Wreckage of Norsk Luftambulanse HEMS Airbus Helicopters EC135P2+ LN-OOI (Credit: AIBN)
History of the Accident Flight
According to the Accident Investigation Board Norway (AIBN) investigation report (issued in June 2015), the helicopter and its crew were on standby at Lørenskog, Oslo when a call was received to attend an overturned lorry 21 nm away near Sollihøgda on the E16. The aircraft was airborne 9 minutes after the ambulance control took the 112 call. The Aircraft Commander was in the front right seat, the HCM in the front left seat and a physician, as a medical passenger, in the right-hand cabin seat.
En-route, the physician received the accident site coordinates via the fleet management system LOCUS used by the emergency medical communication centre. The HCM set a course for position 595950N 0101810E in the helicopter’s digital map system ([EuroAvioincs] EURONAV [5]) and the course to the traffic accident site was displayed on the cockpit multi-function display.
EC135 Cockpit: The large display on the left is operated by the HEMS crew member. He can choose to view the moving map on the entire display, as shown in the picture, or to split the display, as shown for the pilot on the right. A third possibility is that the display on the left shows flight instruments on the top half and the moving map on the lower half of the display (Credit: AIBN)
The crew were “very familiar” with the destination but the HCM “followed the procedures regardless and zoomed in on the possible landing site on the moving map display”. He noticed an adjacent powerline.
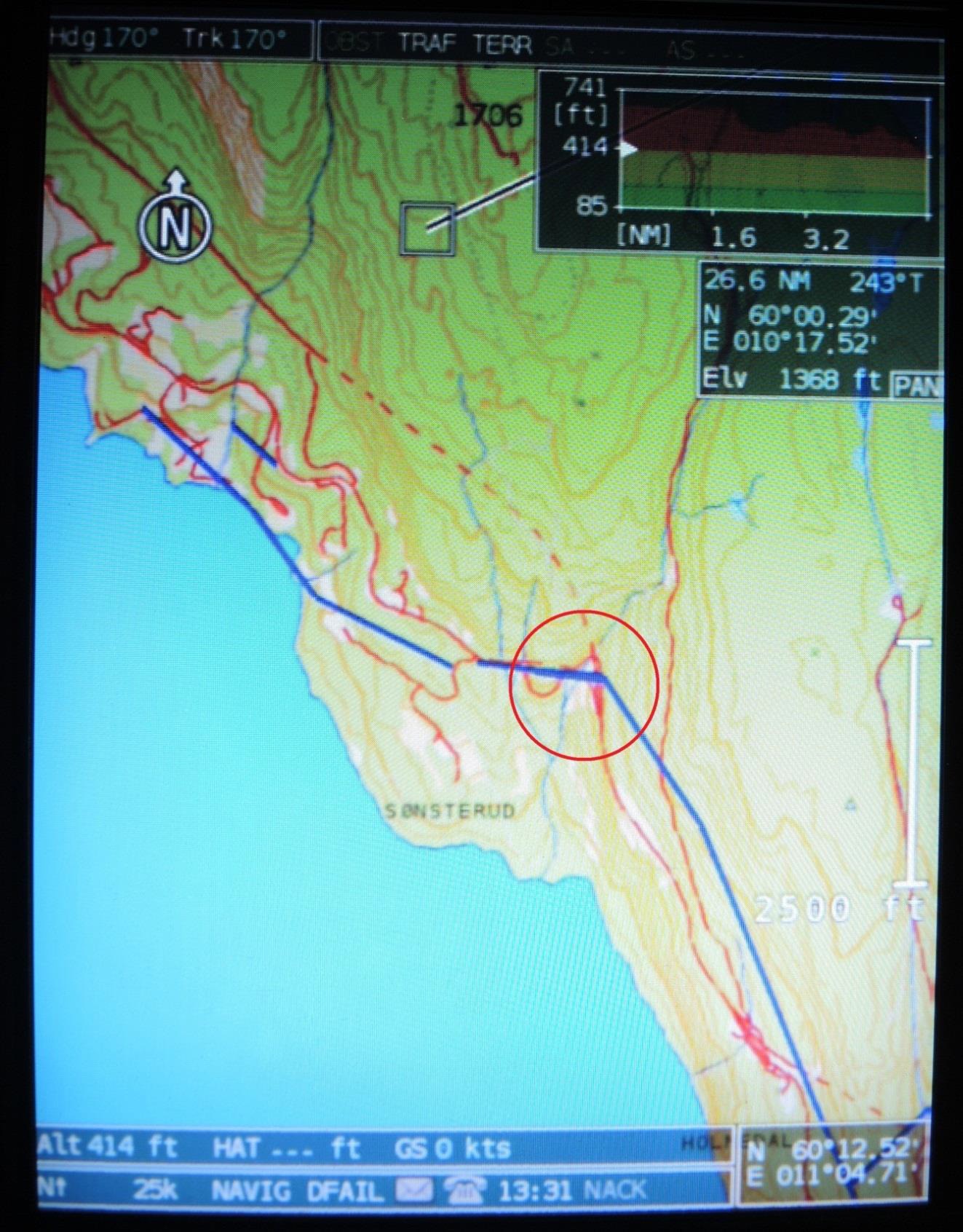
EUONAV Display of Available Mapping. Powerlines in Blue (Credit: AIBN)
The pilot acknowledged it and the doctor was also informed for situational awareness. They tried calling the emergency services on site at the road accident (on Channel 33 – VHF ‘Medical’)) without success. The aircraft was also fitted with radios for the digital emergency network (TETRA). This was not however in use in that district at the time. The introduction of TETRA elsewhere had been problematic due to weak management of change and crews had become use to often landing without having achieved radio contact with ground units.
After a ten-minute flight, the helicopter arrived at the scene of the traffic accident which had occurred between the exits of the Nes and Sønsterud tunnels.
Accident Site Norsk Luftambulanse Airbus Helicopters EC135P2+ LN-OOI (Credit: Police via AIBN)
The aircraft commander reduced the speed to 50 kt and flew approx. 200 m south of the site, in a south-western direction, at approx. 800 ft. altitude above the ground (1 461 ft. MSL) in order to find a suitable landing area.
