Accident Report: Fatal Police Helicopter Double Engine Flameout Over City Centre (A109K2 JA11PC)
While returning from a routine patrol over a crowded city both engines flamed out on a police helicopter. Due to the helicopter’s low altitude and the congested environment the aircraft crashed into buildings with multiple fatalities. We examine at the accident investigator’s final report and highlight the value of studying accidents internationally.
The Helicopter Accident
You might have assumed was the tragic accident in Glasgow, UK, 29 November 2013 (UPDATE 23 October 2015: discussed here). In fact it was an AgustaWestland A109K2 JA11PC of the Shizuoka Prefectural Police in Shizuoka City on 3 May 2005.
During a routine traffic congestion patrol at around 16:28 Local Time on a National Holiday (Constitution Memorial Day), the helicopter, call sign ‘Fuji 1’, crashed into a residential area in Kusanagi, Shimizu-ku, Shizuoka City. The aircraft was destroyed and a post-crash fire broke out. All five police officers on board were fatally injured.
The Japanese Aircraft and Railway Accidents Investigation Commission (ARAIC) issued their final report 28 March 2007. Note that on 1 October 2008, ARAIC merged with the Japan Marine Accident Inquiry Agency (JMAIA) to form the Japan Transport Safety Board (JTSB).
History of the Flight
A routine afternoon road congestion survey flight was to be conducted using the ‘Fuji 2’, Eurocopter AS365N3 JA22PC, by the local Prefecture’s police aviation unit (one of many across Japan), which the investigators refer to as ‘the flying squad’. The flight had been planned to cover the eastern area of the prefecture, but when the team of observers from the Traffic Regulation Division arrived, 40 minutes before the planned take-off, they asked to include a congestion survey on the Tomei Expressway in the west of the prefecture too and the Pilot In Command (PIC) agreed.
Following a technical fault shortly after take-off at 14:00, Fuji 2 returned to base and five of the seven people on-board transferred to the slightly smaller Fuji 1, an AgustaWestland A109K2. The flight was expected to last 2 hours and the pilot filed a flight plan that estimated 2 hours 20 minutes of fuel on-board. The change to the smaller aircraft resulted in one other significant change, namely the PIC choose to leave the co-pilot behind.
The replacement aircraft took off from Shizuhama Aerodrome at 14:42. Investigators concluded the aircraft took off 58kg over maximum gross weight, perhaps symptomatic of the rushed change in plans.
After taking off the aircraft flew an approximately 195nm route with a ground speed of about 110kt. The early aerial photos recovered were taken from a 1,000 – 1,500ft above ground level, but those photos taken later were from 1,000ft or below. The last photo was taken at 16:23:26, approximately five minutes before the crash. At 16:25 the PIC made a radio call “Over Shimizu. Landing soon.” It was usual to make a call to warn ground crew of their arrival and there was no indication of any abnormality. In these final few minutes, witnesses remarked on the aircraft’s particularly low altitude. The accident investigators report that:
a. At the point approximately 500m away from the crash site, flying altitude was approximately 300ft.
b. In the area mentioned in a. above, sound of the aircraft changed and went silent.
c. At the point approximately 150m away from the crash site, something fell away from the aircraft.
d. In the area mentioned in c. above, the aircraft was silent with the MR blades almost stationary.
e. At approximately 100m, the aircraft’s attitude changed greatly into a nose-down attitude.
f. The change of altitude from a. to e. was 10 – 20m.
g. In the area mentioned in
e. above, the aircraft’s course changed to the left.
