Wreckage of Puerto Rico Air National Guard Lockheed WC-130H, 65-0968 (Credit: USAF)
All nine persons on board were killed. The last moments of the flight were captured on dramatic CCTV footage:
History of the Accident Flight
The aircraft was en route to Davis-Monthan Air Force Base, Arizona (commonly known as ‘the boneyard‘) to be retired. It had however been at been at Savannah/Hilton Head since 9 April 2018 for scheduled fuel cell maintenance which could not be done in Puerto Rico due the unit’s hangar being damaged by Hurricane Maria in September 2017. Unscheduled work on engine no 1 had also been conducted (see below).
The aircraft commander, Mishap Pilot 1 (MP1), had 18 years or service, was an instructor pilot and was “regarded by many as the best pilot in the unit” according to the US Air Force (USAF) Accident Investigation Board (AIB) report. The AIB say that the crew performed a rolling take off that morning, and so were less able to check for correct engine performance.
During takeoff roll, engine one revolutions per minute (RPM) fluctuated and did not provide normal RPM when MP1 advanced the throttle lever into the flight range for takeoff. At approximately eight seconds prior to aircraft rotation, the engine one RPM and torque began to significantly decay and dropped to 65% RPM and 1,971 in-lbs torque at the moment of rotation. [The Mishap Flight Engineer] MFE failed to execute his learned and practiced visual scan patterns to recognize the loss of power and call for a reject of the takeoff.
FDR Data Replay at Rotation for Puerto Rico Air National Guard Lockheed WC-130H, 65-0968 (Credit: USAF)
The fluctuation on roll and significant performance decay went unrecognized by the MC [Mission Crew] until rotation, when MP1 commented on aircraft control challenges and the MA [Mishap Aircraft] veered left and nearly departed the runway into the grass before it achieved flight.
As the landing gear, was retracted the crew identified the engine no 1 malfunction and MP1 called for engine shutdown. However, the investigators say the crew…
…failed to complete the Takeoff Continued After Engine Failure procedure, the Engine Shutdown procedure, and the After Takeoff checklist as directed by the Flight Manual, and the MA’s flaps remained at 50 percent. Additionally, MP1 banked left into the inoperative engine, continued to climb, and varied left and right rudder inputs.
FDR Data Replay Just Prior to Loss of Control of Puerto Rico ANG Lockheed WC-130H, 65-0968 (Credit: USAF)
At an altitude of approximately 900 feet mean sea level and 131 knots indicated air speed, MP1 input over nine degrees of left rudder, the MA skidded left, the left wing stalled, and the MA departed controlled flight and impacted the terrain on Georgia State Highway 21.
Previous Flight, Maintenance Troubleshooting and Engine Failure Analysis
On the ferry flight from Puerto Rico to Savannah [on 9 April 2018], the flight crew…experienced an RPM issue with engine one, and reported the incident for troubleshooting and repair. The crew explained in the write up that engine one’s RPM dropped to 96% when the crew switched the synchrophaser master switch off during final approach (a step taken as the aircraft is on approach for landing). However, as explained in the write up, the ferry crew believed the RPM corrected to normal parameters when they switched on the propeller governor control to mechanical governing. Upon landing in Savannah, the ferry flight crew chief notified [their maintenance unit] in Puerto Rico of the discrepancy in engine RPMs, and the 165 AW shop supervisor loaded the write up into the IMDS/G081 system, which also informed the 156 AW that the MA had an engine discrepancy.
On 23 April 2018, after the fuel tank maintenance was complete, two propulsion specialists from Puerto Rico, Mishap Maintainer 1 (MM1) and Mishap Maintainer 2 (MM2), arrived in Savannah to perform the necessary engine maintenance. On the next day, MM1 and MM2, with the assistance of two crew chiefs, performed two separate engine runs.