According to the HCM, they flew relatively fast and high, and were not on particular lookout for any aviation obstacles [and] he and the aircraft commander agreed to land on the road by the southern exit of the Nes tunnel [where there was an emergency lay-by].
A survey of the operator’s employees conducted by AIBN after the accident confirmed this was a reasonable site, considering the obstacles the crew had spotted (a line of streetlights and a coincident low powerline).
After passing the landing site, the helicopter continued on a south-western course, at the same time as it descended to 700 ft. (MSL) and made a wide right turn. It then slowly continued towards the landing site in a north-eastern direction.
[The operator’s OM-A (Operations Manual Part A General)] does not describe a special procedure for landing in areas where the moving map indicates that there is a power line or other aviation obstacles. OM-A also does not contain a description of how the crew should use their eyes to look for aviation obstacles in the most critical final part of approach and landing.
On site two police officers had been scouting for a suitable landing site. They were aware of various obstacles and tried calling the aircraft (on Channel 5 – VHF ‘Rescue 1 [Guard]’) four times without success. The HCM meanwhile…
…gave the aircraft commander the all clear. After landing check was performed, he switched to flight instrument mode on the multifunction display. Accordingly, the moving map was no longer displayed. All three focused on looking for aviation obstacles. The helicopter flew horizontally with a speed of 8 – 10 kt while the aircraft commander turned the nose of the helicopter somewhat to the left so that it started to fly sideways.
As they approached poles with a line between them, the HCM opened the door on his side and looked down to ensure that there was good clearance between the obstacle and the helicopter. As he closed the door and looked forward again, he heard a bang and the helicopter started to shake severely.
Norsk Luftambulanse Airbus Helicopters EC135P2+ LN-OOI Contacting Wire: The helicopter has hit the lower ground wire with the wire cutter and pulled it in the direction of flight. The main rotor rotate under the live lines. The lower powerline between the street lights along the E16 entry ramp is visible in the bottom of the photo (Credit: via AIBN)
LN-OOI had hit the power line marked on the moving map. It consisted of three live lines and a grounded line that crossed directly above the line between the street lamp posts. The latter lines [which the crew had seen and were monitoring] were not indicated on the map.
