S-92A Night Approach Mode Awareness Incident (PHI Sikorsky S-92A VH-IPE)
On 1 February 2025 PHI International Sikorsky S-92A VH-IPE suffered an incident on a night approach to the Transocean Endurance mobile drilling unit (MODU), 38 NM NNW of Exmouth, Western Australia.
The helicopter descended as low as 191 ft above the sea according to the Australian Transport Safety Bureau (ATSB) who issued their safety investigation report on 4 February 2026.
Purpose of the Flight, the Crew, Flight Planning & Crew Coordination
At Exmouth offshore transport flights are daytime only but flight crew are rostered on standby for night medevacs. The helicopter had departed Exmouth for a routine night recency flight at 19:18 Local Time, 15 minutes before last light.
The aircraft commander had 10,240 hours total experience (1,100 at night), 3,530 in multi-engine helicopters. They had 299 hours on type (13 at night). Their 13 S-92A night hours…
…were a combination of simulator assessments and their initial 5‑night helideck landings…on 2 November 2024…
The co-pilot had 5,360 hours total experience (1,240 at night), 2,390 in multi-engine helicopters. They had 224 hours on type (9 at night). They…
…had last flown at night on 14 December 2024 during their initial night helideck landings under supervision.
Both these pilots had flown the Leonardo AW109 for marine pilot transfer (MPT).
The operator’s…
…rostering policy for flight crew minimum experience reflected the guidance of the International Association of Oil and Gas Producers [IOGP] for offshore helicopter operations, which stated: …co-pilots with less than 500 hours offshore multi engine and multi-crew should not be rostered with any commander who has less than 100 hours PIC since command appointment on the contracted type.
While the commander had <100 hours of S-92A command of the S‑92A, the copilot’s offshore multi-engine helicopter experience exceeded the requirement to be paired with a commander with more experience on type, albeit in a light twin doing MPT. ATSB observe that:
No additional rostering restrictions were identified in either the IOGP guidance or the operator’s policies for flight crews experience for pairing crew night.
During flight planning an “operational risk assessment is conducted”. The operator used a software tool that “generated a risk level for the flight”.
The completed risk assessment indicated a ‘caution’ risk due to the crews’ experience on the aircraft type and flight at night. The crew recorded that they had discussed the risks involved with their inexperience and night flight during the sortie planning. The captain also stated that as this was their first flight back following an off-duty period they took additional time to go through pre-flight checklists recalling they did not want to rush.
The aircraft commander was the pilot flying (PF), in the right seat and the copilot was the pilot monitoring (PM) in the left seat. A third pilot was sat in the cabin on the transit out.
The purpose of the flight was for each pilot to conduct 3 take-offs and landings so the crew would remain current in case of a night medical emergency evacuation…
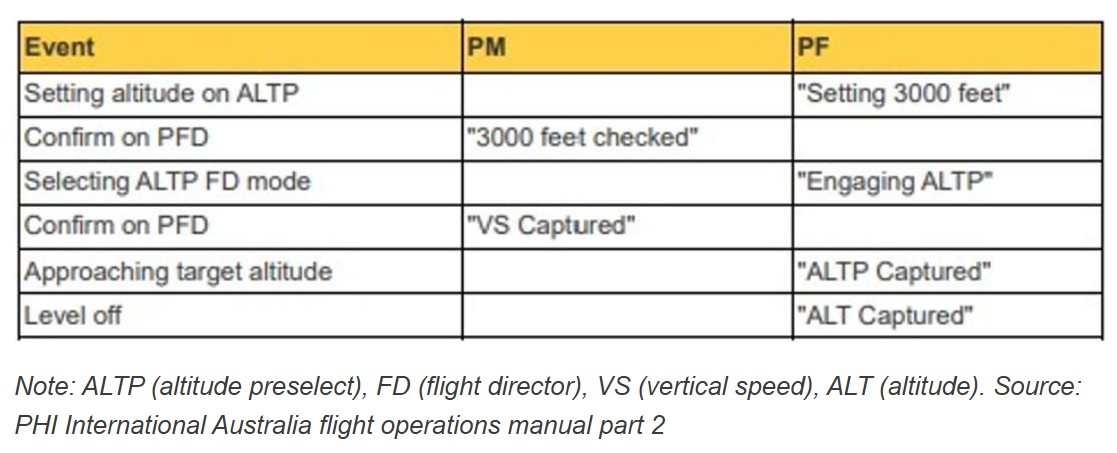
The ATSB explain that the operator’s Flight Operations Manual Part 2 (FOM 2) stated that:
Operating procedures have been developed to achieve the optimum use of both pilots. Many duties may be carried out by either pilot, depending upon which one at the particular time has spare capacity. However, system handling by the PF should never interfere with their main task of flying the aircraft. Particular attention must be given to good crew co-ordination during all phases of flight. A crew briefing must be completed prior to every take-off, approach and landing. Normally the crew briefing will be given by the PF.
