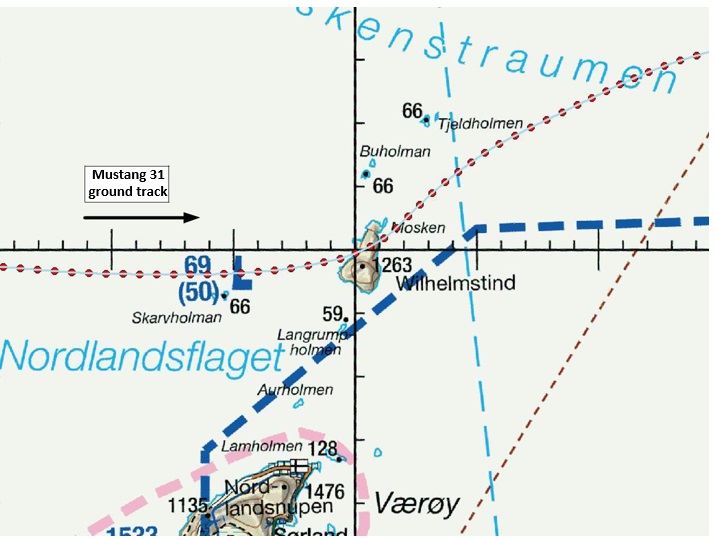
Mustang 31 Ground Track (Credit: NSIA)
The maneuver meant that the nose of the aircraft was raised at the same time as PF selected TAKEOFF power on all four engines. When the PF MG31 pushed the throttle levers to the forward position, the levers were automatically retracted since the autothrottle was still active. The reduced engine power lasted for about 10 seconds before the PF was manually disconnected from the autothrottle and full engine power was given again on all four engines.
A turn to the left was maintained during the first part of the maneuver. As the nose of the aircraft was raised to an angle of 14.3°, a vertical acceleration of 1.95 G was recorded. After four seconds, the aircraft had reached the peakbank angle of 22° before the wings were levelled.
The climb continued while the angle of the aircraft’s nose was gradually reduced to 8.2°. The speed was maintained at close to 200 kt.
About 13 seconds after the climb was initiated, a warning came from one of the aircraft’s Ground Collision Avoidance System (GCAS [i.e GPWS]), both in the form of “Altitude” warning and “Pull-Up” warning.
GCAS provides audiovisual alerts in situations that may lead to collisions with the terrain. Such alerts are based on real-time data from the aircraft’s position, configuration, speed and altitude, but without the use of terrain models [that if available would provide the full] Terrain Awareness and Warning System (TAWS) [capability].
As discussed in a previous Aerossurance article Extreme Latitudes – Extra CFIT Risk, that discussed a 2012 RNoAF C-130J CFIT into Mount Kebnekaise in Sweden, the terrain database was not available at high latitudes (>60º N). After an 8-year project one only became available in 2020, after this serious incident. The full TAWS functionality would have given a warning at 1.4 nm (c 25 s of warning).
At 20:26:19, 14 seconds after the obstacle was discovered, the MG31 passed the northern part Mosken with 144 ft clearance. The climb then continued uninterrupted to a cleared height of 5,000 ft.
Onboard MG32 the crew…
…identified terrain via the digital map and on weather radar…approx. 30 seconds before MG31 made its evasive manoeuvre. Due to limited situational awareness, the crew in MG32 did not notify [MG31 of] the terrain.
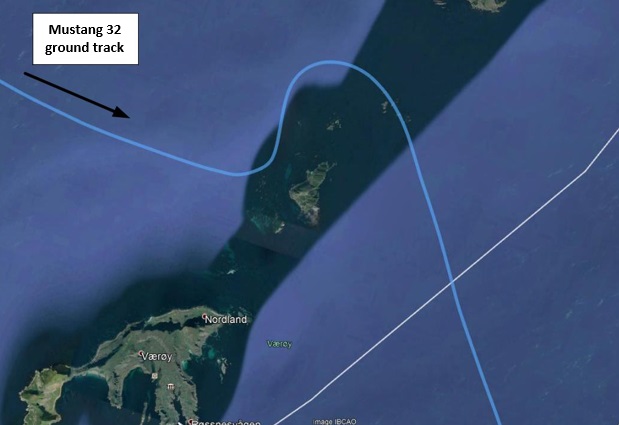
The crew of MG32 completed a horizontal avoidance manoeuvre.
Mustang 32 Ground Track (Credit: NSIA)
The NSIA Safety Investigation
The NSIA applied a 7-stage framework to their investigation (‘the NSIA method’) and in their analysis go on to examine Crew Resource Management (CRM), Risk Management, Safety Culture, the 2012 CFIT in Sweden, Safety Management and Supervision (by which they mean regulatory oversight).
NSIA note that the low-flying portion added a “complex” and “high risk” element to the flight. The crews’ dynamic risk assessment “was deficient and did not contribute sufficiently to identifying and correcting the risk”. The investigators suggest this was due to the demands of flying reliant on NVIS, “a false sense of security over the sea”, and the pressure of “delivery”, “press” or “performance” culture.
It emerges from the interviews that flexibility is a trait that is valued in the squadron. The pilots themselves express a strong motivation to deliver and complete missions.
An internal desire to perform, as well as an external pressure for delivery from management and other players, may have contributed to reducing the safety margins in the operations at 335 Squadron…
The investigators note that this can be found across and at different levels within RNoAF. In 2017/18 various initiatives aimed at creating a better balance of demand and resource had been launched by the RNoAF.
The investigators determine CRM “did not work satisfactorily”, noting that RNoAF CRM training was not standardised and was left to individual units.
