Cold Comfort Conference Call: USAF F-35A Alaska Accident
On 28 January 2025 US Air Force Lockheed Martin F-35A 19-5535 of the 355th Fighter Squadron crashed and was destroyed at Eielson Air Force Base (AFB), Alaska (a total loss valued at $196.5 mn). The pilot ejected and suffered only minor injuries.

F-35A Lightning II during Red Flag Alaska 25-3 at Eielson AFB, AK, 25 July 2025 (USAF Stock Photo: Credit Senior Airman Alexzandra Gracey 354th FW)
The USAF released their Accident Investigation Board (AIB) report on 26 August 2025.
A USAF AIB does not conduct a safety investigation (a separate Safety Investigation Board [SIB] is convened but their report is not released publicly), instead (our emphasis added):
In accordance with AFI 51-307, Aerospace and Ground Accident Investigations, this accident investigation board conducted a legal investigation to inquire into all the facts and circumstances surrounding this Air Force aerospace accident, prepare a publicly-releasable report, and obtain and preserve all available evidence for use in litigation, claims, disciplinary action, and adverse administrative action.
The Accident Flight
A Landing Gear Fault After Take Off
The accident aircraft was number 3 of a flight of four 355 FS F-35As, callsign YETI, that was to conduct an Air Combat Maneuvers (ACM) sortie with two other F-35As, callsign CHEVY. The 355 FS is part of the 354th Fighter Wing (354 FW).
The pilot of YETI 3 was a current F-35A evaluator and instructor pilot with 2702 hours in total (555 hours on type).
Shortly after takeoff, the pilot of YETI 3 received an OVERSPEED GEAR caution. They identified that instrumentation showed yellow and black hash marks for the Nose Landing Gear (NLG) that indicated ‘gear in-transit’. Their wingman reported the NLG door was “open by about 2 inches”.
The pilot followed the necessary checklists, which included lowering the gear and conducting flight control system resets. The NLG was initially angles c25 degrees left. This was reduced to c17 degrees during this fault finding.
Calling a ‘Conference Hotel’: Fault Finding Technical Support Call with Lockheed Martin
The pilot then requested a ‘Conference Hotel’, namely a conference call with Lockheed Martin engineers. This was swiftly organised through the on-duty Supervisor of Flying (SOF) at Eielson AFB. Although the AIB don’t say when this call was requested it appears to have been set up in less than 20 minutes. On the call were the Eielson SOF, a “senior 354 Operations Group (354 OG) leader” and 5 Lockheed Martin engineers (a senior software engineer, a flight safety engineer and three landing gear systems engineers). The Eielson SOF was in turn in contact with the pilot.
According to the AIB report the engineers…
…requested information on, among other things, how much fuel the MA [Mishap Aircraft] had remaining, direction of the NLG wheel, and health reporting codes [HRCs].
The AIB then says that they…
…did not request or receive information about where the mishap was occurring and ambient air temperature.
That’s an odd observation because presumably they did know the call was arranged by the Eielson SOF, that Eielson AFB is in Alaska and that in January Alaska is rather chilly…!
Initially an arrestor landing was mooted, but the pilot pointed out that “cable arrestment must be in a 3-point attitude” according to the published procedures, meaning the NLG would have to be on the ground prior to the cable engagement. That course of action was abandoned because of the concern that an uncentered nose wheel could result in aircraft rollover or runway departure.
An alternative was then suggested, namely a touch-and-go to see if cycling the Main Landing Gear (MLG) Weight on Wheels (WoW) sensors would straighten the nose wheel.
Both main gear WoW sensors are plunger-type sensors actuated by keeping physical contact with the landing gear torque arms integral cam.
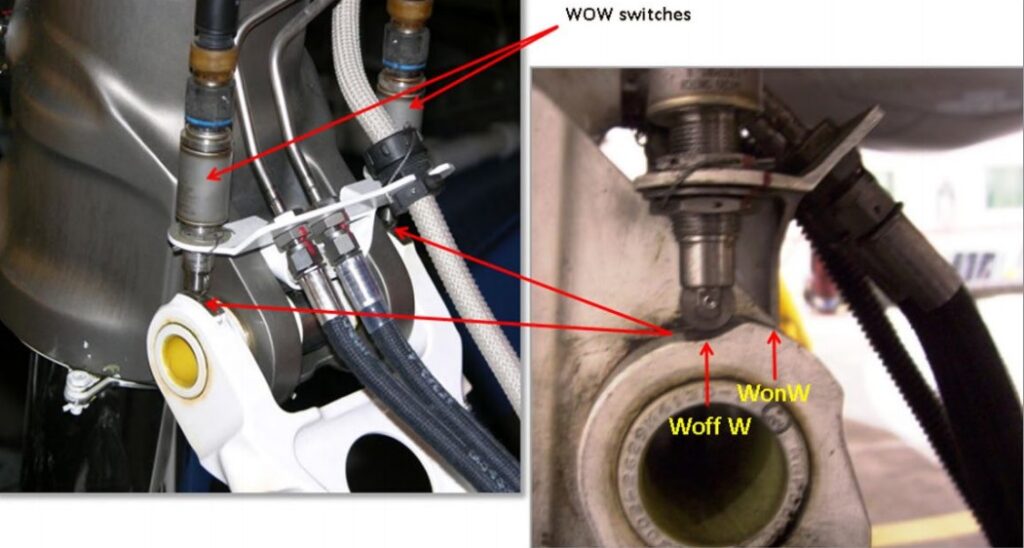
F-35A MLG WoW Sensors (Credit: USAF AIB)
The pilot then proposed a touch-and-go at a higher speed with the NLG contacting the runway (presumably to try to shock the NLG straight). However, the SOF radioed the pilot:
Alright the engineers uh are not optimistic about this COA [Course of Action] but, extremely low PK [probability kill, meaning the probability this would fix the issue], but we’re going to try anyway is a touch-and-go on the runway, mains only, do not touch the nose gear, uh lift back off in all cases and have the uh have Yeti 4 reconfirm the nose gear position once your safely airborne.
