Wreckage of All Nippon Helicopters Airbus EC135T2 JA31NH near Shizuoka Heliport (Credit: JTSB)
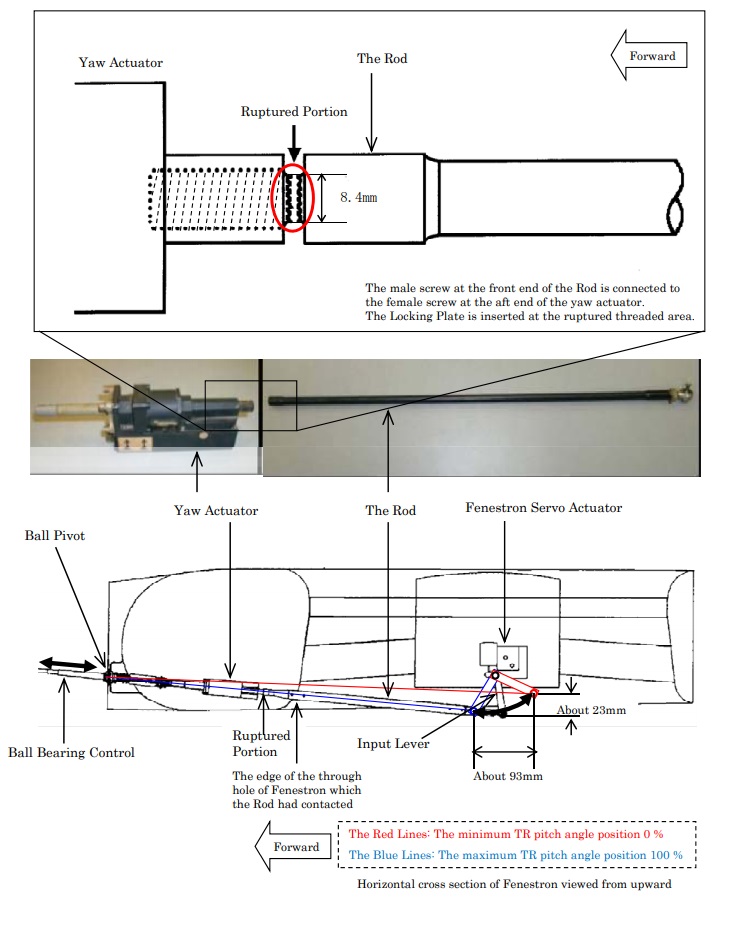
Investigators from the Japan Transport Safety Board (JTSB) determined that following the propagation of a fatigue crack, the tail rotor (TR) control rod had ruptured at the threaded connection to the yaw actuator during the flight and this made the tail rotor uncontrollable.
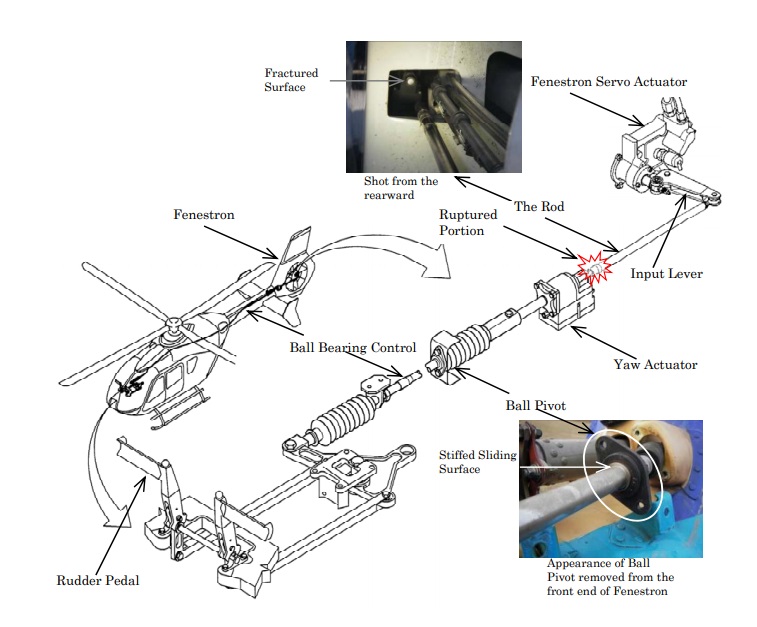
Airbus EC135T2 Tail Rotor Control (Credit: JTSB)
As the helicopter decelerating, the fuselage started to rotate, possibly after power was increased for a go-around, and the aircraft lost height and impacted the ground. The investigators comment in their safety investigation report that:
…it is considered highly probable that the captain did not perform an emergency procedure for the tail rotor failure conditions, as provided in the flight manual. It is considered probable that his failure to perform such an operation reflected the absence of a syllabus for tail rotor failure in the periodic training for the captain.
