Rescuers Alongside the Royal Netherlands Navy NH90 N-324 in the Caribbean: Note the Pilot’s Inflated Personal Liferaft (Credit: IVD)
The Dutch Safety Board (DSB or Onderzoeksraad) issued a safety investigation report (in Dutch only) on 9 December 2020. They concluded a water impact occurred after airspeed reduced during the downwind leg with insufficient power input at a height that prevented recovery (a Loss of Control-Inflight [LOC-I]). They also highlighted survival issues associated with the two fatalities. Just 3 days later we published our analysis of the DSB to highlight some of the important lessons: NH90 Caribbean Loss of Control – Inflight, Water Impact and Survivability Issues.
The Defence Safety Inspectorate (IVD) have now published their deeper investigation report (issued, again in Dutch only, on 2 December 2021). The IVD confirmed the DSB conclusions and make 5 safety recommendations. In this article we are going to concentrate on the survivability aspects.
Rescuers Alongside the Royal Netherlands Navy NH90 N-324 in the Caribbean (Credit: RNLN)
The Water Impact and Capsize
On the eighth flight the helicopter did a lower circuit than before, less than 100 ft, as the plan was to take photos of the ship. The ship was steaming at just 3 knots in a direction of 108º and the wind was from 100º and 20-25 knots. The waves were 3 m high, the air temperature 31ºC and the sea temperature 29ºC. The helicopter passed down the right-hand side of the ship downwind:
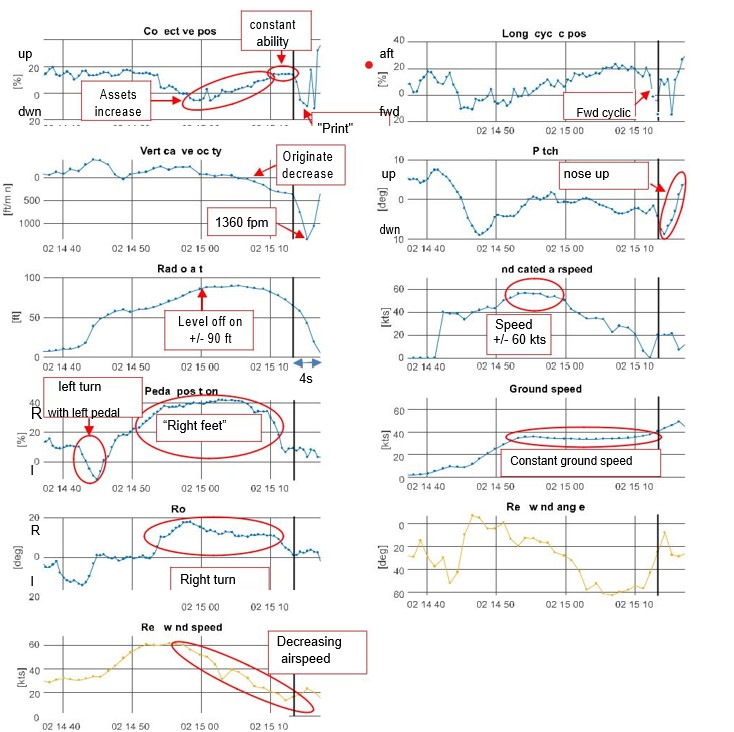
Because the ground speed was kept almost constant at 38 knots during the turn and the helicopter turned to downwind (with a tailwind), the airspeed decreased. With decreasing speed below 80 knots, more power was needed to keep flying horizontally at the same height.
FDR Data for NH90 N-324 (Credit: IVD/NLR)
The helicopter started to descend with the descent speed initially increasing to about 370 feet per minute (fpm) at a height of 67 feet (about 20 meters) above the water’s surface. It is unclear whether the crew was aware that speed and altitude were decreasing.
One second before the helicopter had descended to 67 feet, the pilot gave a forward input to the cyclic stick and then reduced power by 24 percent by moving the collective down. This further increased the rate of descent to 1,360 fpm and it became inevitable that the helicopter would hit the water.
Upon impact the tail broke away. The IVD say that the simultaneous shift in CG and the loss of tail rotor torque meant the aircraft overturned “almost immediately”. The emergency flotation system was armed and automatically deployed, so the aircraft remained floating inverted.
Crew Positions, Aircrew Equipment Assembly (AEA) and Cabin Safety Equipment
There were four occupants on board at the time of the accident; in the front sat a pilot as captain (Pilot in Command, PIC) and a Tactical Coordinator (TACCO), in the back sat a Helicopter Sensor Operator (HSO) and a Rescue Operator Airborne Marksman (ROAM).