The SOF further explained the engineers believed some sort of mechanical malfunction with the nose wheel was causing these issues; this is because under normal circumstances it is impossible for the nose wheel to be stuck canted off at an angle when the gear is extended.
The engineers suspected, based on their experience, that the NLG centering cam was jammed but were uncertain as to the why.
Touch-and-Go 1
The first touch-and-go, less than an hour after take off, did not result in a change to the NLG angle. However the pilot informed the SOF that there were 5 new HRCs including ones relating to the MLG and the WoW sensors.
There then appears to be a inconsistency in recollection between the parties on the call. The AIB initially state that…
The Lockheed Martin engineers “wanted to know about the nose wheel HRCs” and “did not seem nearly as concerned about the other landing gear HRCs”.
It is unclear in the AIB report but they appear to be quoting the SOF. In contrast the Senior OG Leader recalled the engineers were given all 5 HRCs and…
…went line by line . . . with each one” of the HRCs “and then tried to match it to the scenario” with the aircraft.
Whereas the Lockheed Martin engineers say they received 3 codes, all NLG related.
The AIB say that a FCS FAULT was annunciated due to “failures of the Right MLG
WoW Switch 1 and Switch 2″. The pilot did not have a indication as to the cause of the FCS FAULT.
The MA Helmet Mounted Display (HMD) and Panoramic Cockpit Display (PCD) recording showed no HRC for FCS in the Prognostics and Health Management (PHM) page, and the checklist does not indicate all of the reasons that the FCS FAULT advisory could annunciate.
The pilot initiated an FCS/ENG RESET but the FCS FAULT advisory returned.
The pilot was not aware that the right MLG struct had not fully extended after the touch-and-go. Video recorded by his wingman confirms it was only partially extended, but the pilot of that aircraft had not noticed it. The AIB do not comment but possibly this is because of focusing on the NLG position.
Touch-and-Go 2
After further discussion on the conference call it was agreed to try the pilot’s earlier suggestion of a faster touch-and-go on all three gear.
Recorded FLIR video from the wingman’s aircraft showed both the MLG and NLG touching down on the runway during the second touch-and-go at 21:48:15Z. The nose wheel went from 17 degrees left to 6 degrees left
The pilot of the mishap F-35A momentarily selected Maximum Afterburner (MAX ETR) and the aircraft lifted off the runway at 21:48:24Z. Eight seconds later the pilot conducted an FCS/ENG RESET.
Loss of Control and Ejection
Four seconds later, at 21:4836Z, while climbing away, the aircraft “began to experience significant oscillations in the yaw axis followed by oscillations in the pitch axis” which the pilot tried to counteract before selecting MAX ETR at 21:48:41Z.
Two seconds later the pilot attempted to initiate a left bank. The aircraft rolled to the left and “aggressively pitched up “.
The control stick inputs were neutralized at 21:48:43Z, indicating the pilot released his hand from the stick. And at 21:48:44Z, the pilot commanded an ejection.
According to the Martin-Baker analysis report, the ejection occurred at approximately 620ft AGL at an airspeed of 222 KCAS. The aircraft was pitched up 30-40 degrees pitch up and in a 38-degree left bank.
