Canadian Coast Guard Helicopter Accident: CFIT, Survivability and More
17 December 2015
Canadian Coast Guard (CCG) Helicopter Accident: CFIT, Survivability and More (Bo105 C-GCFU)
A fatal Arctic Controlled Flight Into Terrain (CFIT) accident to a Canadian Coast Guard (CCG) helicopter highlights a host of safety lessons, including:
Low level operation with varying visual clues
Compliance with approved maintenance data
Survivability
Alerting / Flight following
Search and Rescue
Data recorders
Regulatory oversight
Wreckage of Bo105 C-GCFU During Recovery (Credit: TSB)
The Accident
The Transportation Safety Board of Canada (TSB) has recently issued their report into the accident to CCG Bo105S CDN-BS-4C-GCFU in the M’Clure Strait, Northwest Territories on 9 September 2013. The aircraft was one of a fleet CCG use in support of various tasks and operated by Transport Canada, Aircraft Services Directorate (TC ASD). The CCG Bo105s are currently being replaced by Bell429 under the CCG Fleet Renewal Plan.
At 1638 local time, the helicopter departed from CCG Ship Amundsen for an ice measurement and reconnaissance flight. The ship was chartered at the time by ArcticNet in support of an 82-day scientific mission. The pilot was accompanied by the ship’s master and a scientist. Ice measurement requires low level flying.
The TSB report that one hour later, at 1738:14, the pilot:
…called the CCGS Amundsen to report that its estimated time of arrival (ETA) was in 10 minutes. At that time, the helicopter was in descent at approximately 390 feet. That was the last recorded message from the pilot. The helicopter continued its descent toward the survey altitude and levelled off at 36 feet at 1739:19, while eastbound. For a period of 3 minutes and 30 seconds, the helicopter maintained an altitude varying between 23 and 39 feet. It then made a slow descent for 13 seconds before colliding with water at 1743:02. The 3 occupants evacuated the helicopter before it sank…
Upon noticing the helicopter had not arrived:
At 1805, the helicopter’s position was checked on the flight following system, which displayed it as being 3.2 nautical miles from the vessel. At 1818, the Amundsen’s crew attempted several times to communicate with the helicopter without success and soon after proceeded to the helicopter’s last position. Debris was spotted and the three occupants were recovered [between 1854 and 1907]. None survived.
The helicopter sank in 458 metres of water and was recovered 16 days later.
The Safety Investigation – Low Level Operation and Visual Clues
The aircraft was operating at low level (20-40ft typically), mostly over ice. Recovered video and still images showed that the ” visual cues and light levels varied considerably during the flight”.
Visual Clues While Flying Over Ice 10mins Before Accident (Credit: TSB)
Shortly before the accident the helicopter fly over an area of open water, approximately 2.3 nm wide.
…the winds were reported as light. Under such wind conditions, the smooth water surface presents a uniform appearance from above, somewhat like a mirror.
This would have resulted in a significant reduction in visual cues available to judge height.
The loss of references in the near visual field would have required the pilot to increase the scan of other available cues (distant visual field and instruments) in order to detect any change in altitude. Given the low altitude of the flight, this transition would have needed to be very quick, as a momentary loss of orientation could have resulted in contact with the surface. In addition, the dark overcast sky ahead would no longer have provided the distinct line of horizon against the water that would have been present when flying over the ice surface. Therefore, a pitch attitude change would have been difficult to recognize.
The helicopter was flown above the open water for approximately 89 seconds before impact.
According to data from the onboard [Flight Following System / satellite tracking system] FFS, the descent leading to the impact lasted about 13 seconds, which indicates that the pilot maintained control for 76 seconds following the loss of references in the near visual field. The 13-second descent corresponds to an average rate of descent of about 166 feet per minute with a slight increase in speed. This is consistent with a shallow descent path, which would have been difficult to recognize in the absence of adequate visual cues. A lack of adequate visual reference as the aircraft was flying over an area of open water is consistent with the facts of the occurrence and cannot be ruled out. There is a strong probability that while over the open water, the pilot experienced a lack of the visual cues required to judge altitude, which led to controlled flight into terrain (CFIT).
