Fatal Gulf of Mexico Bell 407 Offshore Take Off Accident: Safety, Helideck & SAR / Emergency Response Questions (RLC N595RL, Walters/IOC WD-106 Installation) – Updated After NTSB Final Report Issued 16 Jan 2025
In 29 December 2022 Bell 407 N595RL of Rotorcraft Leasing (RLC) crashed on take off from the West Delta 106 (WD106) offshore installation in the Gulf of Mexico (GOM). The pilot and 3 passengers died.

On Friday 13 January 2023, the US National Transportation Safety Board (NTSB) issued their preliminary report into this offshore helicopter accident. UPDATE 22 January 2025: The NTSB issued their final report on 16 January 2025, prior to the renaming of the GOM, and we have updated this article.
The Pilot
The NTSB final report reveals the pilot was hired by RLC on 12 September 2022, just 3.5 months before the accident. His resume reported the following experience, including working for 5 onshore operators (the S-60 time should be S-70/H-60):
On 28 September 2022, the pilot completed RLC’s initial ground and flight training (which included 16.8 flying hours, 7 offshore), and became a pilot-in-command (PIC) in the Bell 407 helicopter. RLC evaluated the pilot as satisfactory for the ‘Dynamic Rollover (Oral)’ and ‘Pinnacles or Platform’ requirements.
The pilot’s total flight experience in helicopters, including the 155.8 flight hours flown with RLC, was 1,667.8 hours, of which 1,343.8 hours were flown as PIC at the time of the accident. The pilot had operated to and from WD106 a total of 23 times (GOM pilots are frequently assigned to contracts with specific customers serving a small number of installations).
The pilot was on a 14 day on, 14 day off roster. He had been in Brazil during his most recent time off and travelled back on the day before the accident. That would involve a 9:20 hour international flight, a 1:50 hour domestic flight, plus a drive of c 2:40 hours. The NTSB did not determine their exact schedule. Based on current flight options this journey either involved leaving late on 27th with an overnight international flight and arriving early afternoon the day before the accident or worse, arriving after midnight on the day of the accident.
The lead pilot stated that the pilot arrived for work at 05:30 on the day of the accident.
The Accident Flight
The helicopter departed South Lafourche Leonard Miller Jr. Airport (KGAO), Galliano, Louisiana with 4 passengers for WD106 on a VFR flight, 51.6 nm to the SE, at 07:48 Local Time. The outbound flight appears to have been uneventful.