The FOM 2 detailed the operator’s checklist philosophy:
Crews should operate the aircraft, which includes changing the configuration and setting up systems, using the “next event” activity cycle, based around the priorities of “Aviate – Navigate – Communicate – Administrate [ANCA]”.
The NCL [normal checklist] should be used as the mechanism to confirm that the required actions have been completed and the aircraft is configured correctly for the task ahead. Crews should avoid flying the aircraft by checklist.
It is important to ensure that the flight director modes have been selected, armed and captured correctly. Both crew members should be actively involved in this process.
ATSB observe that:
When the PF performs the ‘action’, the PM is required to check and confirm the status of the actions.
FOM 2 also stated (a little clunkily):
During all operations, the priority role of the PM is to monitor the PF, especially below 1000′, and not be distracted from the task. Reference to checklists, navigation logs or other manuals is not to be made during these critical flight phases. Essential drills, type specific, may be completed with due consideration for the monitoring tasks.
The Descent
On receiving…updated weather information from the rig, the PM intended to calculate the take-off safety speed (Vtoss) for landing. Vtoss is used by the operator as a minimum target speed in the event [of an engine failure on approach]…and is required to be set as part of the approach briefing.
Use of the Sikorsky performance application was described as “delayed” and “rushed” leading to low confidence in the output, so:
…the crew agreed to use 45 kt, based on their previous experience in the S‑92A, with the intention of recalculating the speed when time permitted.
By now it was 19:33 and the helicopter was…
…11 NM south-east of the drill rig and now in darkness. [and] the helicopter began a descent to the lowest safe altitude of 1,500 ft.
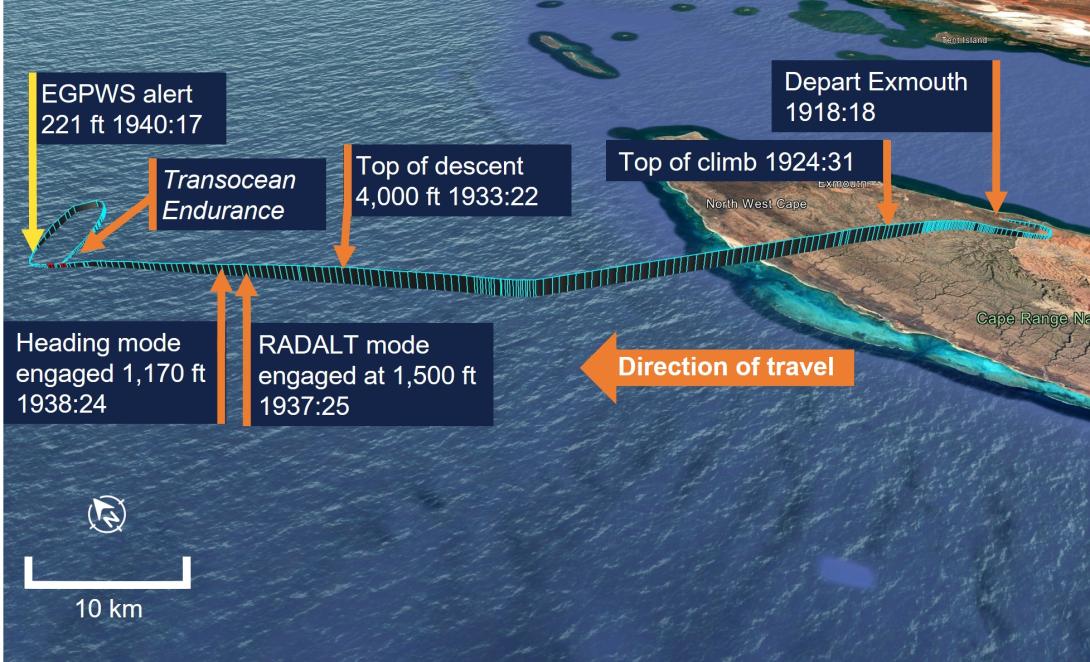
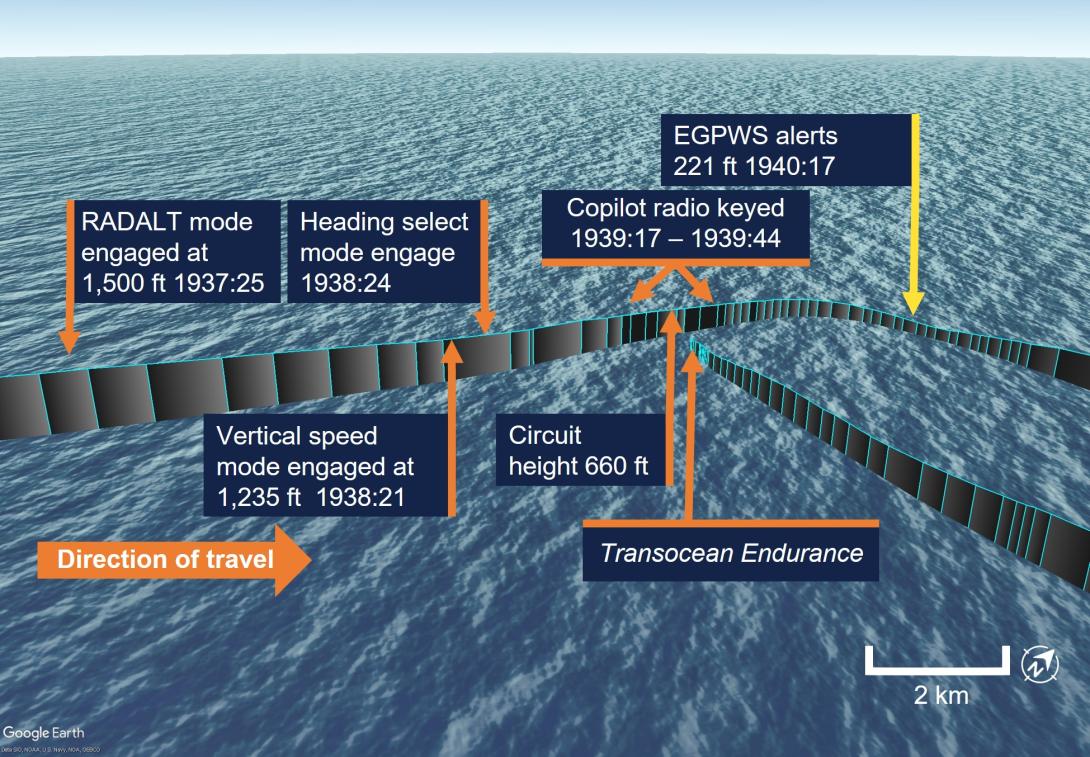
At 19:37, the PF requested the PM to engage the [automatic flight control system (AFCS)] radar altimeter (RADALT) hold mode and lower the target altitude capture height to the 660 ft circuit height.
There are two AFCS mode select panels in the lower middle of the S-92A instrument panel.

The ATSB report describes how there are adjacent rows of ‘hard keys’, with dedicated functions and ‘soft keys’ whose function depends on the menu selected on the panel. The upper hard mode keys illuminate when selected. In contrast the lower hard menu keys have an illuminated surround.