According to the maintenance T.O. [the Technical Order being the USAF equivalent of an aircraft Maintenance Manual], the first step when conducting a C-130 engine maintenance run to troubleshoot an engine RPM discrepancy is to connect a precision tachometer (commonly referred to as an “Accu-Tach”). Often, propulsion specialists will travel with a precision tachometer from their home unit, if one is available. MM1 and MM2 were unable to do so because the 156 AW only had one working precision tachometer and when MM1 and MM2 departed Puerto Rico for Savannah, it was away from station traveling with T/N 65-0984.213
Precision Tachometer Kit (Credit: USAF)
At some point during the engine runs (possibly after the first engine run), the Mishap Maintainers did check out a precision tachometer from the [local unit’s tool store].
This was however a different variant than they were used to.
As a result, the Mishap Maintainers were unable to get this version to connect to the MA because the plugs were a different configuration. The maintainers were unaware the precision tachometer supplied…contained an adapter plug that allowed the device to plug into the MA.
A Precision Tachometer In Use (Credit: USAF)
The first step of the T.O. required connecting the precision tachometer and, thus, the Mishap Maintainers should not have continued the engine runs, as they had not completed the first step. However, without using a precision tachometer, the Mishap Maintainers proceeded with the engine runs.
During the first engine run, MM1 and MM2 attempted to duplicate the discrepancy and solution noted by the 9 April flight crew. They were able to duplicate the discrepancy, but not the solution reported by the flight crew. Regardless of the engine governing selection, neither MM1 nor MM2 observed the engine achieve an RPM greater than 96%. The MA’s Digital Flight Data Recorder (DFDR) confirms this observation. The first troubleshooting method MM1 and MM2 took was to check the RPM tachometer gauge associated with the malfunctioning engine…This is done by removing the gauge and replacing it with a new one…
According to the TO, this should only happen after the engine is shutdown to avoid damaging the gauge. However, the maintainers hot swapped the engine no 1 tachometer gauge with the engine no 2 gauge during the engine run. The replaced gauge still indicated 96% RPM on engine no 1. They then shut the engine down to adjust the engine no 1 valve housing. MM2 made a 12-click clockwise adjustment up with the aim of increasing the engine RPM up to 99%.
According to post-mishap interviews, during a second maintenance engine run, the Mishap Maintainers observed engine one produce 99% RPM. However, this is not supported by the DFDR, which indicates engine one never reached sustained RPM above 96.8% and had significant oscillations between 95% and 98%.
Even if the engine had achieved 99%, the engine would have needed to reach 100% to complete the task (the T.O. requires a range of 99.8% to 100.02% RPM to be verified on the precision tachometer).
The final minutes of the second engine run were captured on the MA’s CVR. This is because the CVR in a C-130 records on a 30-minute loop. On this recording, MM1 stated his intention for the maintenance team to give the valve housing an additional four-click adjustment up and then call the maintenance complete without performing another engine run.
However, after the conclusion of the [second] engine run, MM1 and MM2 discussed the need for an additional adjustment. They concluded that an additional four clicks would get the engine RPM to 100%, but doing so would require an additional engine run… MM1 and MM2 felt that 99% was acceptable and that no additional adjustments were necessary. The DFDR confirms the Mishap Maintainers did not attempt a third engine run.
None of the Mishap Maintainers understood the significance of the MA’s engine discrepancy or the importance of using a precision tachometer and considered the discrepancy somewhat common. MM1 signed off the engine discrepancy as repaired in accordance with the T.O.
The investigators comment that:
In addition, the two mishap crew chiefs did not act as members of a cohesive team with the mishap propulsion maintainers. They seemed to be oblivious to any and all maintenance actions on the MA and specifically engine one. They should have participated as part of the team and, as such, could have voiced a concern over not following T.O. guidance and/or provided an additional scan on the engine one RPM gauge.
Additionally:
…the Propulsion Shop Lead did not know the difference between back shop manuals and on-aircraft manuals [and] neither MM1 nor MM2 realized there were troubleshooting guides in the on-aircraft manuals and relied on a back-shop manual.
The investigators believe the the most likely reason for the engine malfunction was a failure its valve housing assembly, but its destruction in the accident precluded identifying a specific failure mode. When the engine speed dropped below 94%, the engines bleed valves would then have opened, as designed to prevent a compressor stall, further reducing power.