All of the wires [stuck] were aluminium, with a diameter of 10.5 mm, and had a steel core with a diameter of 5 mm. The power line voltage was 22 000 V. The three live lines were installed horizontally with a distance of 1.5 m between them. The groundwire was located 2 m below the southern live wire. The western pole was 10 m high and was partially hidden between trees on an approx. 30 m high knoll. The eastern pole was 11 m high and was located between trees on an approx. 20 m high nearly vertical rock out. The highest point on the power line was 35 m above ground.
Accident Site Norsk Luftambulanse Airbus Helicopters EC135P2+ LN-OOI. Photo taken facing east on the same day as the accident. The power line poles are marked with red arrows. The helicopter wreckage is located behind the trees marked with a green arrow. (Credit: Police via AIBN)
The helicopter hit the power line at an altitude of 25 m above the terrain, approx. 62 m from the eastern pole. The lowest wire got caught in the helicopter’s wire cutter. However, the wire was merely pulled away without being cut. Then the main rotor blades came in contact with the live wires and several powerful flashes occurred. All lines were cut and the helicopter started to fall straight down.
Norsk Luftambulanse Airbus Helicopters EC135P2+ LN-OOI MRB Strikes Wire: (Credit: via AIBN)
One rotor blade broke as the main rotor hit the wires. The main rotor started to shake heavily in relation to the helicopter fuselage, and…the main gear box and main rotor were about to come apart from the fuselage.
The helicopter fell down in a rock fill embankment on the southern shoulder of the entrance ramp to E16 near the eastern tunnel entrance at the Sønsterud tunnel.
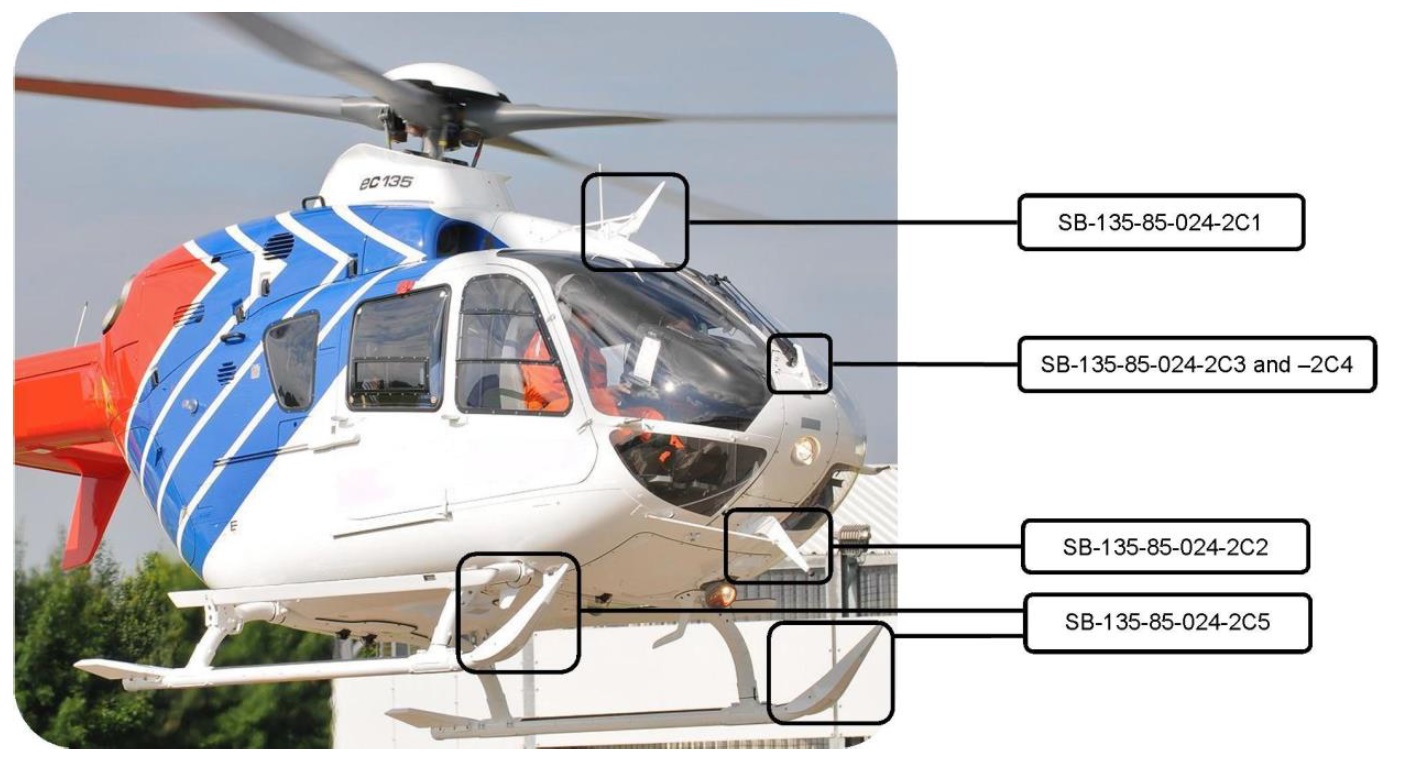
LN-OOI was equipped with wire cutter, devices that will deflect and cut power lines and transport cables if the helicopter collides with these. There is an upper and lower knife that will cut wires.