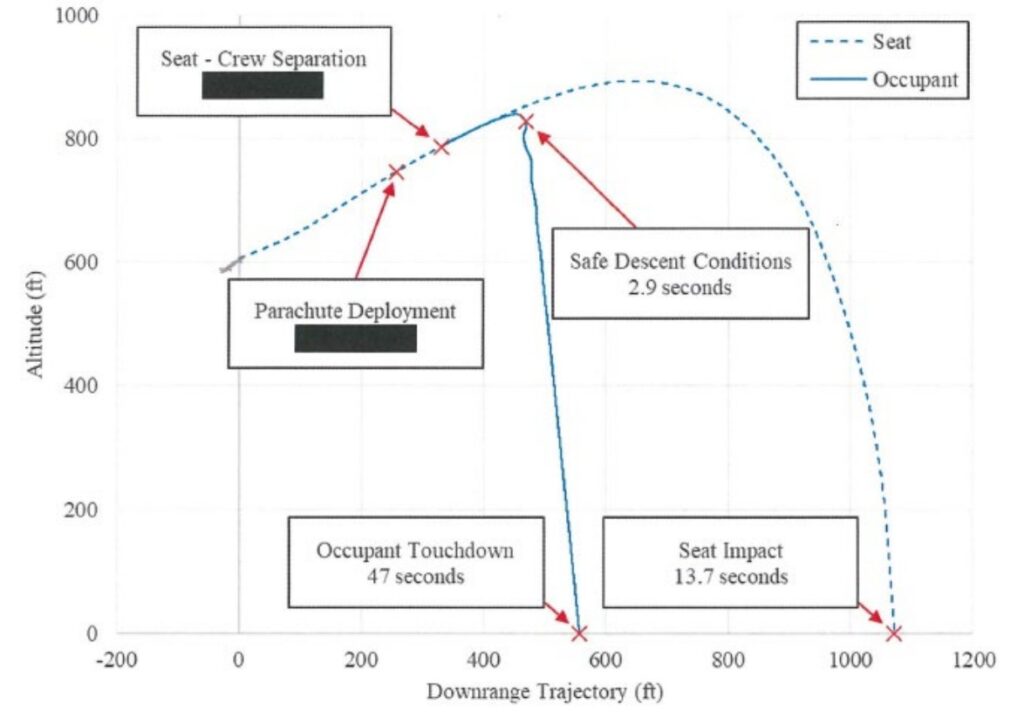
MB US16E Ejection Seat Trajectory (Credit: Martin-Baker via USAF AIB)

Marin-Baker US16E Ejection Seat Trial on the Rocket Sledge at Langford Lodge (Credit: MBA)
The aircraft continued an upward trajectory to 2,665 AGL before stalling, impacting the
ground in a 116-degree right bank at 21:49:16Z.
The Accident Investigation
Prior Maintenance: Water Contamination of Hydraulic Fluid
The Autonomic Logistics Information System (ALIS) is a program used by F-35 Maintenance
personnel to document servicing, inspections, aircraft configuration, status and houses Joint
Technical Data (JTD) used to maintain the aircraft to manufacturer specifications.
A Landing Gear Fluid Servicing was completed on 25 January 2025 to comply with a 200-hour check.
This maintenance action is completed by depleting the pneumatic pressure as well as flushing the hydraulic fluid from the landing gear struts.
The Air Force Research Laboratory (AFRL) tested the hydraulic fluid from the three landing gear stuts after the accident and shockingly “found that approximately one-third of the fluid retrieved from the Right MLG and NLG was water”.
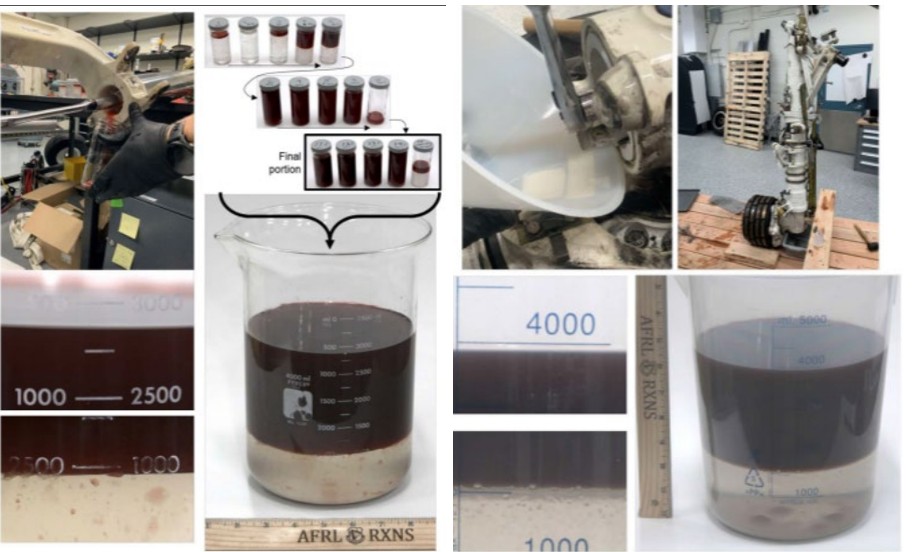
Left: 1L of Water Found in 2.8L of NLG Hydraulic Fluid & Right: 1.5L of Water Found in 4L of MLG Hydraulic Fluid (Credit: AFRL via USAF AIB)
The hydraulic fluid was from a barrel in the 355th FGS support section and had been put into a hydraulic servicing handcart to service the F-35A.