WD106 is owned by Houston based Walter Oil & Gas Corporation, and was constructed in 1994. On its SE corner WD106 has a 24×24 ft square helideck, which gives a 7.3 m D-value. The B407 has a 13 m D-value so this is a small, 0.56D, sub-D deck. The RLC Ops Manuals treats such decks as “a restricted category helideck” and states that “the pilot may have to reduce load to operate safely”.
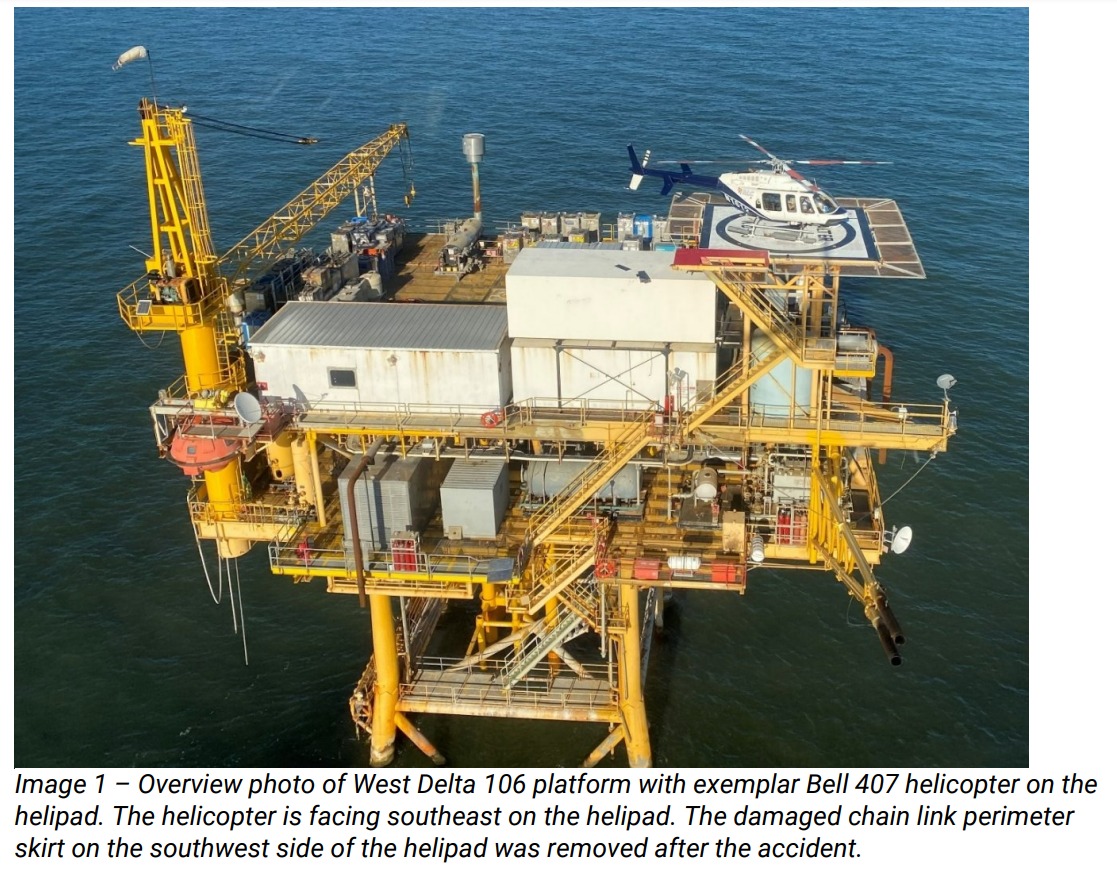
The WD106 Touch Down / Position Marker (TDPM aka Aiming Circle) is 10 ft diameter according to the NTSB, but as evident in images and deck drawings its actually 20 ft diameter.
The NTSB report the deck, which was at an elevation of 100 ft, had recently been repainted and the stairwell painted red.
 It had a perimeter safety net (referred to by NTSB as a ‘skirt’) made of ‘chain-link’ and was marked with 8 perimeter lights (see Figure 3a below), each 8 in (20 cm) tall, rather than the current local standard of 6 in. NTSB claim this was not a factor in this accident (though see our observations below). Some current standards on decks of D<16 would limit these lights to just 5 cm (2 in).
It had a perimeter safety net (referred to by NTSB as a ‘skirt’) made of ‘chain-link’ and was marked with 8 perimeter lights (see Figure 3a below), each 8 in (20 cm) tall, rather than the current local standard of 6 in. NTSB claim this was not a factor in this accident (though see our observations below). Some current standards on decks of D<16 would limit these lights to just 5 cm (2 in).
The helicopter landed at 08:25 positioned on the helideck facing SE. The 4 passengers disembarked and 3 returning passengers, employed by Island Operating Company, who operate WD160 for Walters, boarded shortly after, having had a handover discussion with the incoming personnel below decks. The pilot remained in the rotors running helicopter.
The NTSB state that:
There were no eyewitnesses or surveillance video of the helicopter’s departure from the WD106 helipad; however, there were several individuals who reported hearing the helicopter operating while on the helipad.
Although, the NTSB don’t comment, this lack of witnesses is because the helideck was being operated without a Helideck Landing Officer (HLO) & Helideck Assistants (HDAs) and therefore without immediate fire & rescue cover. This sub-optimal practice is normal on small GOM installations.
These individuals noted that the helicopter’s engine continued to run after it landed on the helipad, and that they heard the engine noise increase for takeoff and then the sound of items hitting the platform.
They immediately went outside and saw the helicopter fuselage floating inverted in the water with the tail boom separated but adjacent to the fuselage. The landing skids were separated from the fuselage and the emergency skid floats were inflated.
Emergency Response
In the preliminary report it was stated that:
Several individuals on the platform then boarded and launched the platform’s emergency escape [freefall enclosed lifeboat] capsule, but the helicopter fuselage sunk before they could render assistance to the four occupants who remained inside the fuselage.
In the final report it was revealed that apparently…
…due to concerns about debris in the water, the survival craft did not reach the helicopter before it sank.
It appears the installation had no Fast Rescue Craft, hence deployment of the installation’s covered lifeboat, an unsuitable craft for attempting a rescue.
The US Coast Guard (USCG) were notified but curiously, despite the NTSB reporting the installation’s crew being aware the helicopter crashed alongside and early social media posts confirming the USCG were aware this was a take off accident, the USCG “searched approximately 180 square miles for 8 hours”.
 It was announced on 4 January 2023 that the bodies had been recovered.
It was announced on 4 January 2023 that the bodies had been recovered.
The Safety Investigation: Installation Damage
NTSB report that:
Examination of the helipad revealed the red paint of the stairwell was gouged and scratched near the southwest end, nearest the skirted area.
The skirt near the stairwell was damaged with metal posts bent and broken and the skirt wire damaged and torn.
One perimeter light, on the southwest corner separated from the helipad and was not recovered. An adjacent perimeter light, located at the center of the west edge of the helipad, was damaged and separated from the helipad. See Figure 7 above.
The light’s blue glass globe was shattered, and shards were found on the deck below the helipad. The remaining perimeter lights appeared undamaged.