The Helicopter Wreckage, Fuel State & Analysis of the Final Moments
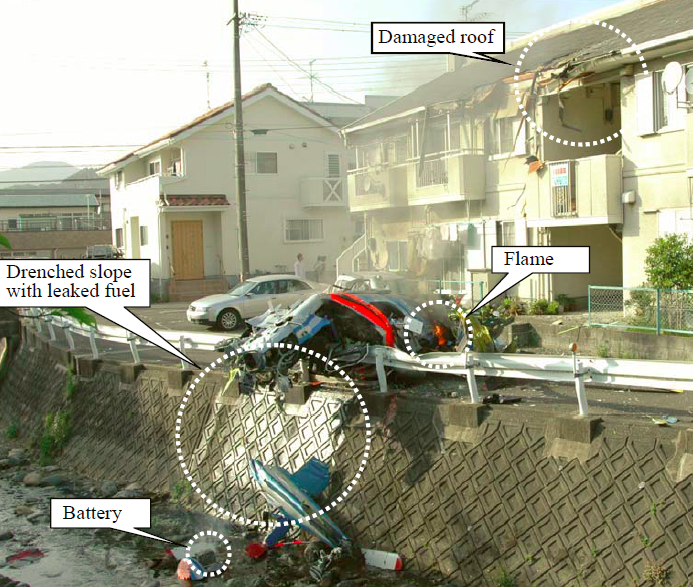
The point of impact was on a roadway between an apartment house and the Kusanagi River. The aircraft damaged the eaves of the building during the crash sequence. The aircraft came to rest on its left side with the cockpit on a crash barrier at the edge of the river embankment and a small post cash fire ensued.
The accident investigators report that:
The fuselage was destroyed and nearly burned out. All four MR blades were broken but still connected to the MR head. The tail boom was fractured in the middle. The forward half of the tail boom was folded forward onto the fuselage and the rear half was found on the riverbed several meters below with the TR blades still attached. There were traces of leaked fuel on the embankment.
No faults were found that could have caused the accident. Neither engine was developing power at the time of impact and the JTSB believe the left hand engine flamed out first.

The accident investigators estimate the helicopter departed with 432kg of fuel and that 1 hour 46 mins later, just prior to the accident, between 11 and 20 kgs remained. Consequently they consider it “very likely” that “while the fuel gauge indicated near zero, fuel was not yet depleted at the time of the crash”. The investigators note that with the fuel available, the pilot’s estimated endurance of 2 hour 20 min was “unfeasible”.
The investigators also state:
Because the aircraft was under low remaining fuel condition when it reached Shimizu-ku ward as described in 3.5.2, it should have made precautionary landing. Considering a normal operation with low fuel, it should have climbed and flown straight to the aerodrome. However, it is considered very likely that the aircraft was making low altitude meandering flight [for which no operational reason was identified by the investigation]. It is considered possible that the PIC was flying the aircraft unaware of low remaining fuel and illumination of FUEL LOW caution light(s). It was not possible to confirm why the pilot made an unusual flight (low altitude and meandering flight) even if he was unaware of low fuel.
Based on valve position, the accident investigators state:
…it is considered probable that, immediately before both engines lost their power, the PIC tried to supply or was supplying fuel via cross-feed valve.
Also:
…it is considered possible that, following the LH engine stall [sic], the PIC might have taken inappropriate actions, such as incorrectly operating fuel valves and pumps, power levers, or confusing LH and RH controls, resulting in loss of power of the RH engine.
…it is considered possible, that during the actions taken to stop, recover or otherwise handle the malfunctioned engine, the PIC would have moved the controls quickly (such as rapid collective lever movements and corresponding rapid cyclic stick movements) to control aircraft attitude, which would have resulted in loss of power of the other engine against his intentions.
The accident investigators believe that by the time the helicopter was 500m from the accident site, both engines had flamed out. At the time:
…it is considered probable that the aircraft was flying at an altitude of approximately 300ft at a speed of 110 – 120kt
While this is a surprisingly low altitude, the investigators state that entry to autorotation should have been possible:
It is considered possible that after both engines lost power the MR rpm decayed sharply because the collective lever was mistakenly pulled up.
The PIC was possibly affected by the following; excessively low-flying altitude, unexpected stall of both engines, or second engine stall that occurred against his intentions while he was dealing with the first engine that had stalled earlier. The reasons, however, could not be confirmed.