Investigators tested the barrel and servicing cart for contamination using a Portable Oil Diagnostics System (PODS). This showed both failed to meet the applicable Society of Automotive Engineers (SAE) standards for hydraulic fluid. Both had more than 1024 parts per million (ppm) of particulates, more than double the allowable level. The test does not accurately measure contaminates above 1024ppm, so the contamination was “potentially far greater”.
Hydraulic fluid is controlled by the 355th FGS hazardous materials (HAZMAT) program. The AIB report then states that this
…program suffered from insufficient manning and frequent supervision changes… At the time of the accident, there was not a primary HAZMAT manager assigned, which led to one of the Airmen assigned as an alternate manager to assume the duties of the primary manager by his own initiative.
It is interesting to see an ‘airmen’ being referred to as the ‘manager’.
While this Airman’s actions are commendable because he recognized the need, flight leadership failed in their duty to assign a primary program manager.
The AIB they state:
Additionally….managers did not lock the barrels, observe servicing of hydraulic cart to ensure maintainers were properly servicing hydraulic or oil hand carts, nor log what hydraulic or oil servicing carts were filled from the barrels.
Moreover, the hydraulic pump that sits on top of the barrel had no Teflon thread sealer, which could permit water to contaminate the hydraulic fluid if the barrel was not stored properly.

Contaminated Hydraulic Barrel and Pump Threads (Credit: USAF AIB)
Investigators found that movement of barrels (e.g. for exercises) were not fully traceable.
For example, information about at 354 FGS hydraulic fluid barrel that was transported to Kadena Air Base, Japan…was overwritten by a subsequent deployment to that Air Base. This error made it impossible to track where the barrel had traveled upon completion of the exercise.
This example appears to have surfaced because of a lapse during one deployment to Kadena:
Because of incomplete records, there was insufficient information to confirm whether the barrel used…on 23 January 2025 was the same hydraulic barrel that was left outside in inclement weather at Kadena Air Base for at least six weeks…in direct violation of Air Force regulations, which require that hydraulic fluid be stored in a “container tightly closed in a dry and well-ventilated place”…
The AIB reports conclusions also reveals that similar issues occurred on another deployment (to an unnamed location).
Additionally, the hydraulic barrel that was used…had been marked “empty/consumed” in April 2024, but had not been disposed of.
This suggests the barrel had been refilled.
Nine days after the accident, on 6 February 2025, another Eielson AFB F-35A experienced an NLG unsafe indication after takeoff. After following the gear fail to retract checklist, the pilot lowered the landing gear and flew for approximately 40 minutes before landing uneventfully. Perhaps surprisingly, just days after the loss of an aircraft, neither the pilot nor their wingman noticed that the nose wheel was misaligned.
Investigation indicated the NLG unsafe indication was due to its uplock missing its roller and rotating the nose wheel 10 degrees to the left. Upon landing, reordered data showed the nose wheel angle reduced to 5 degree. The NLG and right MLG struts were also found to have “significant” water contamination.

Both this and the accident aircraft had flown after their last servicing without problems. Investigators noted however that those uneventful flights were on warmer days and the aircraft had spent less time outside their heated shelters prior to taxi.
The Effect of Contaminated Hydraulic Fluid on the Landing Gear
The AIB conclude that the NLG didn’t fully extend due to ice build-up within it’s strut due to the presence of “significant water contamination” and “ambient freezing temperatures around Eielson AFB”.
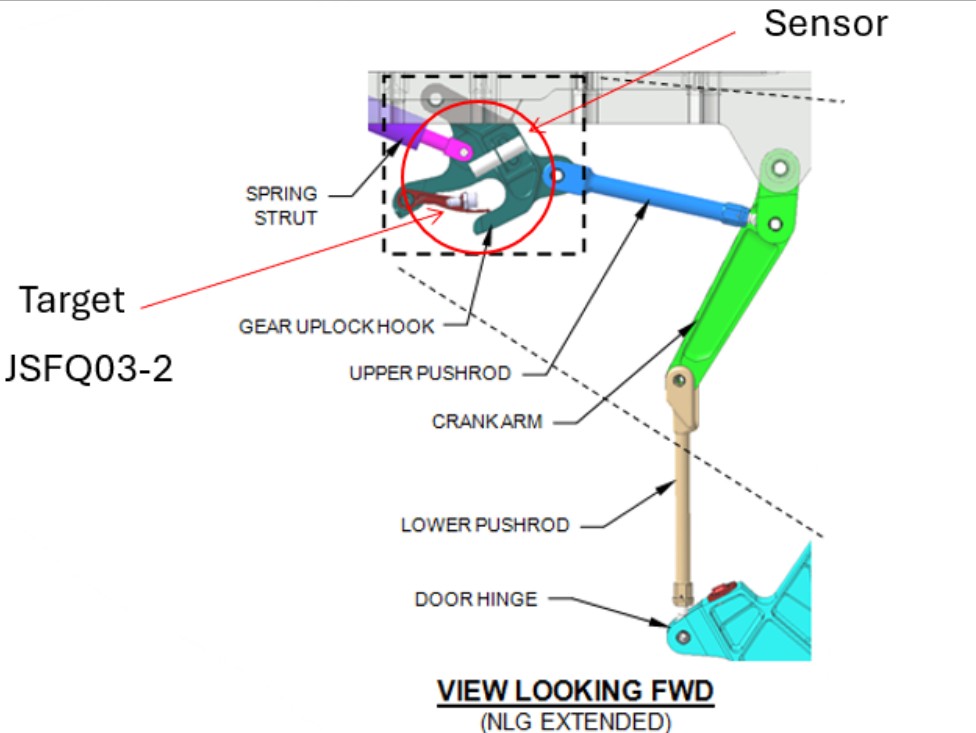
F-35A NLG Uplock (Credit: USAF AIB)
The lack of full extension caused a misalignment that prevented the NLG uplock hook [which is connected also to the NLG door] from catching the NLG uplock roller, causing damage to the metal adjacent to the roller.