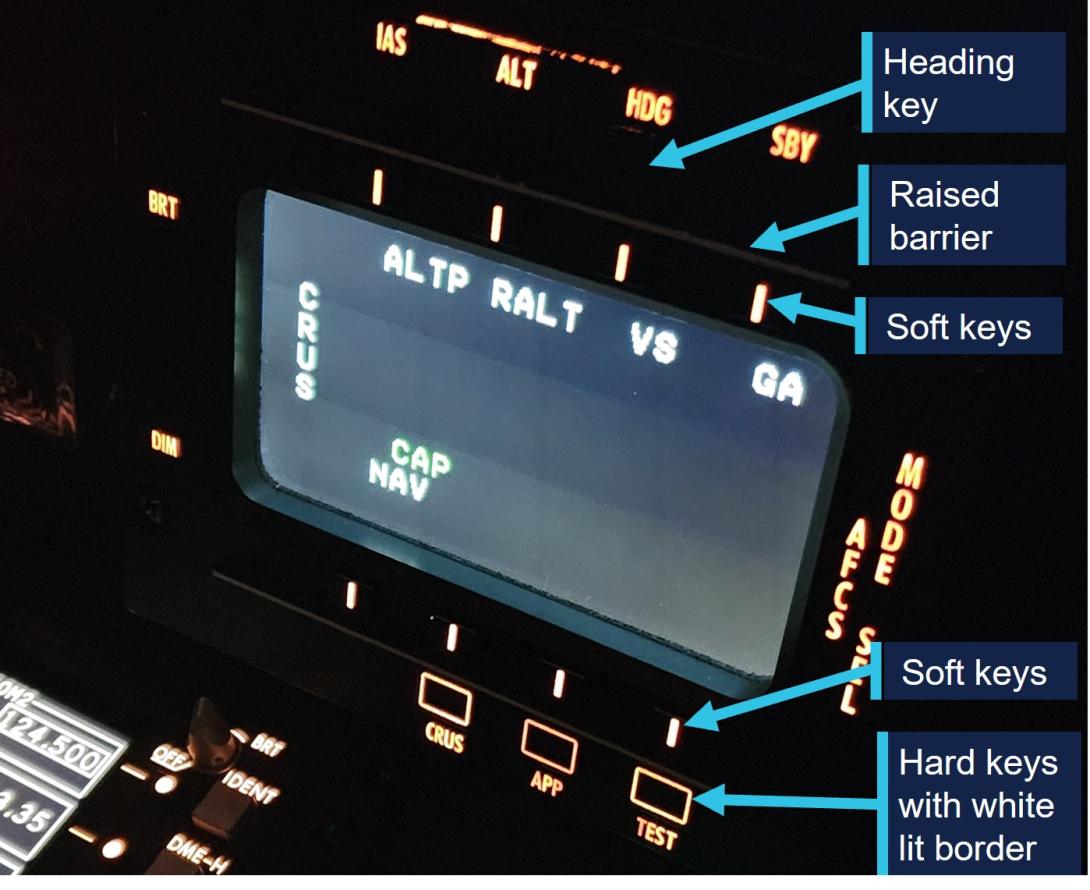
A later design of panel (“likely due to customer feedback”)…
….was upgraded to incorporate two white coloured finger barriers above and below the display screen between the rows of hard and soft keys [that] gave pilots tactile feedback on finger position in relation to the rows of hard and soft keys.
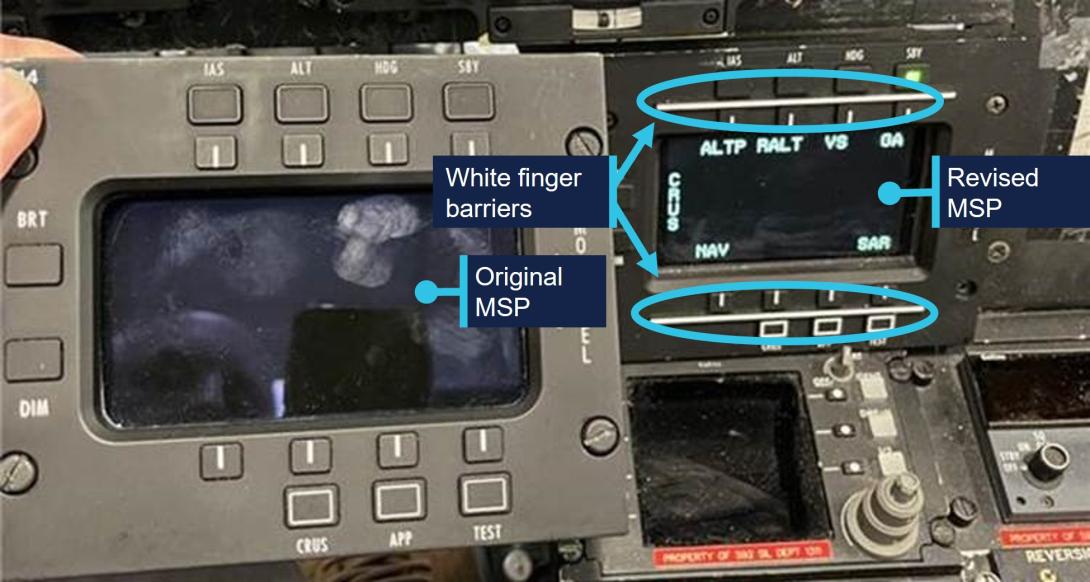
The active modes are shown at the top of each pilot’s primary flight display (PFD).