 There were two areas of the landing pad surface with gouges in the paint. One area was located on the western area of the aiming circle and consisted of 3 linear gouges and 2 circular gouges into the paint. The other area consisted of 9 linear gouges in the paint.
There were two areas of the landing pad surface with gouges in the paint. One area was located on the western area of the aiming circle and consisted of 3 linear gouges and 2 circular gouges into the paint. The other area consisted of 9 linear gouges in the paint.


Further examination of the platform revealed composite debris scattered throughout multiple decks below the helipad. Most of the scattered debris was consistent with the materials used to construct the main rotor blades. A six-foot-long portion of a main rotor blade came to rest on a metal handrail located on the deck below the helipad [see Image 2b above].
Close examination of imagery released by the USCG suggests the main rotor blade debris was two decks below the helideck. Thee are also significant infringements in the 5:1 falling gradient of the helideck.

The handrail exhibited a downward bend near the location of the main rotor blade. Three pieces of lead weight, consistent with blade weights, and multiple pieces of dark tinted acrylic, consistent with the cockpit overhead windows from the helicopter, were found on the same platform deck as the main rotor blade. The acrylic shards exhibited red paint transfer consistent in color with the red paint of the stairwell.
The upper hydraulic servo cover, normally located above the cockpit, also exhibited the same red paint transfer [see Image 3b above].
The NTSB don’t comment further but it is noticeable that the upper portion of the helicopter struck the stairwell.
Fragments of tail rotor blades were found on the deck below the helipad.
There is no comment on what the tail rotor may have struck.
The Safety Investigation: Wreckage
On 2 January 2023 was the submerged wreckage was located and salvage commenced.

No pre-accident mechanical or system defects were identified. The Engine Control Unit (ECU) was sent to the NTSB Vehicle Recorder Laboratory for data extraction. This confirmed that the engine was functioning normally up until the main rotor blades impacted the helideck.
The Safety Investigation: Recorded Data & Accident Timeline
The Flight Safety Foundation (FSF) Basic Aviation Risk Standard for Offshore Helicopter Operations (BARSOHO) introduced a requirement in 2015 for single-engine helicopters contracted to the BARSOHO standard to have either a:
(1) Cockpit voice and or image recording capability designed to be crash-resistant or;
(2) Flight data recording capability designed to be crash-resistant, adequate for flightpath reconstruction.
The intent was to standardise technology that had been developed over the previous 10 years and thus provide greater occurrence data for single engine, often single pilot helicopters not required to have crash-protected CVRs and FDRs. In this context ‘crash-resistant’, rather than ‘crash-protected’ meant…
…the ability of the recorded data to survive a more limited level of impact, fire and submission in water following an accident. It is accepted that in some extreme cases this data will not survive but the intent is that in the majority of helicopter accidents data should be recoverable.
RLC had fitted an Appareo Vision 1000 cockpit image and data recorder, but in their preliminary report the NTSB noted that it…
…was not found at the platform or in the recovered wreckage; however, there was extensive fuselage damage in the area that the cockpit image recorder is normally mounted.