EC135 Wires Strike Protection System (WSPS (Credit: Airbus via AIBN)
The precondition is that the target is within the area for the upper and lower knives. If a wire passes above the upper knife, it could hit the main rotor. If a wire passes below the lower knife, it will also pass under the skids. According to Airbus Helicopters, the system is designed so that it is efficient at speeds between 13 and 52 kt.
Mapping & Marking of Obstacles Background
EURONAV contain[s] a database with digital maps that provide more detailed information as you scale up the map. Aviation obstacles are presented…in the form of symbols and lines…based on map data from Statens kartverk (the Norwegian Mapping Authority [NMA]). The NMA is required to keep a register of aviation obstacles…. The information…mainly comes from reports which obstacle owners are required to provide through the regulations relating to aviation obstacles. The NMA has an online form that must be used when reporting measures or structures that could obstruct or be a danger to aviation. The NMA also carries out several tasks to quality control the database content: Photogrammetric inspection of obstacles (normally aerial photo); Visual verification from the ground [and] Analysis of other data sets to identify obstacles (particularly power lines).
The power line [struck] at the accident site had a maximum height of 35 metres above the terrain. It was thus subject to reporting requirements, but not subject to marking requirement [being less than 60 metres]… The low power lines between the lamp posts were not subject to reporting or marking requirements.
In a meeting between the AIBN and airport department of the Civil Aviation Authority on 19 November 2014…the CAA then stated had been working to have the entire country laser scanned. This initiative was taken in part due to implementation of requirements in ICAO Annex 15 (Aeronautical Information Services) through EU Commission Regulation 73/2010 relating to Aeronautical Data Quality (ADQ). A number of state agencies would benefit from such a digital mapping of the country, but they had been rather unwilling to share the expenses. The CAA clearly saw the safety potential of improving the overview of aviation obstacles in Norway, but does not have the authority or financial capacity to take on this task alone. They…believed than an interdepartmental collaboration and financing model
needed to be in place first.
A representative from the Swedish Transport Agency has stated that 75 – 80% of the country has already been laser-scanned. The work took place as a collaboration between Lantmäteriet (equivalent to the Norwegian Mapping Authority), LFV (a parallel to Avinor) and Forsvarsmakten (Swedish Armed Forces), among others. The objective was to quality-assure the obstacle data which the Swedish Armed Forces was already
managing. The grounds for performing laser scanning was also one of the requirements in EU Commission Regulation 73/2010 concerning ADQ.
Norsk Luftambulanse passed this NMA data to EuroAvionic for integration with EURONAV. After the accident it became apparent there was also detail on some lower obstacles in two other NMA digital mapping databases.
The presentations in the EURONAV system only indicate the height over the terrain of obstacles that exceed the height subject to marking requirements in accordance with the regulations (60 m).