The letters P (Pitch), R (Roll), and C (Collective)…correspond to the autopilot axis controlling each mode. The system does not provide audible tones or display alerts when a mode is changed or immediately captured.
The RADALT hold mode selection by the PM (who had older build standard of panel) was via a soft key….
…was confirmed by the PM and the helicopter commenced a further descent to the drill rig circuit height.
ATSB are ambiguous but this appears to mean that the PM verbally confirmed doing the selection, but without mode verification from the PFD by the PF as required.
Both flight crew later recalled completing the before landing checklist during the descent.
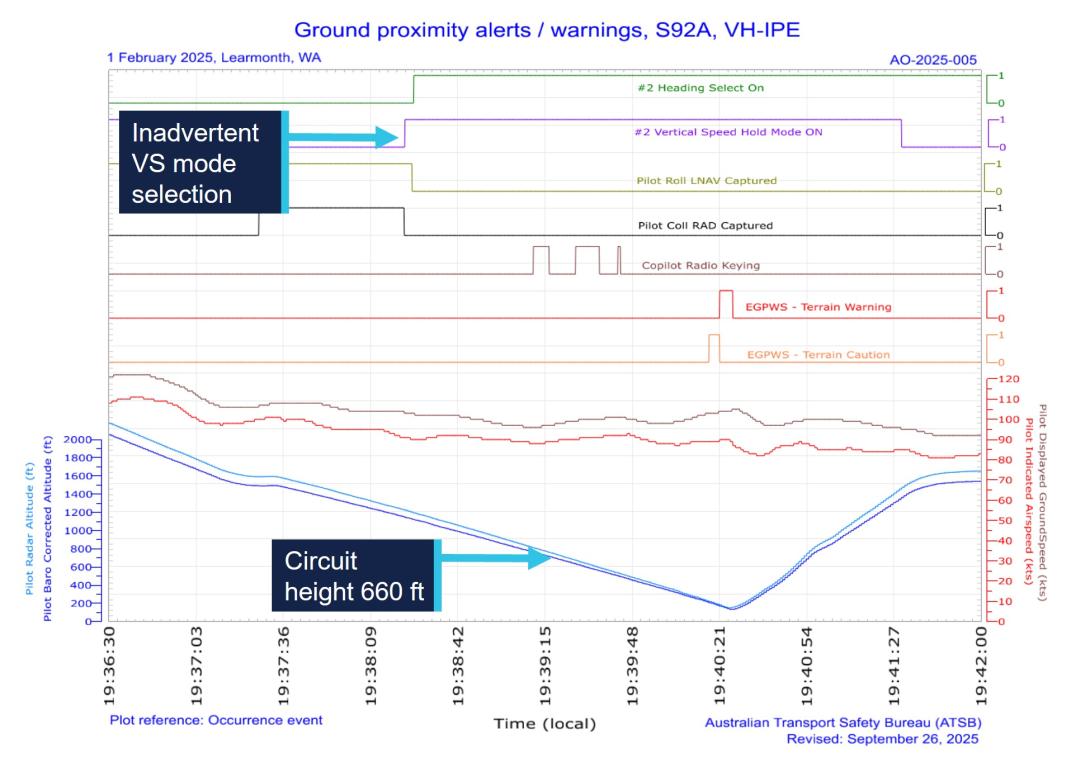
At 19:38:21 and about 1,235 ft, during the descent for a visual approach to the rig, the PF attempted to select the heading mode on the AFCS mode select panel to adjust the heading and avoid flying directly over the rig.