Organisational Culture
The investigators report that:
During the course of the investigation, several recurring factors emerged with regard to the health and low morale of the 156 AW. These factors were captured in statements, testimony, and discussions during the visit and tour of the Muñiz Air National Guard Base. While several of the items are common in any organization (manning challenges for example), the number, the repetition, and the combination of all the factors, highlighted up and down the chain of command at the 156 AW, may be indicative of a climate and culture of complacency.
They speculate that:
This climate could have shaped the attitudes and actions of the Mishap Maintainers to disregard T.O. guidance, the team’s attitude that 99% RPM was good enough as the “aircraft is going to the boneyard anyway” (as captured on the CVR), and not realizing the significance of T.O. violations. It may have also been a factor with the MC’s apparent complacency during takeoff roll, failure to brief emergency actions adequately, and failure to monitor the MA’s performance, specifically the performance of engine one after maintenance work for a recent discrepancy.
Many of the those interviewed commented on the low morale of the Wing. The factors cited as leading to low morale include:
Having the oldest C-130’s in the USAF and the belief the 156 AW is an afterthought in Air Force planning.
156 AW aircraft were not combat-rated and so members do not see themselves as participants in the “Total Force” with no direct connection to a specific mission.
Difficulty with obtaining spare parts, leading to long repair times and lower mission capable rates for their aircraft.
Manning challenges in a vicious circle of low morale causing manpower shortfalls as people choose to leave the unit leading to higher workload and lower morale.
Human Factors Analysis
The investigators opine that:
The Mishap Maintainers (MM1, MM2, MM3, and MM4) showed a distinct lack of motivation to ensure engine one was operationally ready for flight.
They note that several violations of procedures occurred during the engine maintenance. The investigators comment that the flight crew did not correctly follow specific checklists and procedures during the take off.
Had the MC followed the appropriate checklists and procedures, they could have easily flown out of the emergency and not placed the MA in such a dangerous flight position and vulnerable to an errant left rudder input.
They also opine the MFE’s visual scan pattern broke down, resulting in a failure to identify the anomalous engine performance promptly. They also discuss a lack of assertiveness and authority gradient in the cockpit:
As the MA turned into the feathered engine, MP2 verbalized the hazard in time to correct the situation with his call, “Turning into number one, crew.” MP1 never acknowledges the call of MP2. his call by MP2 appears to be an attempt by MP2 to state critical information, i.e., that the MA should not be turning towards the inoperative outboard engine. However, MP2 who performed well in the simulator during flight training on this type of emergency, said nothing further, did not run any of the proper checklists or procedures, and did not suggest or direct any solutions, e.g., keeping the nose low, applying right rudder, etc.
They also opine MP1 had become fixated on returning to land:
…evident by his repeated use of the phrase “Coming Back” five times over 25 to 30 seconds without giving any other meaningful direction to the MC other than “Brace” just prior to impact.
They state there was confusion about the symptoms the crew were experiencing. Finally, the aircraft was over-controlled.
In the last minute of the mishap flight, MP1 applied and varied both left and right rudder pressure multiple times, then reversed and sustained the pressure to the left rudder. This left rudder input led to an increasing left skid of the MA. This final rudder input coincides with the MA stall and subsequent left roll when the MA departed controlled flight. If not for this left rudder input, the MA would not have departed controlled flight.
AIB President’s Conclusions
After a comprehensive investigation into this mishap, I find, by a preponderance of the evidence, the cause of the mishap was MP1’s improper application of left rudder, which resulted in a subsequent skid below three-engine minimum controllable airspeed, a left-wing stall, and the MA’s departure from controlled flight.
Additionally, I find, by a preponderance of the evidence, the MC’s failure to adequately prepare for emergency actions, the MC’s failure to reject the takeoff, the MC’s failure to properly execute appropriate after takeoff and engine shutdown checklists and procedures, and the Mishap Maintainers’ failure to properly diagnose and repair engine number one substantially contributed to the mishap.
Our Observation
This format of conclusion lead to the unfortunate prevalence of ‘pilot error’ being used as a simplistic label in press reports. It is also noticeable that the cultural aspects discussed in the report were not acknowledged in the conclusion.