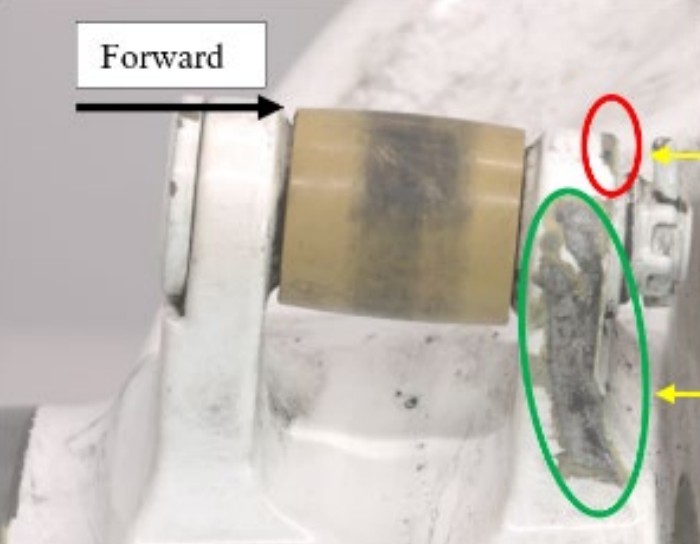
Damaged NLG Uplock Hook (Credit: USAF AIB)
The NLG has centering cams at both ends of the strut, but with the partially extended NLG these could not ensure proper centering of the NLG.
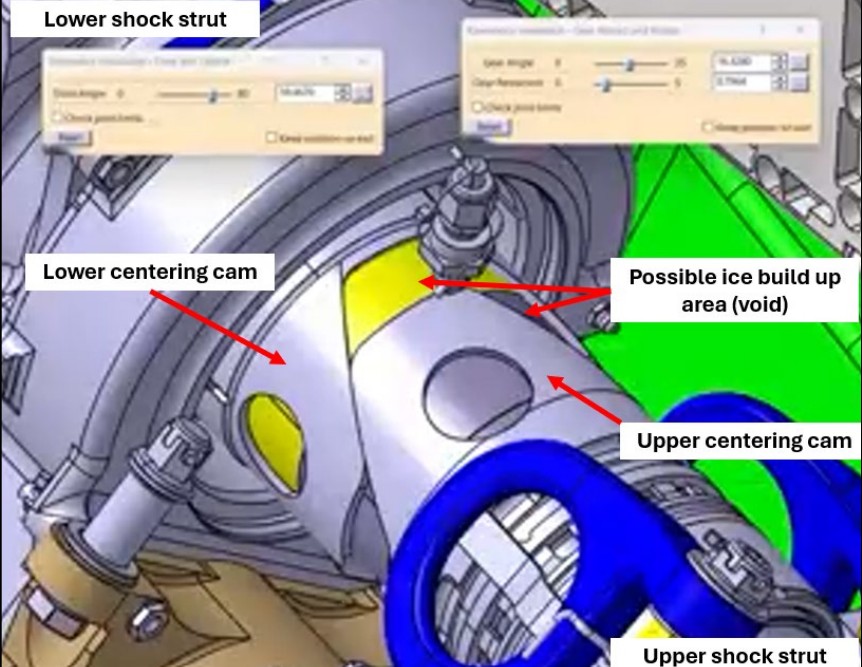
F-35A NLG Lower Centering Cam (Credit: USAF AIB)
“Significant” corrosion pitting was found within the strut but that did not affect NLG functionality.