While attempting to press the heading mode button [an upper hard key], the PF inadvertently and unknowingly selected the vertical speed button which was directly below it.
This mis-selection was done by the PF, who had the improved standard of panel. Crucially this unintended selection meant that:
The inadvertent selection of the vertical speed hold mode captured the helicopter’s 500 ft per minute rate of descent, and cancelled the RADALT hold mode that would have levelled the helicopter at a preset circuit height of 660 ft above sea level.
The PF noticed the heading button on the AFCS panel was not lit, indicating it was not engaged and presumed the original selection had not registered on the first attempt and reselected the heading mode key.
This second attempt occured within 3 seconds as:
Heading hold mode was engaged at 1938:24, at about 1,200 ft. The PF later recalled confirming the selection with the PM.
Again the ATSB text suggests that the PM did not verify that selection by reference to the PFD.
The crew reported that some residual terrestrial light remained as they approached the rig and allowed them to see the ocean and recalled the wind conditions to be calm with no white caps.
The Circuit
The Transocean Endurance helideck height is 109 ft.
The operator’s helideck approach guidance indicated a 1,500 ft height for minimum safe altitude above the rig and that the circuit height was 660 ft above mean sea level.
![]()
ATSB explain that:
At 19:39:00, the helicopter joined a crosswind leg to conduct a right circuit to the rig. This was so the PF could keep the rig visible from their side of the helicopter. While on the crosswind leg, the PM’s radio was keyed several times.
During this time, both crew were unaware that the helicopter had continued descent through the preset circuit height of 660 ft.
At 19:39:46 and about 500 ft, the PF commenced a turn onto the downwind leg of the circuit and later stated they were certain the helicopter had levelled at the circuit height.
At this point PM and PF both became engaged in other activities. Firstly:
The PF then requested the PM to check the Vtoss for landing, later stating that they thought the estimated speed was too high. This required the PM to use the electronic flight bag (EFB).
Secondly the PF…
…began to manoeuvre the helicopter searchlight [a 450W light additional to two 450W landing lights] which required them to visually identify that the beam was in the desired direction.
The operator’s before landing checklist required the landing lights to be selected ‘On’, although there was no requirement for the use of the searchlight for landing in the operator’s checklists. The PF reported that the use of the searchlight was, in the event of a water ditching, to assist the flight crew to visually identify the water’s surface…
The PF…had difficulty finding the searchlight beam due to reflection on the water from the well-lit rig, and therefore setting the beam in the right position took longer than expected.
Then:
At 19:40:17 and 221 ft, the crew received an EGPWS [Honeywell MKII enhanced ground proximity warning system] terrain caution alert and at 19:40:21 and 181 ft, this was followed by a terrain warning alert.
The crew reacted to the alerts and initiated an emergency climb to the minimum safe altitude of 1,500 ft.
At 19:40:25 the helicopter had descended to its lowest height of 152 ft before climbing.
Debrief and Continued Operations
The crew concluded incorrectly that the unintended descent was a result of the PF accidently adjusting the RADALT target height; the trim switch is in close to the searchlight slew toggle switch on the collective.
The crew were comfortable to complete the planned flying and returned to Exmouth without incident, landing at 22:08.
ATSB Human Performance Discussion
ATSB include a generic human performance discussion that includes:
Workload represents the level of mental and physical demand placed on an individual by the operational environment and the nature of the task.
High workload may lead to errors when task demands exceed the available cognitive or physical resources. As task demand increases beyond certain limits, performance declines even though an individual’s effort may rise.
Expectations strongly influence where a person will search for information and what they will search for (Wickens & McCarley, 2008), and they also influence the perception of information (Wickens, Hollands, Banbury, & Parasuraman, 2013).
Our Own Human Factors Observation
We would be tempted to also highlight astudy by R. Key Dismukes & Ben Berman “Checklists and monitoring in the cockpit: Why crucial defenses sometimes fail” (NASA Technical Memorandum Report No. 2010-216396). This observation based study, highlighted cases where “a pilot either responded verbally to a challenge item [of a checklist] without visually inspecting the item, responded verbally before inspecting the item or responded that the item was correctly set when in fact it was not. In some cases [they] may actually have been instances of ‘looking without seeing'”.