TC ASD had conducted a low level flying CFIT risk assessment in 2009. The risk was considered to be high because of:
distraction caused by any mechanical malfunction, such as a single engine failure, a master caution indication, or a warning tone, which can cause a lapse in concentration and result in a loss of altitude and ground contact;
lapse in concentration for any other reason, resulting in a loss of altitude and ground contact;
loss of situational awareness due to lack of, or loss of, suitable visual cues needed to determine aircraft attitude, which can cause a loss of altitude and result in ground contact; and
failure to recognize a pressure ridge in the ice due to less-than-ideal visual cues or momentary distraction causing collision with the pressure ridge.
In order for the pilot to relax his concentration level and manage the onset of fatigue and distraction… low flying [was limited] to short periods of time, usually no more than 5 minutes. This was increased to 15 minutes in June 2010, following discussions with Aircraft Services Directorate (ASD) pilots and human factors specialists. However, no new risk assessment was done to determine the level of risk associated with this increased time limit. Since 66% of the 65 minute [accident] flight was spent at low altitude, it is possible that the pilot’s concentration was reduced to a point that the shallow descent was not recognized in a timely manner to prevent the impact.
Although the risk assessment identified critical threats it is not clear how they were mitigated (with the exception of the relaxed control on duration). The TSB do not address the issue of why the aircraft was being operated so low when not conducting ice measurements and whether this had become an habitual issue (a formal of procedural drift, something we have discussed in the context of a British Arm Lynx AH9 accident). This may be partly due to lack of data recorders (see below) to provide clarity. The operation was also particularly high risk as it was operated at weights in excess of the TC ASD procedures for low level survey flights and it was being flown with the heater on, which would have rendered the aircraft unable to maintain altitude in the event of an engine failure.
The Safety Investigation – Ice Probe Installation
On the day of the accident, the helicopter was fitted with a nose mounted ice probe (visible in the photo earlier). The probe was been certified under a Supplemental Type Certificate (STC) in 2001.
Ice probe (Credit: TSB)
However, on the day of the accident the wiring was not routed as per the STC (i.e. down the left hand side of the fuselage), but down the right hand side so as to allow the fitment of a video pod on the left hand skid. The first time this configuration was flown the unapproved routing mirrored the left hand side routing (shown below). On the first flight this resulted in airspeed indication errors. Consequently the cables were rerouted below the pitot tube (seen in the centre of the photograph below), apparently curing the problem. However, on the day of the accident, the cables were installed as per the first unapproved routing, potentially reintroducing airspeed indication error (although the TSB were not able to determine if such an error influenced the accident).
The emergency floats remained attached to the helicopter skids. The TSB refer to impact damage but do not state if the system remained capable of functioning. They do say that “there was no indication that the flotation system was activated prior to or at the time of the impact”. The system was manually activated only, with no automatic float deployment system (AFDS).
The aircraft carried a life raft certified to FAA Technical Standard Order (TSO) C70a (rather than the enhanced standard for operating in a hostile environment EASAETSO-2C505, which includes features to aid boarding). It was mounted internally, making successful extraction in this cash scenario unlikely. TSB say:
…all 3 occupants survived the impact, but succumbed to the effects of cold water exposure and drowned before they were rescued. ….the occupants were immediately exposed to cold shock as the helicopter sank in the −0.6 °C water. It has not been determined if the individuals managed to unbuckle their seat belts by themselves [all three were found unbuckled] or if they were helped by one of the other occupants. Considering that neither the master nor the scientist had taken helicopter underwater egress training (HUET), it is possible that it was more difficult for them to exit the helicopter than it would have been for the pilot, who had taken HUET in the past. Therefore, it is possible that the pilot managed to escape more rapidly and inflate the PFD before being incapacitated.