The investigators note that:
The maintenance manual provides that the periodical inspection of the TR control, including that of the ball pivot, must be performed every 800 flight hours or every three years, whichever occurs first. A periodical check for the Aircraft was performed by the Maintenance Service Company on March 9, 2006, 368 h 25 min in flight time before the occurrence of the accident. But there was no looseness in the threaded area of the Rod. There was no abnormality with the ball pivot, either.
However:
After the accident, it was found that the ball pivot had become stiff in the sliding surface due to corrosion. It is considered highly probable that the unusual feeling in the anti-torque pedal movement, which had been reported by several pilots, was caused by the stiffening of the ball pivot…
The investigation revealed that troubleshooting was performed on 20 October 2007, 45:35 flying hours before the accident, but this:
…was not performed in accordance with the trouble shooting procedure provided in the English written maintenance manual of the aircraft manufacturer. As a result, the inspection of the ball pivot was not performed and its stiffening was not found. In addition, the fact that the joint of the tail rotor control rod and the yaw actuator has a left-handed thread is provided in the English written maintenance manual of the aircraft manufacturer, but it is considered somewhat likely that the mechanic involved in this case, while intending to tighten the joint, actually turned the joint to the opposite direction to loosen it.
The investigators concluded that:
Therefore, it is considered highly probable that the threaded area of the Rod had become loose and the ball pivot had stiff sometime after the periodical inspection performed by the Maintenance Service Company and as a result, a crack created in the threaded area of the Rod.
Location of Rod Failure: All Nippon Helicopters Airbus EC135T2 JA31NH (Credit: JTSB)
They went on:
…it is considered highly probable that repetitive bending loads in excess of the fatigue strength had been applied on the Rod due to the loosening of the joint of the Rod and the yaw actuator and the stiffening of the ball pivot as well as a resonance phenomenon following the stiffening. As to the stiffening of the ball pivot, it is considered highly probable that the phenomenon had occurred because red rust created with the corrosion of the contact surface of the inner ring and the outer ring caused volume expansion in the space between the two rings and this restricted the movement of the two rings.
In relation to survivability:
…it is considered highly probable that because the captain had not fastened the shoulder harness, his body bent forward due to the impact at the time of the crash and his heart was damaged as he had his chest hit with the cyclic stick.
Other Safety Resources
Aerossurance has previously written on these associated topics:
Airworthiness Matters: Next Generation Maintenance Human Factors Over the last 10-15 years, much attention has been focused on maintenance human factors training and reporting & investigating errors. While we could concentrate on simply doing more of these and certainly can find ways to do these things better, perhaps the next generation approach needs to include a much wider range of activities.
Aircraft Maintenance: Going for Gold? Should we start treating maintenance personnel more like athletes who need to achieve peak performance every day?
UPDATE 30 March 2019: Contaminated Oxygen on ‘Air Force One’ Poor standards at a Boeing maintenance facility resulted in contamination of two oxygen systems on a USAF Presidential VC-25 (B747).
UPDATE 12 October 2019: ATR72 VH-FVR Missed Damage: Maintenance LessonsUnclear communications, shift handover & roles and responsibilities, complacency about fatigue and failure to use access equipment all feature in this serious incident.