It is considered probable that, after both engines had lost power, the aircraft, without entering autorotation, experienced rapid decay of MR rpm, excessive MR blade flapping and lead-lag movement beyond allowable range leading to breakage and falling apart of the oil reservoir and lead-lag dampers on the MR head.
The Unit & the Helicopter Pilot
The pilot was the chief of the flying squad and held the post of the ‘chief officer responsible for aircraft operations’ as defined in the Rules on Police Aircraft Operations’ within the National Police Commission regulations. The accident investigators report that:
(1) The PIC was relatively cautious when piloting and was strict during training.
(2) As to the autorotation training as a means of emergency procedures, it was planned and conducted for each pilot, including the PIC, at least once every month. As the flying squad had three kinds of helicopters, autorotation practice using the [particular] aircraft [type] was sometimes carried out only once per three months.
(3) The PIC received autorotation full landing (autorotation landing procedure up to touchdown without using engine power) training on the type aircraft in Italy. After the flying squad introduced the aircraft, the PIC intended to provide autorotation full landing training to other pilots, but he decided to abandon this plan because he was not confident to take over the controls at the moment of touchdown.
(4) The PIC, who had been operating large-sized aircraft, had a tendency to move the controls rather liberally, but not in a manner of rough manoeuvring.
(5) The flying squad had established “The Flight Safety Standards” per the internal police directive concerning aircraft operations. The standards stipulate that “The operation manager shall be responsible for crew assignments” and that “The crew shall in principle consist of a PIC and another pilot who is qualified for PIC duties.” However, in emergencies or when needed to fly all three helicopters at the same time, there were cases where just one pilot flew a helicopter. For all three helicopters owned by the flying squad, the minimum required number of crew is one pilot.
(6) In five years since the introduction of the aircraft into the flying squad, there had been only two cases where FUEL LOW caution light illuminated during mission flights. One of the two occasions occurred when the aircraft was still under operational test just after the introduction. In both cases, flight phases were immediately prior to landing. The flying squad had so far conducted operation with ample fuel remaining.
(7) On normal missions, flying speed is approximately 100kt and flying altitude is 1,000 – 2,500ft. However, a helicopter may fly at slower speed and lower altitude to check situation if its crew discovers or is informed of a crime or an accident while in flight. But on the day of the crash there were no occurrences or reports of crime or accident in Shimizu-ku ward or in its vicinity.
(8) There had been no significant difference in fuel consumption between LH and RH engines of the aircraft, meaning no significant difference in indicated fuel level between LH and RH fuel tanks.
(9) Shizuoka Heliport is located approximately four kilometers northwest, and Miho airstrip is located approximately eight kilometers east-northeast of the crash site. Takeoffs and landings were frequently performed at these locations. Refueling were possible there.

Discussion
The Commission’s Probable Cause was:
It is considered very likely that this accident was caused by the crash of the aircraft, preceded by both engines power loss, no autorotation maneuver, MR rpm decay, and uncontrollable conditions, while the aircraft was flying on a road traffic congestion survey mission toward Shizuhama Aerodrome at low altitude on low fuel. The aircraft was destroyed and burned with five fatally injured onboard.
Causes of both engines power loss and why the aircraft did not enter autorotation were not confirmed.
Although it is considered probable that continued flight on low fuel and of low altitude contributed to the occurrence of the accident, reasons for these could not be confirmed.
The Bureau d’Enquêtes et d’Analyses (BEA), the accident investigation body for the State of Design of the engines, commented more specifically on the engine shutdown:
It could not be clearly determined why both engines lost power, but no anomalies were confirmed on the engines and their accessories that would have occurred before the crash. Furthermore, the probability of simultaneous in flight shutdown of both engines for technical reasons is very low. The most probable cause seems to be interruption of fuel supply.
Causes could not be determined why the aircraft did not enter autorotation.