The pilot was wearing a VikingPS4089 survival suit. It has an insulation value of 0.7 clo in still water with no leaks. The passengers were wearing Mustang Survival model MS2175 TC ‘helicopter transport’ suits. This model is not however certified to a recognised standard. It has an insulation value of 0.4 clo in still water with no leaks. All the survival suits were found to contain water, significantly compromising the insulation, due to the zips being partially open. In particular the pilots suit had a ‘split-neck seal’ and a zip that required two hands to close (and in tests could only be done with assistance). This zip was routinely left open to the mid-sternum position by pilots for ventilation. None of the three, had been able to don gloves or hoods. The three occupants wore Switlik HV-35C life jackets, or Personal Flotation Device (PFD), certified to the obsolescent FAA TSO C13d (rather than EASA ETSO-2C504 for hostile environments).
The pilot was found floating face up, and not wearing a PFD. The scientist was found on his side, with the PFD only partially inflated. The master was found face down; the PFD was not inflated.
A maintenance quality issue had been identified where some of these life jackets had had their flotation bladders rolled rather than folded, which would result in poor inflation characteristics. It was not possible for the TSB to determine if any of the occupant’s life jackets were affected by the problem.
The Safety Investigation – Cold Water Survival
The three survivors then found themselves in sub-zero water, with compromised protective equipment. TSB explain that:
There are 4 phases of cold water immersion. The first phase, cold shock, is the primary cause of crew and passenger drowning in helicopters that ditch in cold water. Even with the protection of an immersion suit, the sudden exposure to the cold water causes a gasp reflex, hyperventilation, and involuntary water intake. The gasp reflex and hyperventilation can last from 10 to 120 seconds….In near freezing water, breath-holding time in a well prepared test subject drops dramatically to about 10 to 15 seconds.
It is for this reasons that Emergency Breathing Systems (EBS) are used by some organisations, civil and military.
The second phase…is cold incapacitation. During this phase, the muscles and nerve fibres cool, which decreases their ability to function and leads to limitations fine motor movements and then gross motor movements.In 0 °C water, the decline in physical performance could start within 1 to 2 minutes, and complete incapacitation could occur within 10 to 20 minutes. Without gloves, muscle and nerve cooling would quickly decrease hand dexterity and strength.
The third phase is hypothermia. Normal body core temperature is 37 °C. The clinical threshold for mild hypothermia is 35 °C, with the following classifications: Mild Hypothermia, 35–32 °C; Moderate Hypothermia, 32–28 °C; and Severe Hypothermia, less than 28 °C. An adult human body in normal winter clothing will normally take at least 30 minutes before reaching mild hypothermia in 0 °C water and more than 2 hours before becoming severely hypothermic… The addition of thermal protective clothing will delay the onset and severity of hypothermia.
Circum-rescue collapse is the fourth phase and can occur just before, during, or after rescue/extraction. Symptoms range from physical collapse to fainting, to cardiac arrest and death. Rescue can cause mental relaxation and decreased stress hormone production (e.g., epinephrine), which can lead to a large drop in blood pressure, and as the cold, irritable heart works harder to maintain blood pressure, it can stop.
Significantly, TSB state that “for practical purposes a significant risk of immersion hypothermia” is considered to occur at sea temperatures below 25 °C and so “the risk of immersion hypothermia in North America is nearly universal during most of the year”. However the TSB consider it…
…highly unlikely that the victims’ immersion time was long enough to induce severe hypothermia and cold-induced ventricular fibrillation. However, the victims were definitely immersed long enough to cause considerable, if not complete, cold incapacitation which would have made it impossible for them to maintain their airway above the water line while not wearing a PFD, or while wearing one that was improperly inflated. Based on the sea temperature (−0.6 °C) and conditions (calm), as well as the clothing worn, the core temperature of all victims was predicted to be no lower than 34 °C when recovered; this is considerably higher than the core temperature at which hypothermia would cause ventricular fibrillation (generally <28 °C); therefore, hypothermia per se was not a primary cause of death. It is likely that the occupants were completely submerged during impact and egress since it is probable that the helicopter sank quickly. Complete submersion in ice water would initiate the gasp reflex and decrease breath-holding ability; thus, drowning could have occurred as early as during egress.
This suggests that a Compress Air Emergency Breathing System (CA-EBS) may have been of value (see Extra Resources below).