Expectation that an item is correctly set arises from memory of having just set or checked an item and from the vast number of previous instances in which that item has been correctly set. Thus, even though the pilot may direct gaze toward the item to be checked, he or she may perceive it to be in the correct position even when it is not, especially if gaze fixation on the item is brief due to rushing. Also, it is possible that pilots’ response to the checklist challenge may become so automatic that pilots sometimes utter the response automatically, perhaps not even realizing that they have not visually confirmed the challenged item.”
Summary of ATSB Analysis
During interviews conducted with the ATSB…both flight crew reported they believed their total time and time at night flying the S‑92A likely affected their familiarity with the cockpit and efficiency completing administrative tasks.
The combination of the [short] flight time and the PM’s experience on the helicopter type, resulted in them being rushed to complete the take-off safety speed (Vtoss) calculation prior to the top of descent.
The PF’s low familiarity with the helicopter type at night likely created an unfamiliar cockpit environment which was compounded by their lack of recency, following a 4-week period off duty. In a complex cockpit environment such as the S‑92A this increased the risk of a selection error.
The PF…
…mistakenly selected the vertical speed key before then reselecting the heading key. The inadvertent selection of the vertical speed mode went unrecognised by the crew.
This was consistent with an unintentional slip.
Both the heading and vertical speed keys are physically close, located one above the other. Further, as the top row of hard keys were not backlit when the mode was not engaged, identification of the correct key is more difficult in a dark cockpit, especially for flight crew who had limited experience flying the S‑92A at night.
Next the ATSB state that the “PF confirmed with the PM that the engagement of the intended heading mode was correct”. However, crucially the vertical speed mode was selected. The ATSB do not identify that confirmation as erroneous or consider that check further (but we will; see Our Observations below).
The helicopter continued a 500 feet per minute rate of descent that was not recognised by the crew in the mostly dark conditions. The reduced visual reference when combined with the preoccupation of additional tasks resulted in the helicopter’s continued descent until the crew reacted to the EGPWS alert.
Although uncommented upon by ATSB, more modern types have AFCS protections in such circumstances (see Our Observations below).
While the PF requested the PM to calculate the Vtoss for landing, they also diverted their own attention to activating and manipulating the searchlight beam outside the helicopter. Consequently, neither flight crew member was monitoring the helicopter’s altitude which contributed to the unidentified descent below the circuit height, triggering a ground proximity alert.
ATSB contend that the pre-flight ‘operational risk assessment’ “did not capture the risk of the crew’s limited experience on type at night”, even though they previously said it ” indicated a ‘caution’ risk” and consider this to be the one ‘safety risk’ emergent from this incident.
PHI Safety Actions
Subsequently PHI implemented the following procedures:
- All initial approaches during night flight to be conducted as an instrument approach, which ensures a more structured process with procedural barriers.
- Night recency flights not to be conducted on a first flight back following any pilots leave.
- Radar altimeter alert to be set at 500 ft.
PHI also:
…increased the risk loading on its operational risk assessment for pilots with less than 500 hours on type.
Night flights with both pilots with less than 500 hours on type at night now require discussion with the senior base pilot regarding the additional risks relating to inexperience on type.
The S‑92A cockpit lighting environment was reviewed by the operator with subject matter experts to consider if an engineered improvement was practicable.
This is an interesting aspect as the S-92A’s cockpit lighting was discussed in a 2017 SAR accident report.
A procedural change was implemented…that required the use of small lights that are worn on the pilot’s fingers to improve visibility of the cockpit environment (such as switches, buttons, and controls) during S‑92A night flights.
PHI reported that:
…lessons from this occurrence have been shared and promoted both internally and externally. These efforts included an internal safety alert and a ‘learning from occurrence’ video detailing what happened and why to the international community through industry body HeliOffshore.
Operational procedures regarding multi-crew cooperation, automation mode changes/awareness, and EGPWS alerts were highlighted to all flight crews through internal communications. These points were also highlighted within the training and competency teams as focus areas during both simulator and line training sessions.