The Commission goes on to add the following ‘safety opinion’:
While the reason could not be confirmed why both engines lost power and why the aircraft did not autorotate, it is considered possible that the following would have cumulatively acted as contributory factors to the occurrence of the accident. As the accident might not have occurred if any one of them had been cleared, persons concerned should keep the following items in mind as they perform operations.
(1) Flight operations became unreasonable after the unexpected change of flight plan
It is considered possible that the fuel load would have become insufficient for the flight after the flight route was extended from the original plan and aircraft were switched from Fuji No. 2 to the aircraft. Furthermore, it is considered very likely while higher flying speed increased the range and fuel consumption, it reduced the endurance. In addition, it is considered very likely that the aircraft eventually took off with exceeded maximum gross weight and this also would have contributed to increased fuel consumption. As fuel consumption is a function of such factors as gross weight and length of flight, all persons concerned should have carefully checked the fuel consumption and other parameters involved and operated the aircraft with feasible flight plan.
(2) Single pilot operation
Because minimum required number of persons on board the aircraft was specified as one pilot, single pilot operation is admissible. However, since unexpected occurrences are foreseeable, persons concerned should have as much as possible abide by “The two-pilot rule for safe flight”, which was stipulated in the voluntarily established Flight Safety Standards. In case where single pilot operation is a compelling need, crew assignment should not have been left solely to the discretion of the single person responsible for the mission assignment (the person who has the final authority to approve the pilot(s) for duty on each flight), but all persons concerned should have been involved to make such assignment in accordance with clearly defined criteria, which excludes consecutive flights of different types of aircraft.
(3) Low altitude flight
The aircraft was considered to be in a condition of flying at an altitude of a few hundred feet and at a speed of 110 – 120kt when both engines lost power and this condition is within the envelop of possible autorotation. Autorotation trainings are usually conducted from an altitude with sufficient safe margin. In this accident it is considered possible that low flying altitude at the moment of loss of engine power constituted a factor that prevented the aircraft from autorotation. If the PIC had maintained flying altitude as high as possible to secure sufficient time for gliding, it is considered possible that the PIC would have been able to make the transition to the autorotation with relative ease.
Comment
This accident also highlights how risk can increase when circumstances change at short notice (i.e. the traffic officer’s extended mission request 40 minutes before departure, the technical malfunction with the original helicopter at 14:00 and then the change of aircraft type and the change to single pilot operation prior to the second flight at 14:42).
The UK Civil Aviation Authority (CAA) issued a safety notice on 20 November 2014 on the matter of flight planning. In part it follows a January 2013 helicopter accident in London which Aerossurance discussed back in September. It highlights the European Helicopter Safety Team (EHEST) Pre-flight Planning Checklist as one potential tool that is available.
UPDATE 23 April 2016: Dim, Negative Transfer Double Flameout. This article examined a double engine flameout and associated human factors in an older generation helicopter in New Zealand. Fortuitously this day-time HEMS incident did not result in any casualties.
UPDATE 11 September 2016: Another case were a last minute change of plan was partly responsible for an accident: Final Report: AS365N3 9M-IGB Fatal Accident
UPDATE 4 August: 2018: US HEMS EC135 Dual Engine Failure: 7 July 2018
UPDATE 24 October 2019: EC135P2+ Loss of NR Control During N2 Adjustment Flight
UPDATE 24 November 2019: Austrian Police EC135P2+ Impacted Glassy Lake
UPDATE 21 December 2019: BK117B2 Air Ambulance Flameout: Fuel Transfer Pumps OFF, Caution Lights Invisible in NVG Modified Cockpit
UPDATE 2 January 2020: EC130B4 Destroyed After Ice Ingestion – Engine Intake Left Uncovered
UPDATE 18 July 2020: Vortex Ring State: Virginia State Police Bell 407 Fatal Accident
UPDATE 31 January 2021: Fatal US Helicopter Air Ambulance Accident: One Engine was Failing but Serviceable Engine Shutdown