The Safety Investigation – Alerting / Flight Following
The helicopter was fitted with a fixed Artex Emergency Locator Transmitter (ELT). The TSB note this was:
…designed to transmit a 406-MHz signal for 440 to 520 milliseconds, repeating every 47.5 to 52.5 seconds. However, the first transmission after activation is deliberately delayed for 50 seconds in order to prevent false alarms that can occur during routine ELT maintenance….[but]….this delay may prevent the broadcast of an actual distress signal in a ditching scenario if the aircraft submerges before a signal is emitted.
In this case it was not possible to determine if the ELT activated at impact due to the rapid submergence of the aircraft. Each occupant had a Personal Locator Beacon (PLB). However the type used must be manually activated, something that would have been very unlikely in the cold water with uninsulated hands. The helicopter was equipped with a SkyTrac ISAT-200R satellite tracking system. This had started to replace a obsolescent system during 2013 in CCG / TC ASD operations. At the time of the accident the ship’s Control Display Unit (CDU) needed to be manually set before every flight to ensure the aircraft position was updated every 2 minutes (rather than a less frequent default).
However, the Shipboard Helicopter Information and Procedures Manual had not been updated to reflect SkyTrac, as it was “still in the development phase”. It did not specify who was responsible that action or who should monitor the system while the helicopter was airborne. The ship’s crew did not receive training on the system directly but via the ASD staff carried on-board. On the day the wheelhouse crew were distracted and did not complete the CDU adjustment. Although they spotted that the aircraft position was not as expected, with their limited training they did not appreciate that this indicated the reset had not been done. Furthermore, after several false overdue notifications, the automated e-mail overdue notifications function had been deactivated in July 2013 until these erroneous notifications were eliminated (although crew activated emergency messages remained enabled).
Since the master was on board the helicopter, the chief officer (CO) assumed responsibility for the vessel and its crew, and he was on the bridge supervising the scientific work and standing by for the helicopter. The CO is authorized to act in the master’s absence to make decisions and to take control of the vessel’s movements as required. In addition to the CO, the first officer and his wheelsman and the second officer and his deck crewman were standing by on the bridge while waiting for the helicopter to return. At approximately 1740, the second officer and the deck crewman left the wheelhouse to prepare the flight deck for the helicopter’s arrival when they heard that the ETA was in 10 minutes. The vessel continued its maneuvers.
At 1805, 17 minutes after the helicopter’s ETA and 22 minutes after the helicopter crashed, the wheelhouse crew checked the position of the helicopter on the vessel’s CDU, which displayed the helicopter’s distance at 3.2 nm. This information led the crew to believe that, although the helicopter was late, it would arrive in approximately 3 minutes. The crew did not realize that the helicopter position displayed on the CDU was time stamped at 1741, which meant that it was 24 minutes old. At 1818, once informed that communication with the helicopter had been lost, the CO assumed control of the vessel from the first officer, and ordered and supervised the SAR effort.
Search and Rescue operations therefore commenced operations 35 minutes after impact.
The Safety Investigation – Search and Rescue
The TSB report that:
At 1824, the decision was made to proceed toward the helicopter’s last displayed position. However, due to ice conditions, the vessel could not proceed direct. At 1854, 2 of the 3 occupants were located and found to be floating and unresponsive. They were brought on board the [ship’s Fast Rescue Craft] FRC and were showing signs of drowning. No vital signs were observed. At 1907, the third occupant was located floating, also unresponsive, and was brought on board the FRC showing signs of drowning and no vital signs. Due to the lack of space inside the FRC, no first aid treatment or resuscitation manoeuvres could be attempted. Once brought into the vessel’s hangar, vital signs, except for body temperature, were checked. None of the occupants was showing signs of breathing, and a pulse rate could not be felt. They were all pale and had dilated pupils. CPR was attempted for a few minutes on the pilot, to no avail. He was pronounced dead at 1920, 15 minutes after being brought on board the vessel. Considering that the master and the scientist were showing similar physical conditions, it was felt that attempting CPR would also be unsuccessful. Therefore, no CPR was attempted on the master and the scientist, and both were pronounced dead shortly after their arrival in the hangar.