Operator’s Safety Management Background
At the time, the operator was transitioning from the a Joint Aviation AuthoritiesJAR-OPS 3 flight safety programme to a safety management system (SMS). They had a web-based system for raining safety reports (introduced in 2010). AIBN say:
A [safety] database search revealed that 119 flight operations reports were registered in all of 2013. A total of 129 flight operations reports had not been fully processed in the autumn of 2014. A significant portion of these dealt with operating issues with the communications system and EURONAV.
A survey of employees conducted by AIBN after the accident suggested to AIBN that “EURONAV was a good aid, but it was not possible to trust that all aviation obstacles were shown on the moving map”.
The [safety] database contained two reports that dealt with hazardous situations with aviation obstacles. When unknown aviation obstacles are discovered, this is reported via the company’s technical rescue manager, who in turn reports to the Norwegian Mapping Authority for updating the “National register of aviation obstacles”.
Immediately following the accident, the company established an internal investigation group. This group has provided useful and good information to the AIBN. On 12 May 2014, the group submitted an extensive internal investigation report. Among other things, the report contains 13 safety recommendations that are directed both at internal conditions and factors outside of the company’s control.
Multiple safety recommendations relate to standardisation of the procedures during VFR approaches to unknown landing sites. Key topics are reconnoitring, communication, visual verification of aviation obstacles and sterile cockpit concept in the final part of the approach. Furthermore, the report recommends several improvements as regards aviation obstacles, databases, digital maps and power line detection systems. The report also recommends improvements in communications, training and reporting of nonconformities. The investigation group also provided recommendations to limit the extent of damage and simplify accident investigations by e.g. recommending improvements in flight following and by recommending that future helicopters are outfitted with flight recorders and cockpit voice recorders.
AIBN Analysis: Introduction
The investigators open their analysis with some reflection (our emphasis added):
This accident generally seems easy to explain because the course of events is well documented.
The accident took place during a highly ordinary mission with a very experienced crew in weather conditions that should not pose problems. The chosen landing site was seemingly very suitable, but the crew did not detect in time that a power line ran across the final part of the approach.
Only when looking beyond the completely obvious cause and effect can you see that the accident is more complicated. An analysis of underlying factors of a safety-related significance is important because it can form the basis for lasting improvements that can help prevent similar accidents in the future.
At the start of their report the AIBN states:
The Accident Investigation Board has compiled this report for the sole purpose of improving flight safety. The object of any investigation is to identify faults or discrepancies which may endanger flight safety, whether or not these are causal factors in the accident, and to make safety recommendations. It is not the Board’s task to apportion blame or liability.
In their analysis the AIBN are scrupulous in not only not appropriating blame but also not implying blame and diverting from their mission of highlighting lessons to improve safety.
AIBN Analysis: Site Selection and Approach
AIBN conclude that the site selected as a candidate landing site was reasonable and that it would be advantageous if lay-bys were specifically designed so they could also serve as suitable landing sites.
The reconnaissance that took place was neither particularly thorough nor particularly superficial. The landing site was in many ways suitable, provided that you were aware of the location of all obstacles in the area.
The AIBN commented positively about much of the crew’s technique approaching the site. They go on that:
The helicopter was flying mostly horizontally for the final part of the approach and could not start final descent until it had passed the lamp posts. Landing was imminent, and it is natural to assume that both the commander and HEMS crew member were focusing forward and downward towards the chosen landing site at the time of the collision. [Their eyes would have needed to] have been directed forward or at an angle upward in order to detect the lines that collided with the helicopter above the cockpit.
The commander’s potential thoughts about power lines during the final phase are unknown. It can be speculated whether the commander assumed that the power line he previously saw shown on the moving map was behind the landing site, whether he became distracted and forgot, or whether he confused the power line with the line between the lamp posts.
AIBN seem to believe that distraction or a failure to recall the lines marked on EURONAV was most likely
AIBN Analysis: Why the Powerline Was Missed
AIBN say that 9 potential barriers that could possibly have prevented the wire strike or its consequences were not functioning effectively or were missing:
Neither the lines nor the poles were physical marked, and it was unusually difficult to detect the power line.
The helicopter had no sensors that could have detected and provided a warning about the obstacle.
The helicopter’s moving map system had a visual warning function, but the system had weaknesses and was not used during the final part of the approach.
The preparations for landing do not appear to have included a positive verification of where in the terrain the power line they saw on the map was actually located.