Our Observations
While night operations where both pilots have <500 hours night experience “now require discussion with the senior base pilot” at PHI, its worth highlighting that in a regions with relatively little night flying, most crews will have less night experience than that if they are mostly doing a few hours of recency flying every 90 days. So such “discussions” will be common.
A crucial defence against an incorrect mode selection is crosschecking what was set after selections are made. The Operator’s standard callouts assume the PF would set the AFCS mode, verbalising this, and the PM would specifically check the mode displayed on the PFD. This does not appear to have happened (the PM merely acknowledging the PF’s call out). Hopefully the action taken on “automation mode changes/awareness” has emphasised the PFD mode display being checked and verbalised by the PM.
More modern types benefit from AFCS logic that would reduce the commanded rate of decent close to the surface.
If regulations and industry recommended practices establish prescriptive criteria for rostering crew members together it is perhaps optimistic to expect an ‘operational risk assessment’ to have more restrictive criteria. As most such tools are pretty crude and uncalibrated, at least in this case at least it identified an elevated risk when after most accidents other examples of such tools remained at a low risk.
We have seen comment on social media by a salesman for a proprietary ‘pilot line observation programme’ using cameras (rather than having an on-board observer like the established LOSA approach) that implied their proprietary approach would have detected ‘errors’ made in this occurrence, presumably before any incident. We’d observe that:
- There would need to be a high sampling rate on the relatively rare night recency flights to give a reasonable probability of detection of night specific issues.
- Detecting if PMs are looking at the PFD before confirming mode selection is difficult to do. Actions that appear conform to procedures, albeit weak procedures, are thus less likely to be identified as problematic.
Safety Resources
The European Safety Promotion Network Rotorcraft (ESPN-R) has a helicopter safety discussion group on LinkedIn. You may also find these Aerossurance articles of interest:
- AW139 Loss of Control Climbing Away from SAR Exercise
- Night Offshore Take-Off Loss of Control Incident Norway
- North Sea Helicopter Struck Sea After Loss of Control on Approach During Night Shuttling (S-76A G-BHYB 1983)
- Night Offshore Helicopter Approach Water Impact
- Loss of Sikorsky S-76C+ 5N-BQG of Eastwind Off Nigeria 24 October 2024
- 29 Seconds to Impact: A Fatal Night Offshore Approach in the Irish Sea
- S-76D Loss of Control on Approach to an Indian Drilling Rig
- Fatal Taiwanese Night SAR Hoist Mission (NASC AS365N3 NA-106)
- Air Ambulance Helicopter Struck Ground During Go-Around after NVIS Inadvertent IMC Entry
- A HEMS Helicopter Had a Lucky Escape During a NVIS Approach to its Home Base
- SAR Helicopter Loss of Control at Night: ATSB Report
- Night HEMS BK117 Loss of Control
- HEMS A109S Night Loss of Control Inflight (N91NM)
- Air Ambulance A109S Spatial Disorientation in Night IMC (N11NM)
- HEMS Black Hole Accident: “Organisational, Regulatory and Oversight Deficiencies”
- HEMS S-76C Night Approach LOC-I Incident
- Drift into Danger: AW109SP Night HLS Accident
- ‘Procedural Drift’: Lynx CFIT in Afghanistan
- US Fatal Night HEMS Accident: Self-Induced Pressure & Inadequate Oversight
- HEMS Black Hole Accident: “Organisational, Regulatory and Oversight Deficiencies”
- Taiwan NASC UH-60M Night Medevac Helicopter Take Off Accident
- Italian HEMS AW139 Inadvertent IMC Accident
- Dim, Negative Transfer Double Flameout
- BK117B2 Air Ambulance Flameout: Fuel Transfer Pumps OFF, Caution Lights Invisible in NVG Modified Cockpit
- HEMS Black Hole Accident: “Organisational, Regulatory and Oversight Deficiencies”
- EC135P2 Spatial Disorientation Accident
- EC135P2+ Loss of NR Control During N2 Adjustment Flight
- Austrian Police EC135P2+ Impacted Glassy Lake
- That Others May Live – Inadvertent IMC & The Value of Flight Data Monitoring
- HEMS S-76C Night Approach LOC-I Incident
- CHC Sikorsky S-92A Seat Slide Surprise(s)