The Safety Investigation – Data Recorders
The helicopter was not equipped with a flight data recorder (FDR) or a cockpit voice recorder (CVR), nor was it required to be by regulation.
We have previously discussed the value of data recorders:
TC ASD is considered a commercial air carrier but is unusual in being part of the same organisation as the regulator. It holds operating certificates for operations under Canadian Aviation Regulation (CAR) Sub-parts 702 (aerial work), 703 (air taxi) and 704 (commuter). None of those requirements include a need to have a Safety Management System (SMS). TC ASD had however initiated the implementation of an SMS. A regulatory audit by:
…TC in September 2011 resulted in 15 findings: 9 related to flight operations and 6 related to maintenance. The flight operations findings were related to operational control (3), flight and duty times (1), flight crew training records (2), company manuals (2), and flight documentation (1). Of the findings related to operational control, one was described as critical and another as major. The critical finding cited 2 incidents involving CCG helicopters as examples of a lack of operational control.
At the time of the accident in September 2013 the majority remained open and the next audit was not conducted until after the accident.
TSB Findings as to Causes and Contributing Factors
There is a strong probability that while over the open water, the pilot experienced a lack of the visual cues required to judge altitude.
The possibility of pilot distraction could have caused a lapse in the pilot’s concentration, resulting in the loss of altitude and water contact.
None of the 3 occupants was supported in a manner to keep their mouth and nose above the water line. It is likely that they drowned as a result of cold incapacitation before they were rescued.
The life raft was installed inside the helicopter and sank with the aircraft; therefore, it was not available to aid the survivors after the accident.
The training did not bring the vessel’s crew to the required level of competence to set up the flight following system and later interpret the information displayed on the control display unit. This reduced the effectiveness of the flight following system and delayed the initiation of the search and rescue.
There was no aural warning to alert the vessel’s crew immediately that the helicopter was no longer transmitting position reports. Therefore, the initiation of search and rescue was delayed.
Additionally 19 ‘findings as to risk’ and 3 ‘other findings’ are recorded in the TSB report.
Safety Actions
TSB raised no safety recommendations. During the first year since the accident TC AS issued a number of notices. Then:
On 16 September 2014, a team of ASD and CCG personnel completed a review of the 2008 risk assessment related to immersion suits for the rotary wing operations to verify the assumptions and update the document to ensure it remained valid. The recommendations from that risk assessment have resulted in a policy change proposal that will increase the frequency for wearing immersion suits in operations over water. The risk assessment team also recommended an immersion suit trial program to identify better options for flight crew, given advancements in suit technology since the previous procurement of the Viking 4089 in 2011. Following the immersion suit trial, new suits (Survitec 1000-300 or Viking 4043) were provided to flight crew identified in the urgent replacement category.
On 01 April 2015, ASD started to acquire a new fleet of helicopters to replace the BO 105. The new fleet is equipped with automatic float deployment and life rafts that are externally mounted and integral to the flotation system. These new helicopters also have enhanced one-engine-inoperative performance. The new helicopters are equipped with state of the art CVFDR data acquisition flight recorders (cockpit voice recorders and flight data recorders). As well, the new helicopters are equipped with a health and usage monitoring system which can identify premature failures proactively.
A new immersion suit—wearing policy was implemented in April 2015, which significantly increased the requirement to wear suits and the procurement of a new type of immersion suit has begun. The evaluation and selection of emergency breathing apparatus are completed and the procurement will begin in October 2015. New and improved life jackets were obtained for the new helicopter fleet. New personal locator beacons with simpler activation system were obtained for the new helicopter fleet. An Operations Quality Assurance and Control system was implemented as of 01 April 2014.
The CCG also issued notices, held briefings and revised their survival / immersion suit policy.
Two previous accidents are noteworthy as they highlighted survivability issues, and yet significant room for improvement remained in 2013. On 10 May 2000, CCG Bell 212C-GCHG impacted water near Cabot Island, Newfoundland and Labrador, during an underslung load operation killing the pilot (TSB report). The TSB investigation found that although that impact was considered non-survivable, the pilot was neither:
Equipped to survive either a less severe accident or a controlled ditching into the frigid water,
Wearing an immersion suit or a lifejacket, nor
Wearing the supplied shoulder harness.