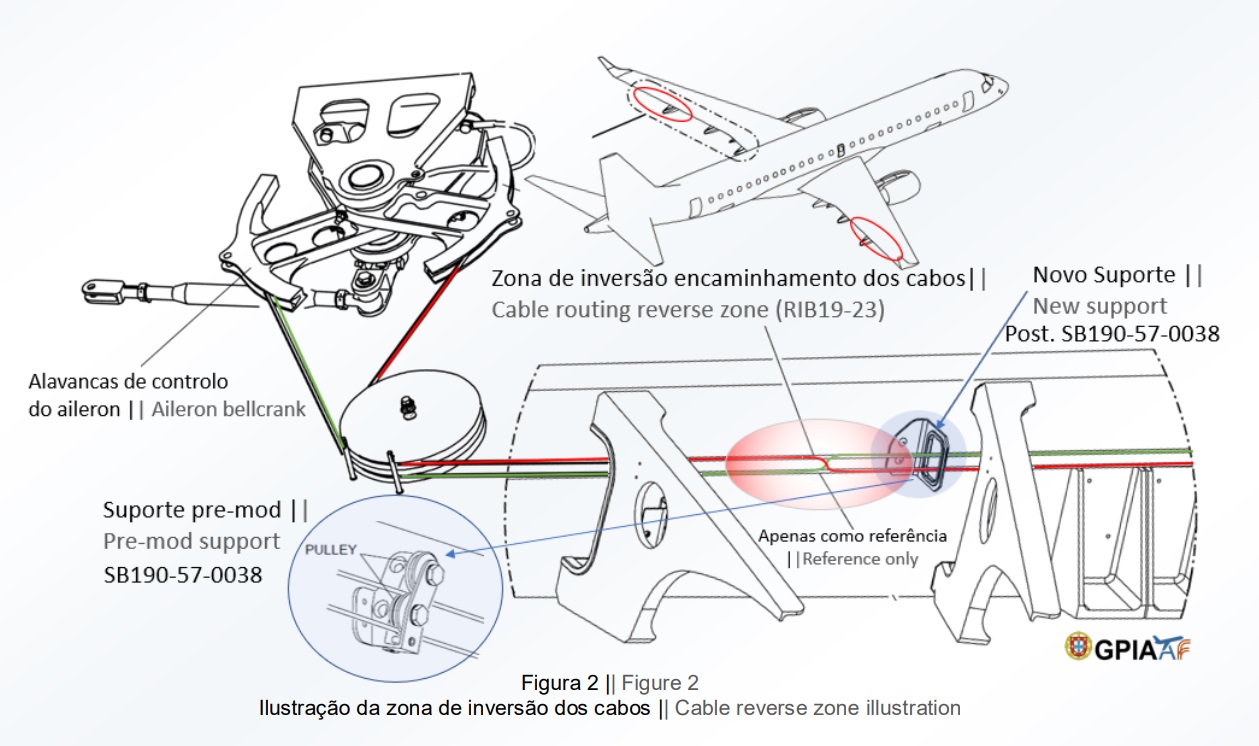
UPDATE 31 May 2019: The Portuguese accident investigation agency, GPIAAF, issued a safety investigation update on a serious in-flight loss of control incident involving Air AstanaEmbraerERJ-190P4-KCJ that occurred on 11 November 2018. The aircraft was landed safely after considerable difficulty, so much so the crew had debated ditching offshore. GPIAAF conformed that incorrect ailerons control cable system installation had occurred in both wings during a maintenance check conducted in Portugal.
Misrigged Flying Control Cable, Air Astana Embraer EJ-190 P4-KCJ (Credit: GPIAFF)
GPIAFF note that: “By introducing the modification iaw Service Bulletin 190-57-0038 during the maintenance activities, there was no longer the cable routing and separation around rib 21, making it harder to understand the maintenance instructions, with recognized opportunities for improvement in the maintenance actions interpretation”. They also comment that: “The message “FLT CTRL NO DISPATCH” was generated during the maintenance activities, which in turn originated additional troubleshooting activities by the maintenance service provider, supported by the aircraft manufacturer. These activities, which lasted for 11 days, did not identify the ailerons’ cables reversal, nor was this correlated to the “FLT CTRL NO DISPATCH” message.”
GPIAFF comment “deviations to the internal procedures” occurred within the maintenance organisation that “led to the error not being detected in the various safety barriers designed” in the process. They also note that the error ” was not identified in the aircraft operational checks (flight controls check) by the operator’s crew.”
Aerossurance worked with the Flight Safety Foundation (FSF) to create a Maintenance Observation Program (MOP) requirement for their contractible BARSOHO offshore helicopter Safety Performance Requirements to help learning about routine maintenance and then to initiate safety improvements:
Aerossurance can provide practice guidance and specialist support to successfully implement a MOP.
Aerossurance has extensive air safety, operations, airworthiness, human factors, aviation regulation and safety analysis experience. For practical aviation advice you can trust, contact us at: enquiries@aerossurance.com