The recorder was subsequently recovered by divers and data successfully extracted.
A review of the helicopter’s in-cockpit video camera revealed that the pilot did not land the helicopter in the center of the helideck during the landing that preceded the accident takeoff.

Additionally, the pilot did not reposition the helicopter before the accident takeoff.
This video and trials / measurements taken by investigators during a trial, using an exemplar helicopter on contract to BSEE, indicates the aft portion of the right skid would have been adjacent to a helideck perimeter light. Figure 18 below shows the B407’s orientation as concluded during the trial and the skid’s proximity to the crucial perimeter light.

RLC provided NTSB with archived Vision 1000 videos for 27 of the pilot’s previous flights. Just two takeoffs showed a pause with the helicopter established in a 3-5 ft hover, as required by RLC policy. The others revealed a continuous ascent and departure from the helideck.
Examination of the helideck revealed impact gouges in the helideck surface that matched the bolt head pattern of the helicopter’s right skid tube.

These gouges likely were created when the helicopter was in a steep right bank angle. The location of the impact gouges in the helideck surface further supports that the aft portion of the right skid tube was in contact with the helideck perimeter light at takeoff. The perimeter light housing, whose attachment hardware to the helideck was not frangible, was found significantly deformed. Based on the physical and video evidence, the helideck perimeter light became the pivot point for a dynamic rollover to occur during takeoff.
NTSB concluded that at about 08:31, the helicopter was on the helideck positioned aft of the optimum position but with the ‘south’ helideck light visible in the Vision 1000 imagery.
At 0832:18, the pilot began to advance the engine throttle for takeoff. About 20 seconds later, the dual tachometer indicated 100% for engine and main rotor speed, and all engine and system instruments were within their normal operating ranges.
At 0832:46, the helicopter began to move, consistent with getting light on the skids, and the engine torque began to increase.
About 5 seconds later, the south light disappeared from view as the helicopter’s nose appeared to move right in conjunction with an increase in right roll. At that time, the engine torque was between 50-60%.
Between 0832:51 and the end of recorded video/parametric data at 0832:53, the helicopter continued to increase in right roll while the engine torque increased to about 75%.
The camera’s view of the instrument panel was obscured during the final moments of the video, but the parametric data indicated that the helicopter was about 2 ft above the helideck, rolled right about 32°, with a right roll rate of about 68 degrees per second when the [Vision 1000] device stopped recording.
The investigators also had a 31 second video filmed by the passenger in the rear left forward facing cabin seat. In the timing format used below, SS:FF, SS are the elapsed seconds, and FF
the number of elapsed frames:
- From 00:00 – 27:21, the helicopter was stationary on the helipad.
- At 27:22, the helicopter showed movement consistent with being light on the skids.
- At 28:20, the helicopter started ascending. The helicopter did not appear to drift in either left or right or forward or back.
- From 29:12 to 30:10, the helicopter started rolling to the right, and the recording showed the left skid started to rise.
- At 30:23 as the helicopter continued to roll to the right, the left skid and float is visible (see below).