At that time it was stated that:
TC responded on 02 April 2001, indicating that a working group has been convened to examine the issue of offshore operations and make recommendations. The working group will consider, inter alia, the requirements for the carriage of survival equipment, survival equipment use, and the accessibility of the equipment.
TC ASD then suffered a fatal CCG Bo105 accident in 2005. According to the TSB report, Bo105 C-GGGC:
…was being used for various tasks associated with the upkeep and operation of lighthouse and coastal navigation facilities in the Burin Peninsula area of Newfoundland and Labrador. While returning to Marystown in the late afternoon of 07 December 2005, with one pilot and one passenger on board, the helicopter encountered heavy snow showers and, at about 1628 Newfoundland standard time, the helicopter crashed into the water of Mortier Bay, east of Marystown.
Recovery of Bo105 C-GGGC (Credit: TSB via ASN)
Both the pilot and the passenger survived the water impact and escaped from the helicopter. However, the pilot perished from hypothermia, and the passenger drowned.
The TSB findings as to causes and contributing factors were as follows:
The helicopter encountered a heavy snow shower and, while attempting to fly out of the snow, the pilot likely became disoriented.
The pilot lost control of the helicopter when the tail broke off after contacting the water during a rapid flare.
The survival equipment fitted to the helicopter sank with it, and was not available to aid the survivors after the accident.
The occupants of the helicopter were not wearing sufficient personal survival equipment to enhance their potential survival in the frigid water.
At the time it was stated that:
TC ASD and the Canadian Coast Guard (CCG) have established a Helicopter Operations Safety Working Group to review safety equipment, training, and procedures, and to make recommendations for improvements. TC ASD is in the process of implementing a Safety Management System, adding the position of an assistant chief pilot helicopter position and a flight operation quality assurance position all intended to improve, where necessary, existing communication, documentation, and risk assessment practices.
Extra Resources
If you found this article of interest you may also enjoy:
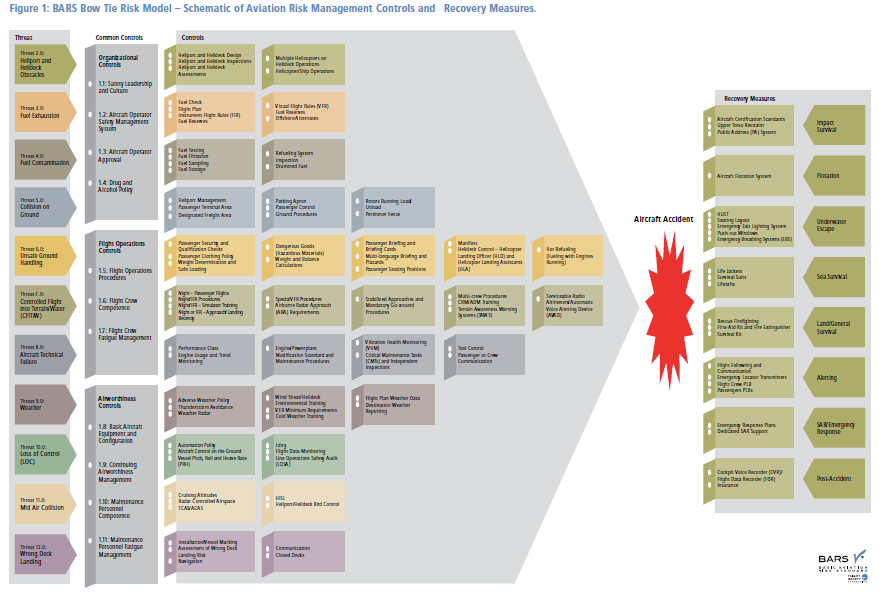
To better understand the recovery measures of an offshore helicopter accident we recommend the Flight Safety Foundation (FSF) Basic Aviation Risk Standard for Offshore Helicopter Operations (BARSOHO), launched in May 2015. It is based on their of their award winning Basic Aviation Risk Standard, used in the mining industry, but tailored to offshore operations. The standard is orientated around a risk bow-tie, contains a number of common and specific threat controls as well as recovery measures (grouped in distinct categories, for survival after an offshore accident): The whole BARSOHO standard is freely available, with an accompanying implementation guide. UPDATE 1 February 2017: BARSOHO Version 3, fully aligned with the HeliOffshore Safety Performance Model, is now issued and available.