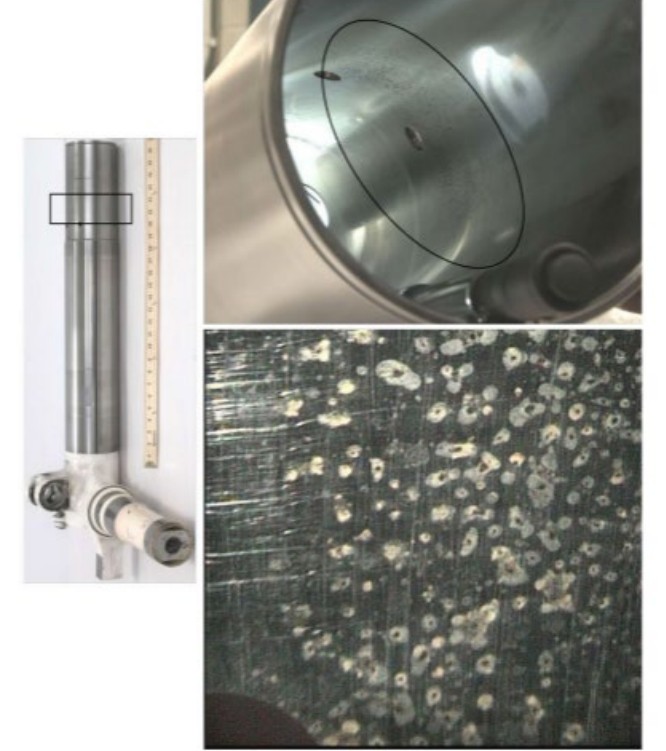
Corrosion Pitting Identified in MLG Piston (Credit: USAF AIB)
While not commented upon, that would suggest water contamination was present for some time.
Loss of Control
During the two touch-and-go landings to attempt to recenter the NLG wheel, first the right MLG strut and then left MLG strut did not fully extend. The AIB concluded this was also due to frozen water contamination in those struts too.
This meant that after the second touch-and-go, all valid WoW signals indicated the aircraft was on the ground and the F-35A transitioned to the On Ground (OG) flight control law (CLAW).
If an aircraft is airborne but still in the OG CLAW, it will experience significant degradation in flying qualities and loss of control can be expected.
Crew Decision Making
The AIB report states:
The entire team involved…admirably dealt with a challenging situation that had not been seen in the F-35 fleet previously.
The pilot used a variety of resources available to troubleshoot and attempt to safely recover the aircraft.
The wingman showed initiative and superior problem-solving abilities by his excellent and timely inputs and observation…
The SOF, Lockheed Martin engineers, and 354th OG leadership all assisted and provided their best advice and considered a variety of potential options to fix the NLG.
Then they note that:
However…the decision to advise the pilot to accomplish touch-and-goes led to the pilot’s uncontrolled ejection.
The AIB consider the safe landing after the 6 February 2025 incident that the 28 January 2025 accident could have been prevented and that aircraft also safely recovered. They then offer the counter factual observation that:
When the pilot relayed the HRCs after the first touch-and-go, the Conference Hotel participants potentially could have referenced the Lockheed Martin maintenance circular from April 2024 that said these WoW sensor issues could lead to aircraft controllability issues.
This circular said:
The WOW switches on the MLG are a mechanical plunger switch that are known to have a history of failure due to internal damage…
These failures assert as actionable HRCs and become more frequent during extreme cold weather operations where aircraft are prepared for flight in a climate controlled hangar and takeoff 20-40 minutes after being exposed to outside ambient conditions. Faults should be taken as an early indication of failure.
If an actionable HRC is asserted noting a fault to a MLG WOW switch, the AFRS tied to that HRC must be followed… Not acting on a WOW switch fault HRC could result in…WOW switches faulting…on a future flight which can cause erratic flying qualities making it difficult for the pilot to maintain control of the aircraft.
Strictly, in the case of this accident, the WoW sensors had not themselves failed though and the erratic flying qualities were because the landing gear pistons were behaving in a way that resulted in an abnormal WoW status being detected. The AIB add counter-factually:
Had the Conference Hotel participants considered this potential outcome, they likely would have advised a planned full stop landing or a controlled ejection instead of a second touch-and-go.
It is not clear if the last point is the AIB’s opinion (which will be subject to hindsight bias) or the reflection of the Conference Hotel participants themselves (a more credible source).
AIB HFACS Analysis
The AIB used the Department of Defense Human Factors Analysis and Classification System 8.0 (DoD HFACS 8.0) to analyse the accident. This framework is divided into four categories: Acts, Preconditions, Supervision/Leadership, and Organizational Influences. Each category is then subdivided into groups of human factors and finally specific human factors classifications. The AIB identify three classifications but leave the reader to determines which aspect of the accident they relate to.
- Precondition – Team Coordination/Communication Factors – PP101 Ineffective Team Resource Management: which is when crew/team members failed to actively maintain an accurate and shared understanding of the evolving task, or manage their distribution of tasks, which resulted in a hazardous condition or unsafe act. This likely relates to the conference call.