They probably also did not discuss whether the overhead line may have been removed, or whether it was actually the line between the lamp posts that was shown on the map.
The police did not succeed in achieving contact with the crew via communications to inform about the landing conditions.
The crew was not successful in achieving contact with personnel on the ground via communications.
The helicopter’s wire cutter did not work due to the low speed.
Latent weaknesses in the company’s established system for creating and maintaining sufficient safety margins during approach to unknown landing sites and approaches during time pressure may have influenced the crew’s decisions.
They comment:
It was unusually difficult to spot the power line which the helicopter hit, and nearly impossible to detect visually from the angle in which the helicopter was flying. There was no snow on the lines. It was difficult to spot the grey colour against the busy backdrop. The southwestern poles were the same colour as the trees they were hidden behind, and the northeastern poles were hidden amongst trees. It was also difficult to see signs of power line corridors through the forest. The AIBN therefore believes that the circumstances indicate that the accident could have happened to any crew in the company.
They then observe and ask:
The helicopter collided with a power line that was shown on a moving map with built-in obstacle warning that was available in the cockpit. It is therefore reasonable to ask why this advanced safety barrier did not prevent the accident.
In response, they highlight the following:
The crews in Norsk Luftambulanse AS have never had access to fully reliable and exhaustive map information.
Important aviation obstacles have been left out, and there are examples of aviation obstacles that have been physically removed several years ago still being shown on the maps.
The map and warning system for aviation obstacles was known for being unreliable, which resulted in little faith in the warning system in the moving map.
The relevant power line was shown on the moving map, but the height was not specified.
There was no audible warning that could call on the crew’s attention in the event of collision risk, the warning was just a symbol change on the display.
When it comes to preventing collision with aviation obstacles, the moving map systems have historically been a supplement.
The company’s operative personnel appear to have had varying levels of familiarity with the EURONAV warning system. Although required training was provided, there were no suitable procedures for use.
The procedure describing that the moving map should be visible when landing in unknown locations, focused on missed approaches rather than detection of obstacles in connection with landing.
Based on this, AIBN concludes that when the LN-OOI accident occurred, neither the moving map system nor the practical use of it were sufficiently mature in order to expect that the visual obstacle warning would have prevented the accident. Considerable luck and circumstance would have been involved if this worked as a safety net. Nevertheless, the accident illustrates a potential. It would theoretically have been possible to use information that was available on board to detect and alert the crew of an obstacle that they were not aware of.
It is worth noting that EURONAV is today a widely used and popular system in air ambulance, police and SAR applications
AIBN then discuss possible improvements:
A good obstacle database, in combination with a functional GPS-based warning system, including audible warnings, could constitute an additional safety net by alerting the crew to collision risk and thus preventing an accident.
An improvement of the moving map databases is essential in order for warning systems related to moving maps to function satisfactorily. A safety improvement in this area presumes the following:
1) The Norwegian Mapping Authority must be given the resources to prepare the most exhaustive database possible of obstacles that could constitute a safety risk for aviation. Much of the information already exists, but quality of the data must be assured and information coordinated in a better manner. Insofar as possible, the database must also include obstacles lower than 15 m. This work should include an imminent revision of the regulation relating to reporting, registration and physical marking of aviation obstacles. Furthermore, it should be made as easy as possible for users to report new obstacles or to have them deleted from the database if they no longer exist. Establishment of a new national height model will also help increase safety.
2) It must be possible for the obstacle database to be used by GPS-based systems for warning of aviation obstacles. In this connection, it is important that information from the map database can be exported in a format that satisfies the needs of the equipment manufacturers.
Norsk Luftambulanse HEMS Airbus Helicopters EC135P2+ LN-OOI – Rotor head, rotor mast, pitch mechanism and parts of the power line. Cut pitch links are marked with red arrows. (Credit: AIBN)
AIBN Analysis: The Operator
The investigators acknowledge that:
It is generally accepted that standardisation results in increased safety margins, however, there is a fine line here from preventing the procedures from becoming so detailed and rigid that they become useless.
However the AIBN challenge an assertion that HEMS is so varied that VFR procedures can’t be standardised.