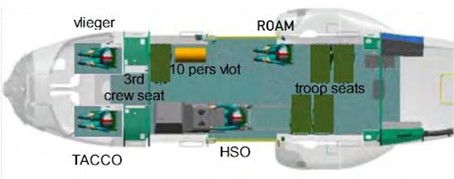
Layout NH90 N-324 , Excluding Shooting Box and Automatic Weapon in Right Hand Cabin Doorway (Credit: IVD)
The helicopter was configured as standard for an operation in the Caribbean at the time of the accident. In the cabin, near the right cabin door, there was a gun mount with an automatic weapon on it.
The helicopter had crashworthy energy absorbing seats.
The cockpit seats…have extensive adjustment options and are equipped with two armrests and a five-point belt that automatically locks in the event of a substantial deceleration. The occupants sit on a [Zodiac Aerospace (Aerazur)] Crew Survival Pack (CSP) that is connected to their life jacket / survival vest [by a lanyard], so that the flight crew automatically takes it with them if they have to leave the helicopter in an emergency.
The HSO seat in the cabin is identical to that in the cockpit, but does not have armrests.
The NH90 has troop seats for the transport of passengers in the cabin. The number of seats installed depends on the configuration and, if installed, transverse to the direction of flight with the backrest mounted against the cabin wall. The troop seats were not occupied during this flight.
The seat for the ROAM is identical to the troop seats, with the difference that it is mounted in the flight direction…behind the right sliding door.
At the time the HSO sitting on the ‘shooting box’ in the right hand doorway next to the automatic weapon and the ROAM was in their seat but unstrapped.
NH90 N-324: Cabin Layout with ROAM’s Troopseat, Automatic Weapon and Shooting Box (with padded seat), in the Right Hand Doorway (working forwards) (Credit: IVD)
Both were connected to the helicopter only by means of their cabin safety line.
All doors of the NH90 are equipped with a mechanism that allows them to be ejected completely in an emergency. There is a lever on each door that operates the mechanism, both on the inside and the outside. On the inside of the sliding doors of the cabin (cabin sliding doors), this handle is covered with a cover that must first be removed before the handle can be operated.
NH90 N-324: Covered Cabin Door Jettison Handle (Credit: IVD)
The sliding door was equipped with push out windows which require the removal of a rubber seal to use.
A ten-person raft is placed on a troop seat in the front right of the cabin, which is intended for the crew members and passengers who do not have a personal life raft, such as the ROAM.
[The] crew members were equipped with a survival vest [Mk 5 for front crew and Mk 7 for rear crew] , personal protective equipment, signalling equipment and an emergency radio that are carried in the survival vest or flight coveralls.
The Mk 7 primarily differs in having a fall protection attachment point for a cabin safety line.
In order to be able to escape quickly in an emergency, this attachment point is equipped with a quick release mechanism that is operated by means of a handle on the left front of the vest. The handle is covered with a textile flap that is held in place with Velcro, so that the quick release handle cannot be accidentally activated.
For all crew:
During flights over water, a flotation device is zipped onto the vest, similar to a life jacket.
NH90 N-324: Front Crew Mk 5 Survival Vest / Life Jacket (Credit: IVD)
On the left front of the Mk 5 vest there is a ‘SEA’ Compressed Air – Emergency Breathing System (CA-EBS) on overwater flights. On the right-hand side of the vest there is a pocket containing a belt cutter. Due to the location of the attachment point on the Mk 7, the rear crew CA-EBS bottle is mounted on the right side of the vest.
The crew had all undergone Helicopter Underwater Escape Training (HUET) using a Modular Egress Training System (METS).
Survivability: Front Crew Escape Attempts
The cockpit crew are trained to egress after jettisoning their cockpit door in the following sequence in the event of a capsize:
Helicopter enters water
Take one last breath before submerging
Wait until the helicopter is stable
Activate the CA-EBS
Disconnect their intercom communication cable
Jettison door
Find and hold reference point
Release their seat harness
Escape
The life jacket should only be activated outside the aircraft.
The TACCO was found lifeless strapped into their seat by rescuers. Their life jacket had been activated. Although the TACCO’s seat had not ‘stroked’ (indicating a relatively low energy impact) the TACCO had suffered a “mild traumatic brain injury, consistent with a concussion”. The investigators postulate “it is likely that he activated his vest in a state of confusion”.
They also note that the TACCO’s seat was in its rearmost position. This is a common practice so a TACCO is clear of the flight controls. The investigators however note that:
During a reconstruction, persons of the same stature as the TACCO could not reach the door ejector lever from this position if the seat belt tensioner was locked.
The TACCO’s CA-EBS bottle was found loose in the cockpit unactivated. The investigators were not able to determine if it separated on impact or if the TACCO had extracted and dropped it.
The pilot was recovered by rescuers on the surface, floating face down. She had died of drowning.