- Supervision/Leadership – Ineffective Supervision – SI001 Ineffective Supervisory or Command Oversight: which is when the availability, competency, quality or timeliness of supervisor/leader oversight did not meet task or mission demands, which resulted in hazardous conditions or unsafe acts. By examining the AIB’s conclusions (below) we see this seemingly relates to the management of the HAZMAT Program.
- Supervision/Leadership – Ineffective Supervision – SI007 Failed to Identify or Correct Hazardous Practices, Conditions or Guidance: which is when any supervisor/leader in the unit failed to identify or correct known hazardous conditions of equipment, facilities, or written procedures/guidance, or correct unsafe work practices of personnel within his/her scope, which resulted in hazardous conditions or unsafe acts. The AIB’s conclusions indicates this relates the control of hydraulic fluid.
You will note there were NO unsafe acts and NO organisational influences.
The former is strange because that would indicate that the factors identified did NOT actually result in any unsafe or causal acts so by implication did not actually affect human performance! The latter suggests that the AIB were unable to identify factors that resulted in Supervision/Leadership issues (such as the lack and turnover of personnel identified above). Its possible that these shortcomings in the HFACS analysis are due to the AIB’s role in focusing rather selectively on accountability rather than on opportunities for improvement.
AIB Conclusions
The NLG retraction failure was due to hydraulic fluid water contamination. The water had frozen, preventing full strut extension, resulting in the NLG being canted to the left. The same contamination affected the two MLG struts. The ice that formed in those prevented their full extension after the touch-and-goes that led the WoW sensors to erroneously indicate the aircraft was on the ground.
Additionally, the AIB president found, “by a preponderance of the evidence”, that:
…crew decision making including those on the in-flight conference call, lack of oversight for the Hazardous Materials program, and lack of adherence to maintenance procedures for hydraulic servicing were substantially contributing factors.
Our Observations on Organisational Accidents
James Reason, Professor Emeritus, University of Manchester popularised the expression ‘organisational accident’ with his seminal 1997 book Managing the Risks of Organizational Accidents. He used the term to differentiate simple ‘individual accidents’ involving just one person from complex accidents involving more people, organisations, technology and systems. Reason explained that:
Organizational accidents have multiple causes involving many people operating at different levels of their respective companies.
Such accidents result from ‘latent organisational failures’ that are like pathogens that have infected the organisation. In the earlier, 1995 book, Managing the Risks of Organizational Accidents, Maurino, Reason, et al give examples:
-
Lack of top-level management safety commitment or focus
-
Conflicts between production and safety goals
-
Poor planning, communications, monitoring, control or supervision
-
Organizational deficiencies leading to blurred safety and administrative responsibilities
-
Deficiencies in training
-
Poor maintenance management or control
-
Monitoring failures by regulatory or safety agencies
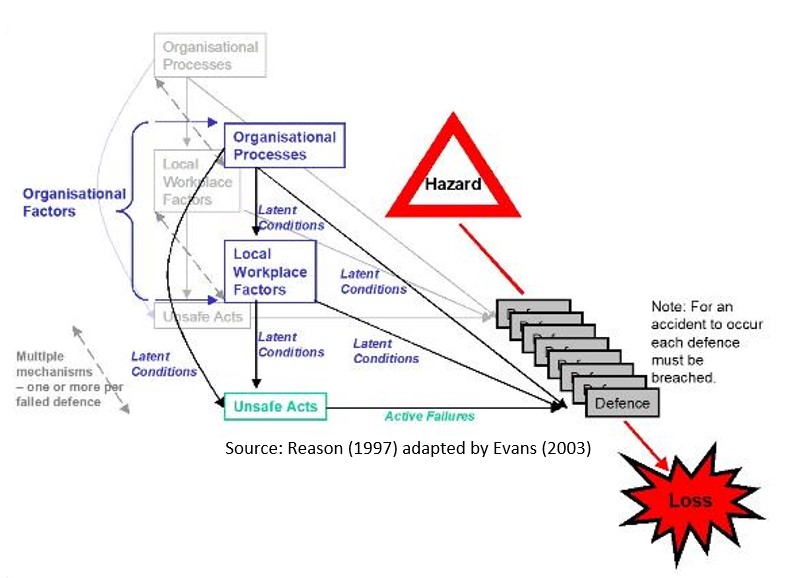
Reason famously illustrated how pathogens build up through the concept of the swiss cheese model, where each layer of cheese represents a defensive barrier.
Latent holes in the cheese, the pathogens, are introduced by both local workplace and organisational factors that remain dormant until holes in every layer align. Often the last line of defence is breached by a human action but focusing on that in safety investigations, means the inherent pathogens are ignored and barriers and control remain unfixed.

James Reason’s Swiss Cheese Model from Managing the Risks of Organisational Accidents (1997)
The Aerossurance visualisation of this model is that as time progresses many of these holes will dynamically change size and position as circumstances change, either increasing or decreasing the risk.
In practice human actions also routinely plug the holes too, knowingly or unknowingly. Another reason that focusing on the actions or inactions of one individual can mean missing the big picture.