The intergranular radial crack in blade four, which ultimately was the root cause of this catastrophic mishap, developed and matured from corrosion pitting and (intergranular cracking) that was not removed during the last blade overhaul [in 2011],” the investigation states.
For instance, the investigation found no evidence that the corrosion-preventing permatreat coating or epoxy primer was ever put onto the blade that incited the accident, even though such treatments were required by the Navy at the time.
Investigators also discovered that eddy current inspections, which use electromagnetic waves to detect anomalies under a metal surface, were also not performed at WR-ALC during 2011, even though they were a compulsory part of the Navy process.”
“We have commissioned an independent review team made up of experts from the Navy, Marine Corps the Air Force and industry to look at the blade overhaul process, to revamp that process, to ensure that we have the proper procedures, the latest technology, the right technical manuals and the right training,” Brig. Gen. John Kubinec, the current commander of WR-ALC, said in a recent interview.
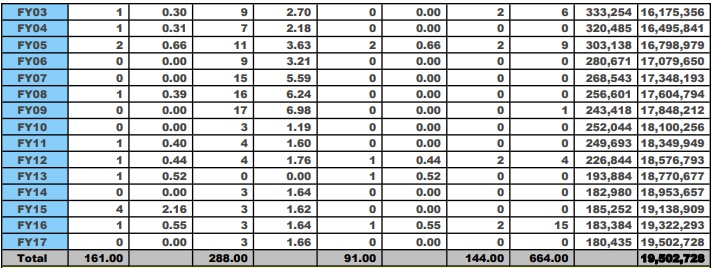
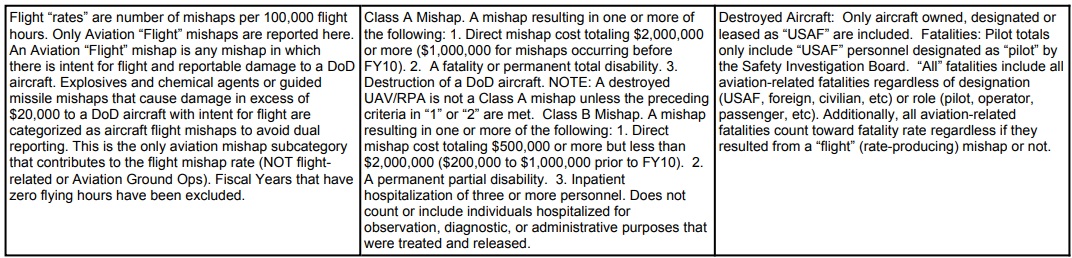
We note that 5 year data is worse than the 10 year data.
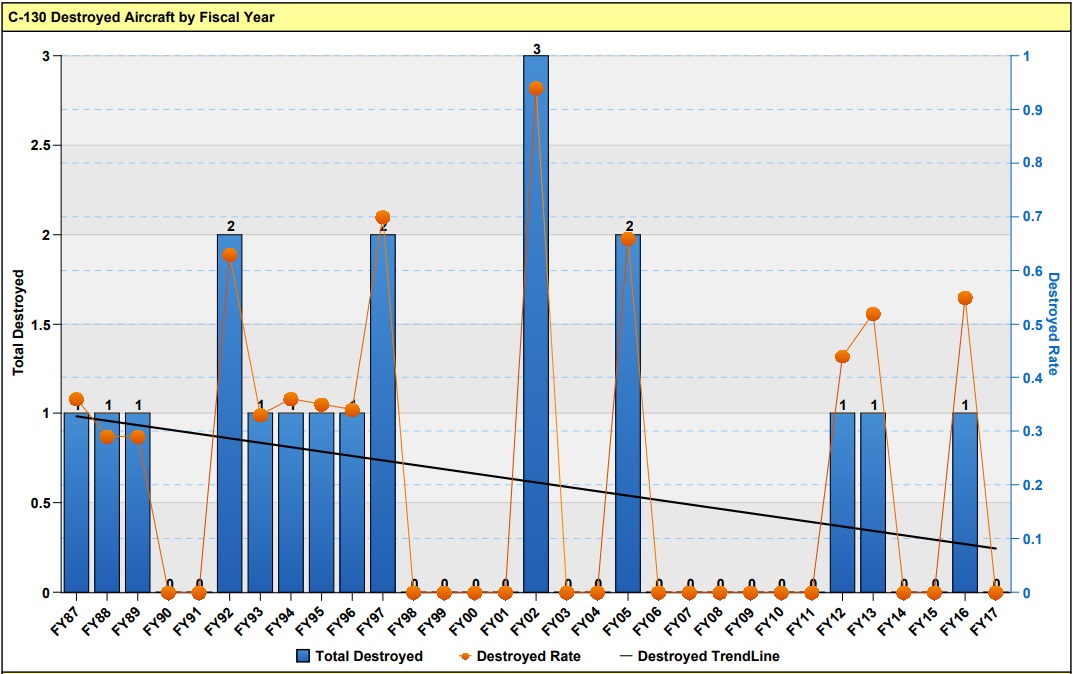
The trend of destroyed aircraft has decreased year on year, though as the tabulation above shows, annual usage has fallen.