- An angle between the horizon and the bottom edge of the left seat window was apparent. The time from when the helicopter began to ascend and began to roll was approximately 1.5 seconds.
- At 31:06, fragments of the helicopter’s main rotor blades were visible in the air.
- The video ended at 31:19.
A dynamic rollover occurs when a helicopter rolls around a pivot point. Dynamic rollover begins when the helicopter starts to pivot laterally around its skid or wheel. Three factors must be present:
1. A rolling moment
2. A pivot point other than the helicopter’s normal CG
3. Thrust greater than weight
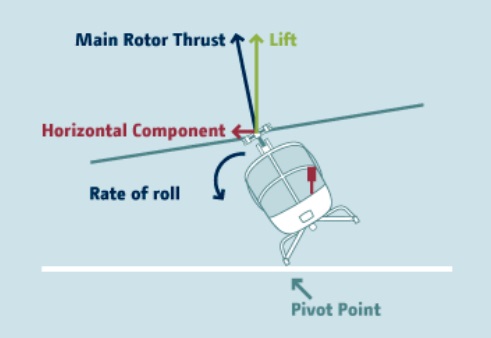
Dynamic Rollover (Credit: EHEST via ESPN-R/EASA)
NTSB Probable Cause & Informal NTSB Safety ‘Suggestions’
The pilot’s failure to ensure the helicopter was clear of obstacles before takeoff from the helideck, which resulted in the helicopter’s right landing skid pivoting about a helideck perimeter light during takeoff and a dynamic rollover.
Additionally, the pilot’s improper takeoff technique likely contributed to the development of dynamic rollover.
In common with most NTSB rotorcraft investigations, NTSB raised no formal safety recommendations. NTSB staff did unusually made the following “safety suggestions” within a specialist report, which were reportedly accepted and implemented by RLC.
- Paint aiming circles on the helipads located at the RLC property in Broussard, Louisiana; so that pilots under training have additional opportunities to train on landing in the center of an aiming circle.
- Do not allow passengers to place the front left-seat headset on the windscreen center piece and leave them there during flight.
The logic of the first point is evident. However, as these pads are not coincident with a Final Approach and Takeoff Area (FATO) its perhaps not surprising that no such markings are evident currently at Broussard. The latter point is not linked to any factual data in the final report or public docket.
The Safety Record of Rotorcraft Leasing (RLC)
This was RLC’s third accident of 2022, and its second fatal accident of the year:
- 14 January 2022 B407 N167RL impacted the ground near Houma, Louisiana. The NTSB have yet to determine a probable cause but information released so far indicates a possible pilot incapacitation. Both occupants died.
- 15 December 2022 B206L4 N414RL fell into the sea from the Ship Shoal 105C offshore installation in the GOM after its skids got trapped in the deck edge ‘skirt’ rolled over and fell off the deck (very similar to this accident two weeks later). In this case the three occupants were rescued by the USCG from an aircraft raft. The pilot recalls an underwater egress and “swimming towards the light”. The NTSB determined the probable cause to be: “The pilot’s improper takeoff technique that allowed the helicopter skid to drift into a helideck light, resulting in a dynamic rollover”. That pilot had joined RLC in May 2022 with 1265 hours, almost all on the Robinson R22 or R44. They had reached 1437 hours (172 more) by the time of the accident. In an undated FAA statement it is suggested by the RLC Chief Pilot that this aircraft drifted into a helideck light (again mounted on the permitter net). The height of the lights on SS105C is not detailed.