Safety Resources
You may also find these Aerossurance articles of interest:
- The Loss of RAF F-35B ZM152: An Organisational Accident A £81 mn fighter is downed by FOD, one of its own intake blanks. This case study illustrates James Reason’s concept of Organisational Accidents and how just asking “who left the intake blank ?” misses the real reasons behind this accident.
- B1900D Emergency Landing: Maintenance Standards & Practices The TSB report posses many questions on the management and oversight of aircraft maintenance, competency and maintenance standards & practices. We look at opportunities for forward thinking MROs to improve their maintenance standards and practices.
- NASA Challenger Launch Decision Another critical conference call
- BA B747 Landing Gear Failure Due to Omission of Rig Pin During Maintenance
- What a Difference a Hole Makes: E-8C JSTARS $7.35 million Radar Mishap
- USAF Tool Trouble: “Near Catastrophic” $25mn E-8C FOD Fuel Tank Rupture
- Inadequate Maintenance, An Engine Failure and Mishandling: Crash of a USAF WC-130H
- USAF Engine Shop in “Disarray” with a “Method of the Madness”: F-16CM Engine Fire
- Inadequate Maintenance at a USAF Depot Featured in Fatal USMC KC-130T Accident
- When Down Is Up: 747 Actuator Installation Incident
- Maintenance Human Factors in Finnish F406 Landing Gear Collapse
- Lost in Translation: Misrigged Main Landing Gear
- Cessna Citation Excel Controls Freeze
- B214ST Tail Rotor Drive Shaft Coupling Misassembly
- Crossed Cables: Colgan Air B1900D N240CJ Maintenance Error
- Crazy KC-10 Boom Loss: Informal Maintenance Shift Handovers and Skipped Tasks
- Frozen Dash 8-100 Landing Gear After ‘Improper Maintenance Practices’ Say NTSB
- ATR 72 Rudder Travel Limitation Unit Incident: Latent Potential for Misassembly Meets Commercial Pressure
- Loose B-Nut: Accident During Helicopter Maintenance Check Flight
- USAF RC-135V Rivet Joint Oxygen Fire
- CHC Sikorsky S-92A Seat Slide Surprise(s)
- SAR AS365N3 Flying Control Disconnect: BFU Investigation
- In-Flight Flying Control Failure: Indonesian Sikorsky S-76C+ PK-FUP
- AAR Bell 214ST Accident in Afghanistan in 2012: NTSB Report
- Misassembled Anti-Torque Pedals Cause EC135 Accident
- EC130B4 Accident: Incorrect TRDS Bearing Installation
- Ungreased Japanese AS332L Tail Rotor Fatally Failed
- R44 Ditched After Loss of TGB & TR: Improper Maintenance
- Missing Cotter Pin Causes Fatal S-61N Accident
- Emergency S-76D Landing Due to Fumes
- Engine & Emergency Flotation Failures – Greenland B206L4 Ditching
- The Missing Igniters: Fatigue & Management of Change Shortcomings
- FAA Rules Applied: So Misrigged Flying Controls Undetected
- BEA Point to Inadequate Maintenance Data and Possible Non-Conforming Fasteners in ATR 42 Door Loss
- BA A319 Double Cowling Loss and Fire – AAIB Report
- BA A319 Double Cowling Loss and Fire – AAIB Safety Recommendation Update
- ANSV Report on EasyJet A320 Fan Cowl Door Loss: Maintenance Human Factors
- Tiger A320 Fan Cowl Door Loss & Human Factors: Singapore TSIB Report
- Human Factors of Dash 8 Panel Loss
- Fuel Tube Installation Trouble
- How One Missing Washer Burnt Out a Boeing 737
- Flying Control FOD: Screwdriver Found in C208 Controls
- Cessna 208 Forced Landing: Engine Failure Due To Re-Assembly Error
- Meeting Your Waterloo: Competence Assessment and Remembering the Lessons of Past Accidents
- UPDATE 15 November 2025: AS350 HESLO Fuel Incident (Superabsorbent Polymer Contamination)
You might find these safety / human factors resources of interest:
- James Reason’s 12 Principles of Error Management
- Back to the Future: Error Management
- This 2006 review of the book Resilience Engineering by Hollnagel, Woods and Leveson, presented to the RAeS by Aerossurance’s Andy Evans: Resilience Engineering – A Review and this book review of Dekker’s The Field Guide to Understanding Human Error: The Field Guide to Understanding Human Error – A Review
- Airworthiness Matters: Next Generation Maintenance Human Factors
FSF Maintenance Observation Programme (MOP)
Aerossurance worked with the Flight Safety Foundation (FSF) to create a Maintenance Observation Program (MOP) requirement for their contractible BARSOHO offshore helicopter Safety Performance Requirements to help learning about routine maintenance and then to initiate safety improvements:
Aerossurance can provide practice guidance and specialist support to successfully implement a MOP.
Recent Comments