The right cockpit door had been jettisoned by the helicopter’s ejector handle. The seat belts were loose and were recovered from the helicopter without damage. Measurements on the seat show no deformations due to impact. During examination injuries to the mouth were found, which are consistent with the use of the CA-EBS during the attempt to escape from the helicopter. When leaving the helicopter, the Crew Survival Pack, containing the personal life raft, came with the pilot.
However, investigators came to the conclusion that the lanyard that connected the CSP to the pilot’s survival vest most likely snagged on the helicopter during the pilot’s egress. During trial’s the IVD identified several points in the cockpit where the lanyard can get caught during an escape. These included the armrest, seat adjustment levers and cyclic stick. If rather than coiled under the CSP the lanyard is left draped over the side of the seat, the risk of snagging (on the adjustment levers) increases.
It is likely that during the escape from the helicopter the lanyard caught on one of the adjustment handles of the seat. In the pilot’s attempts to continue the escape, the lanyard tightened, activating the liferaft, which ascended to the surface pulling the pilot down and preventing her from resurfacing.
NH90 N-324: Arrival of First Fast Rescue Craft (FRC) Alongside Wreckage: Note the Pilot’s Personal Liferaft Inflated on the Surface (Credit: via IVD)
The investigators also discovered that this had been identified in trials in 2012 when the Mk 5 and Mk 7 vests were introduced. However remarkably, as the exiting CSP lanyard was not the subject of the trial “the test team paid no further attention to it in this evaluation”.
[The] Survival Rescue Officer of 860 Squadron had attempted to have the Crew Survival Pack’s lanyard adjusted in response to the problems identified during the life jacket tests. The intention was for the lanyard to come out of the Crew Survival Pack not through the front but the right side. The lanyard also had to be shortened [so it] could be attached directly to the vest on the right side and it would no longer be able to get caught behind anything during an escape.
The Survival Rescue Officer considered this modification desirable in 2012 and contacted the NH90 Project Bureau of the Defence Materiel Organization (DMO) with the request to see whether the modification could be carried out.
The Project Office contacted the French military but found that…
…French users of the NH90 were happy to maintain the prescribed position and routing of the lanyard At the time, DMO indicated that the Defence Helicopter Command could submit the formal need for such a modification via ‘the usual channels’. In a response to DMO’s message, the Survival Rescue Officer of 860 Squadron announced that a solution was being worked on locally by attaching the lanyard to the CSP with breaking thread. That way the crew would not be hindered by the too long safety line. If this adaptation were not sufficient, a need for modification would still be submitted.
Investigators found that no design modification was ever progressed, and any local use of breaking thread had been discontinued before the accident. They also discovered that the maintenance data does not explicitly state the correct routing for the CSP lanyard (it is merely implied by the accompanying illustrations), opening up the possibility it will be misrouted. The investigators note that the CSP lanyard…
…is connected to the survival vest with a spring-loaded quick release.
NH90 N-324: Reconstruction of a Misrouted CSP Lanyard (Credit: IVD)
The quick release can be opened by pulling against the spring pressure, releasing the vest from the rest of the line, and thus from the raft.
However, crucially:
This procedure is not taught. During training, crew members are taught that this line must always remain connected to the vest until rescued to prevent crewmember and raft from being separated.
The belt cutter was stowed in the pilot’s survival vest. The use of this device is discussed during theoretical training but is not used during practical training.
Survivability: Rear Crew Escape
The HSO stated in the investigation that he did not foresee the impact with the water. When the helicopter hit the water, he was thrown from the gun box on the right side of the cabin to the front left of the cabin and hit the bulkhead. He injured his left shoulder and became somewhat dazed and disoriented. Shortly after, he realized what had happened and saw the helicopter filling with water.
He used his CA-EBS and started to orientate himself in the cabin by slowly moving backwards by feel in the direction of the HSO station and the associated seat. He recognized the two crosswise metal strips on the back of the HSO chair and was able to orientate himself from there. He tried to reach the ejector mechanism of the left sliding door but could not find it.
The investigators comment that:
The marking of the control lever for the ejection mechanism of the cabin doors and windows is not clearly distinguishable. This makes it difficult for the crew to find the levers in an emergency.
He then pulled the rubber seal from the window in the left sliding door to eject the window. Banging on the glass did not have the desired effect. By pressing on one of the corners, the window eventually came loose and the escape route to the outside was open.
The windows are designed to push out with a force in the corners. Its not clear in the IVD report if the crew training was clear on this point.
At this point the HSO’s foot contacted the ROAM.
After the HSO had already partially worked his way out, he realized that he was still attached to the helicopter with his fall protection. He partly entered the cabin again to release the carabiner [attached to the aircraft]. Once surfacing, he activated his life jacket and took off his helmet.
In contrast, the ROAM did anticipate the water impact in the final moments of flight:
He saw the surface of the water rushing toward the helicopter and braced himself against the gun mount to absorb the impact. He remained seated in his chair.