One argument for improving the procedures is transfer of experience. The company’s helicopters are flown with only one pilot. This means that the training of new pilots in the company cannot take place during a period as first officer before receiving full responsibility as a commander. Commanders could therefore more easily start habits that deviate from best practice. Some harmonisation will take place naturally via the HEMS crew members, but in this investigation, commanders, HEMS crew members and physicians described differences in execution.
Opportunities for improvement they highlight include:
That crew members update each other during landing brief regarding what threats to expect and how they will be handled.
How to relate to obstacles shown on the map before landing, including both visual verification and approach if verification is not achieved.
The functionality of moving maps and associated warning system and procedures for efficient utilization.
Goal to establish radio communication with personnel on the ground before starting the final part of the approach.
Sterile cockpit concept, i.e. that everyone on board is only working on flight operations tasks during take-off, approach and landing.
A better description of the work load sharing and tasks in the cockpit during the final part of the approach and landing.
Keep human performance and limitations in mind when defining the HEMS crew member’s work load and focus areas during approach and landing.
Considerations when selecting landing sites.
Establishment of predefined landing sites/ambulance meeting places, including a system for communicating information about these.
Good communication concerning the status of relevant patients, so that the landing site decision can be made with the best possible basis, and also reduce unnecessary time pressure.
On regulatory oversight the AIBN note that:
….before the accident, the CAA carried out operator surveillance by the authority focusing on the company’s quality system and flight safety programme, among other things, and no deviations were documented. The weaknesses identified in the company’s procedures in connection with the investigation of this accident were not obvious and the AIBN believes it is understandable that they were missed by the CAA during the audit. Thus, there is no basis for claiming that the lack of findings indicates a failure in the surveillance work. However, the AIBN cannot fail to remark that the two most recent flight operations inspections appear to have been superficial, judging from the reports.
AIBN Analysis: Survivability
Examination of available video material shows that the helicopter fell for approx. 2.7 seconds before it hit the ground [banked approximately 50° to the left when it hit the ground]. Given an approximate constant acceleration, this entails that the helicopter had a vertical speed of 18 – 19 m/s [c 61 ft/s] when it hit the ground (just under 70 km/h). Roughly, the cockpit was relatively intact; hence, there remained adequate survival space after the crash.
This does highlight the structural strength of modern helicopters. The aircraft was fitted with seats certified for impacts of “20 G vertically and 8 G sideways (horizontally)” say AIBN.
Based on an overall assessment of the injuries and damage sustained by the crew and the helicopter, viewed in relation to what they could be expected to withstand, the AIBN believes the load when the helicopter hit the ground exceeded 20 G.
AIBN say “the loads during the accident where on the limit for what can be survived” and are “of the opinion that it will be difficult to give people sitting in seats good support and cushioning from lateral crash forces without this posing a hindrance to necessary freedom of movement”. They comment that airbag solutions may be possible in some cases.
The HCM survived even though he was sitting on the side of the helicopter that hit the ground first. An explanation could be that the left cockpit door provided support against sideways movement. The door eventually hit the ground, which further limited sideways movement. This may have resulted in a more even distribution of crash forces over larger parts of the body.
AIBN Safety Recommendations
AIBN raised three recommendations:
SL No. 2015/04T28: The AIBN is of the opinion that emergency lay-bys and picnic areas, insofar as possible, should be designed so they can also serve as safe landing sites for helicopters, and
therefore recommends that the Norwegian Public Roads Administration incorporate assessment of obstacles and other relevant factors in the standard that applies for design of such places.
SL No. 2015/05T: The AIBN recommends that the Ministry of Transport and Communications take responsibility for coordinating the work on further developing the current obstacle database with the aim of
utilising the safety benefit that can be gained from modern GPS-based warning systems.
SL No. 2015/06T: The AIBN recommends that Norsk Luftambulanse AS revitalise its work on identifying and handling risks associated with landing at unknown landing sites.
The European Safety Promotion Network – Rotorcraft (ESPN-R) has published this video and guidance with EASA:
Aerossurance has extensive air safety, flight operations, SAR, HEMS, airworthiness, human factors, aviation regulation and safety analysis experience. For practical aviation advice you can trust, contact us at: enquiries@aerossurance.com