In another case study we examined the 11 December 2008 loss of RLC B206L4 N180AL with the loss of 5 lives and, in particular, survivability issues at low sea temperature and late alerting of rescue services: So You Think The GOM is Non-Hostile? The sea temperature could have been a factor in the December 2022 accident as cold shock can prevent cabin egress.
We have previously covered the ditching of RLC’s N373RL on 11 November 2012 after a power loss on takeoff offshore. The four occupants in that case were uninjured.
We have also reported on an RLC accident on 25 September 2021 where B407 N662RL was lifting off for departure from a heliport in Patterson, Louisiana when and drifted backwards into B407 N668RL.
Our Observations
In the first version of this article, after the preliminary report was published we wrote:
We would expect a competent safety investigation to consider the operator’s safety management & especially its response to the accident 2 weeks before, the suitability of sub-D decks and single engine helicopter operations, the design standards applied to helidecks, the SAR / emergency response & the survivability aspects and the FAA‘s regulation of offshore helicopter operations & BSEE‘s regulation of offshore installations.
While we were pleasantly surprised with the volume of data and investigative effort expended by the NTSB in this helicopter accident, we are rather disappointed by their negligible examination of these systemic issues and lack of mention of a similar event just two weeks before.
The existence of an SMS is only mentioned briefly in the 369 page pack of interviews for example, with no review of its effectiveness. This is surprising as a similar accident had occurred only two weeks earlier in the same operator.
Flight Data Monitoring (FDM), using the Vision 1000 data, would be a means to verify pilots pulled into a low hover.
One might think the ‘flat’ lighting solution adopted for the circle & H lights concept developed in the UK might be a better form of perimeter lighting for sub-D helidecks. The NTSB’s claim that the use of 8 in not 6 in light being immaterial seems highly dubious when the damage on the lights is examined (see Image 3a above) the damage is worse at 5.75 in height and on a 6 in light the skid may well have slide over the ‘dome’ of the light’s guard.
There is no further evidence relating to the USCG’s SAR actions.
While typos are always possible in large documents, it is disappointing that the errors on which deck the blade debris was found on and the error on the TDPM diameter where not spotted in review before publication. The dubious claim about that the light height probably should have been challenged before the report was issued too.
Safety Resources
The European Safety Promotion Network Rotorcraft (ESPN-R) has a helicopter safety discussion group on LinkedIn. You may also find these Aerossurance articles of interest:
- CHC Scotia AS332L Rollover on West Navion Helideck After Loss of Dynamic Positioning
- Review of “The impact of human factors on pilots’ safety behavior in offshore aviation – Brazil”
- Fatal Mi-8 Loss of Control – Inflight and Water Impact off Svalbard
- Canadian Coast Guard Helicopter Accident: CFIT, Survivability and More
- Korean Kamov Ka-32T Fire-Fighting Water Impact and Underwater Egress Fatal Accident
- NH90 Caribbean Loss of Control – Inflight, Water Impact and Survivability Issues
- Dramatic Malaysian S-76C 2013 Ditching Video
- South Korean Fire-Fighting Helicopter Tail Rotor Strike on Fuel Bowser
- Ditching after Blade Strike During HESLO from a Ship
- US BSEE Helideck A-NPR / Bell 430 Tail Strike
- AS350B3 Ditching Japan
- GOM Helicopter Ops 2000-2019: Single Engine Usage Plummets But Fatal Accident Rate Resistant
- Air Ambulance B407 Hospital Helipad Deck Edge Tail Strike During Shallow Approach
- Gazelle Caught Out Jumping a Fence
- SAR Questions Feature in PNG AIC B427 Accident Investigation
- S-92A Collision with Obstacle while Taxying
- Helicopter Destroyed in Hover Taxi Accident
- Air Ambulance Helicopter Downed by Fencing FOD
- Be Careful If You Step Outside!: Unoccupied Rotors Running AS350 Takes Off
- AS350B3 Rolls Over: Pilot Caught Out By Engine Control Differences
- AS350B3 Dynamic Rollover When Headset Cord Snags Unguarded Collective
- Ambulance / Air Ambulance Collision
- Loss of Bell 412 off Brazil Remains Unexplained
- Taxiing AW139 Blade Strike on Maintenance Stand
- Investigation into Collision of Truck with Police Helicopter
- Offshore Night Near Miss: Marine Pilot Transfer Unintended Descent
- North Sea Helicopter Struck Sea After Loss of Control on Approach During Night Shuttling (S-76A G-BHYB 1983)
- Night Offshore Training AS365N3 Accident in India 2015
- Loss of Control, Twice, by Offshore Helicopter off Nova Scotia
- Night Offshore Windfarm HEMS Winch Training CFIT (BK117C1 D-HDRJ)
- Blinded by Light, Spanish Customs AS365 Crashed During Night-time Hot Pursuit
- UPDATE 4 February 2023: S-92A Offshore Landing Obstacle Strike: CENIPA Report
- UPDATE 11 February 2023: Urgent Exit Required: A Helideck Incident (Omni Sikorsky S-76C+ PR-SEC)
The UK CAA publish the widely adopted CAP 437: Standards for offshore helicopter landing areas