Previous studies on and accident investigations into helicopter ditchings and water impact events have highlighted inadequacies in the existing certification specifications (CS-27, CS-29) and in the rules governing offshore operations.
In particular, it has been established that in an otherwise survivable water impact, most fatalities occurred as a result of drowning because the occupants were unable either to rapidly escape from a capsized and flooded cabin, or to survive in the sea for sufficient time until rescue.
Furthermore, the testing environment in which helicopters are type-certified for ditching bears little resemblance to the sea conditions experienced in operation. In order to thoroughly address these and other ditching-related issues, and due to the nature of ditching-related hazards, this rulemaking task (RMT.0120 (27&29.008)) has taken a holistic approach to the problem, which crosses traditional airworthiness/operational boundaries.
A detailed risk assessment has been undertaken that reflects both certification and operational experience and builds upon data extracted from accident reports and previous studies. The specific objective of this NPA, however, is to propose changes to CS-27 and CS-29…
Retroactive rules are to be considered in a second phase of this RMT.
…the primary change proposed aims to establish a new ditching certification methodology by which a target probability of capsize following a ditching can be determined based on the level of capsize mitigation applied to the design.
UPDATE 22 June 2017: A Canadian Parliament Committee issued a report to the federal government with 17 recommendations, aimed at enhancing aviation safety in Canada. The Standing Committee on Transport, Infrastructure and Communities heard 47 witnesses and received 11 briefs, leading to a report with 17 safety recommendations. These included:
That the implementation of a Safety Management System becomes mandatory for all commercial operators, including the air taxi sector.
That Transport Canada:
a. establish targets to ensure more on-site safety inspections versus Safety Management System audits;
b. use poor results from Safety Management System audits (including whistleblower input) as a ‘flag’ for prioritizing on-site inspections;
c. Review whistleblower policies to ensure adequate protection for people who raise safety issues to foster open, transparent and timely disclosure of safety concerns.
That the government make sure that Safety Management Systems are accompanied by an effective, properly financed, adequately staffed system of regulatory oversight: monitoring, surveillance and enforcement supported by sufficient, appropriately trained staff.
That Transport Canada review all training processes and training materials for civil aviation inspectors to ensure they have the resources to perform their duties effectively.
UPDATE 14 September 2020: Survivor evidence, given virtually, at the 2013 Sumburgh helicopter accident Fatal Accident Inquiry this month strongly reinforced the idea that realistic practical HUET training is crucial to survival.
SAR Consultancy: Procurement, Tenders, Contacts and In-Service Assurance and Aviation Advice
In September 2017 one European Coast Guard selected Aerossurance to be their new aviation consultants after a competitive tender with 7 bidders. In July 2018 Aerossurance started work supporting a second European Coast Guard with a procurement project. The Aerossurance team is and has supported humanitarian aid agencies, air ambulance charities, military air arms, environmental agencies and blue chip energy companies on other emergency service and special mission aviation projects around the world.
Aerossurance has extensive helicopter safety, flight ops, airworthiness, SAR, survivability and accident analysis experience, and is pleased to be part of the BARSOHO development team. For practical aviation advice you can trust, contact us at: enquiries@aerossurance.com







 The whole BARSOHO standard is freely available, with an accompanying implementation guide. UPDATE 1 February 2017: BARSOHO Version 3, fully aligned with the HeliOffshore Safety Performance Model, is now issued and available.
The whole BARSOHO standard is freely available, with an accompanying implementation guide. UPDATE 1 February 2017: BARSOHO Version 3, fully aligned with the HeliOffshore Safety Performance Model, is now issued and available.