He acted immediately after impact to escape from the helicopter. He wanted to eject the right cabin door using the ejector mechanism, but soon lost track of where the lever was because of the inflowing water and the gun mount in the way.
The ROAM then removed the seal from one of the push out windows but…
…was unable to push the window out. He could not remove the glass because, in his opinion, there was still too great a pressure difference with the water pressure outside.
In the meantime, the cabin filled with water and the helicopter overturned, after which it ended up in the water upside down. The ROAM became disoriented.
This was also when he placed the mouthpiece of the CA-EBS and started breathing with the help of the bottle. At first he tried to orientate himself via the safety line to the roof of the helicopter, which by now had become the lowest point and was under water. He could hardly see anything underwater. After feeling up and down in the cabin a few times, he felt the HSO’s foot and decided to leave the helicopter behind him. Like the HSO, he released the fall protection by releasing a carabiner.
Once on the surface the ROAM activated his life jacket and removed his helmet. The investigators comment that:
During the escape training, crew members are taught to remain seated until the helicopter comes to a standstill. The reason for this is, among other things, to prevent a crew member from becoming disoriented when trying to find his way in a moving helicopter. The ROAM has started moving earlier in the hope that this would give him a time advantage. He declared however that after the helicopter overturned, he became disoriented and so had to search for an exit for a long time.
Once they had escaped the cabin:
The HSO and the ROAM stayed together above water with inflated life jackets, but without a life raft.
The sea conditions made it difficult to stay together Although the life jackets were fully deployed, they did not float well and had to tread firmly to keep their heads above water.
The IVD say that three aspects stand out in the escape of the rear crew:
Both rear crew were attached to the helicopter with their fall protection and freed themselves during their escape by releasing the carabiner. The HSO had to return to the cabin for this, which took time and involved a risk. The survival vest…had a quick-release fastener…but they did not use this because they were unfamiliar with the system.
The rear crew escaped without a liferaft. In this situation this was not a problem because the helicopter entered the water next to the ship and the water temperature was about 25 degrees. At lower water temperatures or when rescue takes longer, the chances of survival with a raft increase significantly.
Both cabin members took off their helmets above water because they assumed that it was still attached to the helicopter with the intercom cable. The helmet protects the head and also prevents it from cooling down quickly. In [training] it is taught to keep the helmet on until you are in the raft. In this case there was no need to keep the helmet on, given the temperature of the outside air and seawater and the proximity of the ship allowing a quick rescue.
The investigation also identified that the rear crew had only every worn Mk 5 survival vests during training, so they had not been able to train with the fall protection quick release and had trained with the CA-EBS mounted on the opposite side.
NH90 N-324: Both of the Goningen’s Rescue Craft Alongside the Wreckage as an Attempt was Made to Rescue the TACCO (Credit: via IVD)
Egress Training
The investigators identified that the military Survival Evasion Resistance and Escape (SERE) School at Gilze-Rijen Air Base where the aircrew had trained were not aware of what equipment the rear crew routinely used.
They note that the METS is a procedural trainer used for multiple aircraft types. They highlight that the NH90 operates in multiple cabin configurations too and the METS is used with just one configuration.
Furthermore a ‘dry’ practice on the aircraft of door jettison and egress had been abandoned after the first training in 2010 because of a lack of spare parts and a two week delay to put the aircraft used back into service. Since the accident blindfolded dry training has been reintroduced.
The IVD reflected:
Based on this research, the Inspectorate sees room for improvement in both management and feedback in order to obtain and maintain the necessary skills for underwater escapes. This concerns the requirements…set for the training, the resources to be used, the manner of management, the monitoring thereof and the adequate response to shortcomings identified in practice and in the curriculum.
The priority of the SERE school is to carry out the extensive training package. With the current staffing level, people are able to provide survival training, but there is a lack of capacity to evaluate, improve or substantiate the training with an up-to-date and thorough educational curriculum. This makes it difficult to guarantee the quality of these training courses.
Differences between the training resources and the actual operational resources have made the escape from the helicopter more difficult. Also, not all safety equipment is taught at the SERE school when it comes to non-standard evacuations. For example, the use of quick-release fasteners and the seat belt cutter is not practiced during the training and the school does not have all the vest types with which the helicopter crew actually operates.
Wreckage of NH90 N-324 at Gilze-Rijen Air Base After Recovery (Credit: via IVD)
Our Observations
Although the IVD (inevitably in the circumstances) recommend improving training there are disappointingly no recommendations on the design, test & evaluation of aircraft equipment or AEA, nor on managing issues identified in-service.
Aerossurance has extensive air safety, operations, SAR, airworthiness, human factors, survivability, aviation regulation and safety analysis experience. For practical aviation advice you can trust, contact us at: enquiries@aerossurance.com