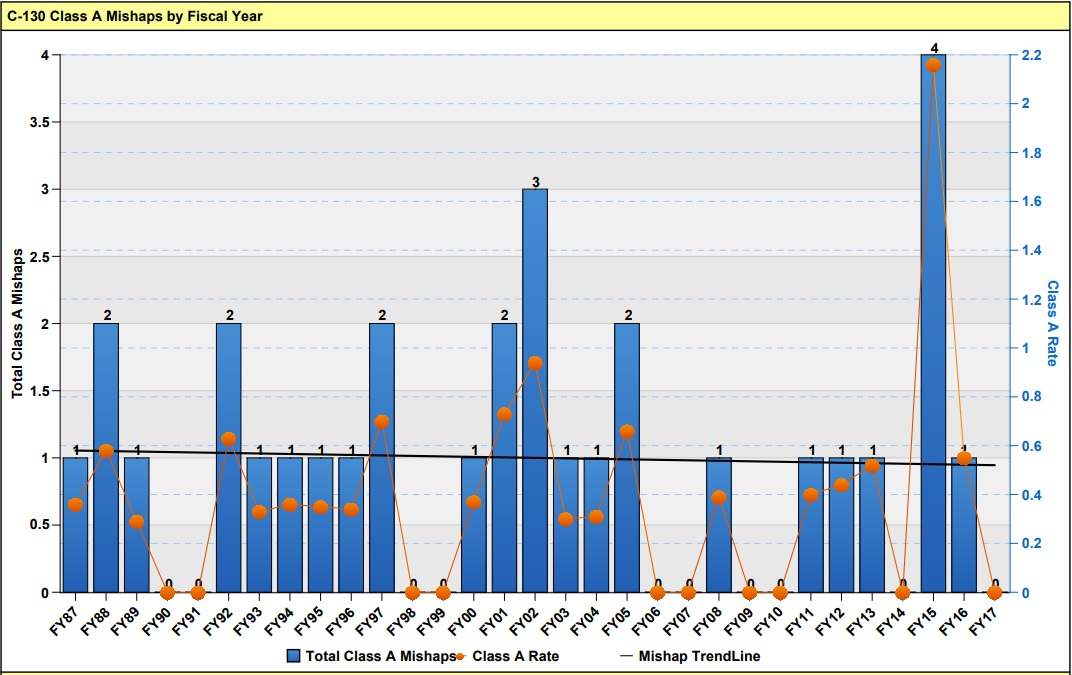
The rate of Cat A mishaps is however static:
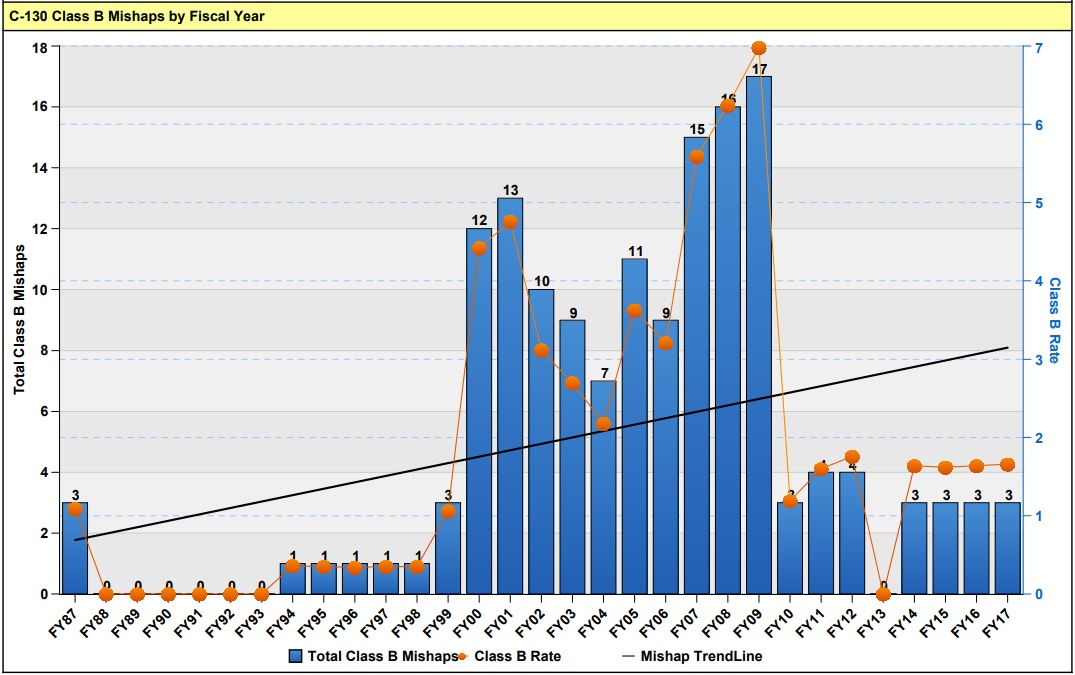
And the rate of Cat B mishaps has risen dramatically.
UPDATE 5 February 2019: The Government Accountability Office (GAO) issue a report, ‘Strategy Needed to Improve Retention of Experienced Air Force Aircraft Maintainers’, which says while the USAF reduced the overall gap between the actual and authorised levels of maintainer staff levels from 4,016 in fiscal year 2015, to 745 in fiscal year 2017, in seven of the last eight fiscal years the USAF had staffing gaps of more-experienced maintainers. These are the people needed to train new maintainers. By hiring more novice maintainers the USAF have not addressed the experience gap. The USAF has a round 100,000 maintainers (including Reserves). They also note that “the Air National Guard has had consistent aircraft maintainer staffing gaps from fiscal years 2010 through 2017— ranging from 84 percent to 89 percent of authorized levels filled”.
Safety Resources
You may also be interested in these Aerossurance articles:
B1900D Emergency Landing: Maintenance Standards & Practices The TSB report posses many questions on the management and oversight of aircraft maintenance, competency and maintenance standards & practices after this serious incident. We look at opportunities for forward thinking MROs to improve their maintenance standards and practices.
UPDATE 30 March 2019: Contaminated Oxygen on ‘Air Force One’ Poor standards at a Boeing maintenance facility resulted in contamination of two oxygen systems on a USAF Presidential VC-25 (B747).