…this deficiency has also been addressed in previous internal reports, most recently in connection with a serious incident with a Sea King SAR helicopter on 17 May 2018.
On risk management:
The Air Force had not established acceptance criteria and requirements for mitigations in risk assessments. 335 Squadron’s risk assessment…were primarily an awareness-raising tool. There was little system for reviewing, assessing, deciding and evaluating the effect of any risk-reducing measures.
When operating at low-level >60º N, beyond the area in the TAWS database NSIA say “the pilots and the regulations formed the primary safety barriers against collisions with terrain”. They contend too, that:
[Flight] Authorization cannot be considered an independent security barrier since the authorization authority is delegated to personnel who are part of the operational environment. The integrity of these barriers was not sufficiently ensured through competence and risk understanding. Like the crews, [the SOF] lacked sufficient knowledge of the regulations regarding weather minima.
The investigators note:
There is generally understaffing on the pilot side of the Air Force.
335 Squadron also had a broad and demanding mission portfolio. This led to a high workload, lack of common arenas, and less time for developing resilience / training. Every assignment was therefore used as an opportunity to conduct training and maintain qualifications.
The investigators highlight that an internal study identified that the RNoAF “almost only emphasizes just culture”, rather than other elements that James Reason identified as aspects of a safety culture. This is sadly not an uncommon problem. The NSIA say the RNoAF “does not have a sufficiently “informed” and learning culture” saying if the…
…culture had been “informed”, they would have seen to a greater extent that eagerness to be solution-oriented and handle emerging issues could damage the ability to achieve organizational learning.
They also point out a number of safety initiatives were not evidence based and that…
Many of the findings related to the Kebnekaise accident were followed up by the Air Force in the following years, but it did not lead to sufficient fundamental and systemic changes.
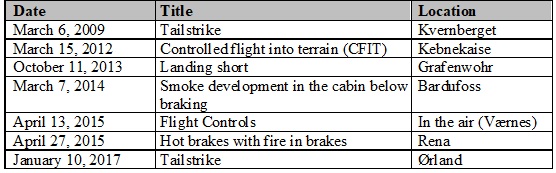
The Air Force had not identified the C-130J as a high-risk aircraft system, despite six investigated incidents and a fatal accident within 12 years (2008–2020).
Recommendations and findings after incidents and accidents do not appear to have been adequately followed up.
They comment that the RNoAF approach to safety means elements of an SMS have been implemented individually but not integrated. 335 Squadron had also not been inspected for 8 years.
NSIA comment that the military regulation were paradoxically, both “complex” and had “gaps and shortcomings”. They say:
This may over time have affected the squadron’s respect and compliance with the regulations.
The defence sector lacks an independent and comprehensive military aviation authority that is separate from the Air Force as an operator of military aircraft, and Defence Materiel as an ownership manager and procurement authority for military aircraft. There are three internal actors who have a mandate to supervise military aviation, but the mandates are authorised in different places. It appears to be fragmented and unnecessarily complicated, and it can lead to role conflicts and to the oversight function being weakened as a barrier.
They also colourfully describe having the military regulate themselves by use of the Norwegian expression «bukken som passer havresekken» i.e. ‘putting a deer in charge of an oatmeal bag’. That foxed us (no pun intended) at first, but it’s the same as ‘putting the fox in charge of the hen house’.
RNoAF C-130J (Credit: Mark Harkin CC BY 2.0)
NSIA Conclusions
NSIA concluded that…
…the incident is due to a combination of local conditions, active actions and latent weaknesses.
The local conditions can be related to a combination of demanding weather and light conditions, low-flying with night optics and it being a check ride for the aircraft commander [of MG31].
The active actions were that the formation deviated from the pre-planned route and failure in the crew cooperation. In addition, the authorized assignment entailed too high a risk and was not in line with the regulations for operations with the C-130J. The authorization process thus did not act as a safety barrier.
The latent weaknesses can in particular be linked to the Air Force’s safetymanagement, delivery pressure combined with understaffing and a performance culture, as well as insufficient regulatory oversight. The Air Force’s management had not identified any weaknesses in safety at 335 Squadron.
NSIA supports the recommendations given in an internal defense investigation report and the further guidelines from the Chief of the Air Force. At the same time, NSIA believes that the Air Force should work more thoroughly on safety management, including risk management, competence and safety culture.
NSIA also questions whether the Air Force itself is able to uncover and correct its own systemic safety problems, and believes that the investigation reveals the need for an external regulatory body.
NSIA Safety Recommendations
2021/05T: …the RNoAF review and improve its risk management procedures in terms of identification of hazards, safety barriers and risk factors, as well as acceptance criteria, requirements for compensatory measures and follow-up of the above.
2021/06T: …the RNoAF conduct a survey to enable it to describe and understand the organisation’s safety culture, both at command level and in operational units, as well as possible. Such a survey can establish a benchmark for subsequent safety work and efforts to improve the organisation’s safety culture.
2021/07T …the Ministry of Defence establish an independent and comprehensive military aviation authority (supervisory authority). This aviation authority must be allocated new resources and not be established at the expense of the RNoAF‘s existing activities.
We also highly recommend this case study: ‘Beyond SMS’ by Andy Evans (our founder) & John Parker in Flight Safety Foundation, AeroSafety World, May 2008, which discusses the importance of leadership in influencing culture.
Aerossurance has extensive military & civil air safety, operations, SAR, airworthiness, human factors, aviation regulation and safety analysis experience. For practical aviation advice you can trust, contact us at: enquiries@aerossurance.com