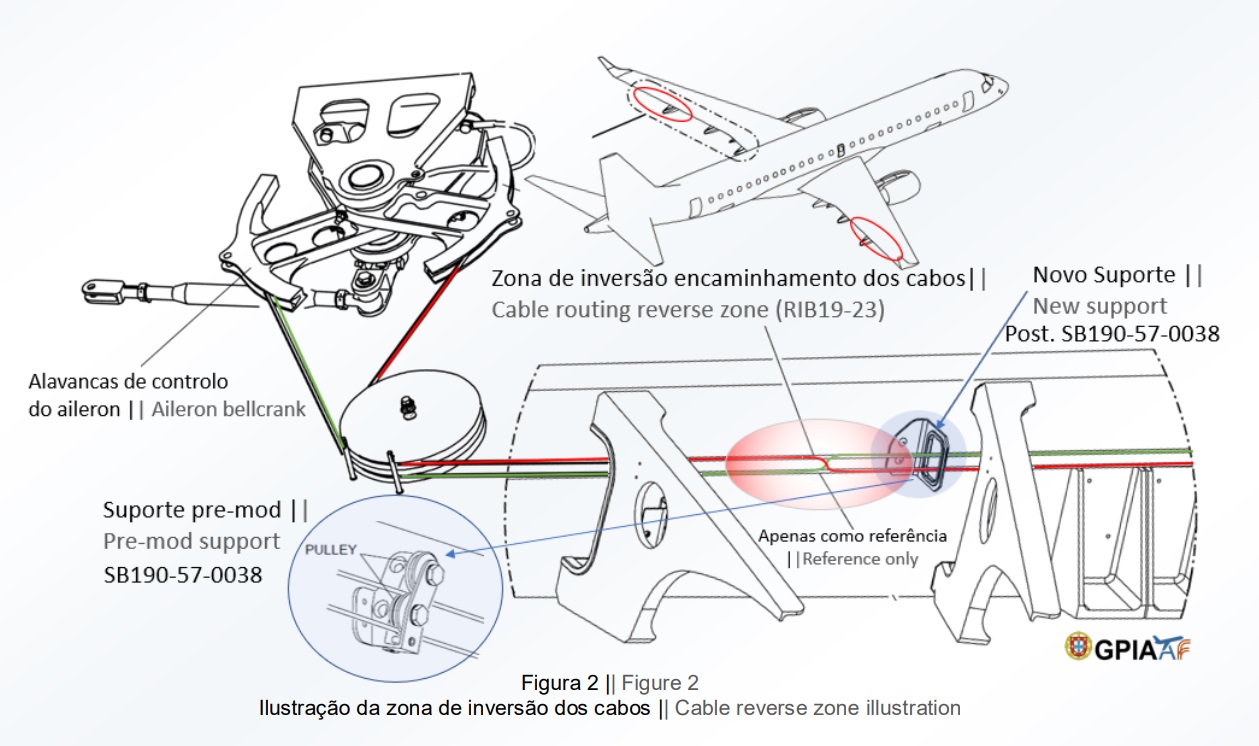
UPDATE 31 May 2019: The Portuguese accident investigation agency, GPIAAF, issued a safety investigation update on a serious in-flight loss of control incident involving Air AstanaEmbraerERJ-190P4-KCJ that occurred on 11 November 2018. The aircraft was landed safely after considerable difficulty, so much so the crew had debated ditching offshore. GPIAAF conformed that incorrect ailerons control cable system installation had occurred in both wings during a maintenance check conducted in Portugal.
Misrigged Flying Control Cable, Air Astana Embraer EJ-190 P4-KCJ (Credit: GPIAFF)
GPIAFF note that: “By introducing the modification iaw Service Bulletin 190-57-0038 during the maintenance activities, there was no longer the cable routing and separation around rib 21, making it harder to understand the maintenance instructions, with recognized opportunities for improvement in the maintenance actions interpretation”. They also comment that: “The message “FLT CTRL NO DISPATCH” was generated during the maintenance activities, which in turn originated additional troubleshooting activities by the maintenance service provider, supported by the aircraft manufacturer. These activities, which lasted for 11 days, did not identify the ailerons’ cables reversal, nor was this correlated to the “FLT CTRL NO DISPATCH” message.”
GPIAFF comment “deviations to the internal procedures” occurred within the maintenance organisation that “led to the error not being detected in the various safety barriers designed” in the process. They also note that the error ” was not identified in the aircraft operational checks (flight controls check) by the operator’s crew.”
UPDATE 12 October 2019: ATR72 VH-FVR Missed Damage: Maintenance LessonsUnclear communications, shift handover & roles and responsibilities, complacency about fatigue and failure to use access equipment all feature in this serious incident.
Aerossurance has extensive air safety, operations, airworthiness, human factors, aviation regulation and safety analysis experience. For practical aviation advice you can trust, contact us at: enquiries@aerossurance.com