A HEMS Helicopter Had a Lucky Escape During a NVIS Approach to its Home Base (Norsk Luftambulanse Airbus Helicopters EC135P3 LN-OOZ )
On 6 November 2020 a HEMS Airbus Helicopters EC135P3 (H145) LN-OOZ of Nordic Air Ambulance was damaged when it briefly contacted the ground after Inadvertent Entry into IMC (IIMC) while on approach to Ringsted, Denmark. The helicopter initiated a successful go-around and diverted to Slagelse Hospital.
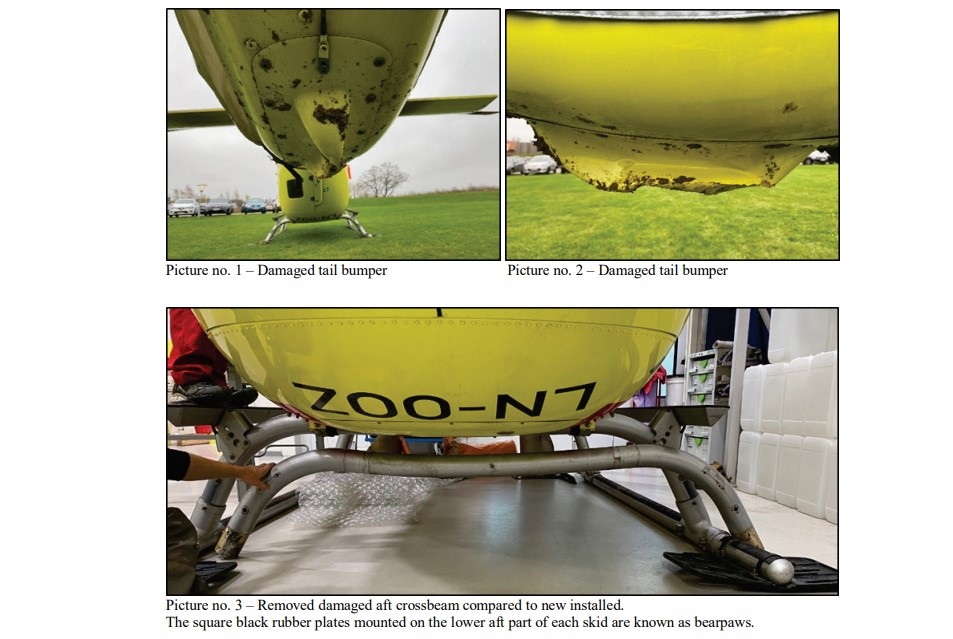
A Lucky Escape: Damage to Norsk Luftambulanse Airbus Helicopters EC135P3 LN-OOZ after IIMC CFIT (Credit: DAIB)
The Serious Incident Flight
The Danish Accident Investigation Board (DAIB or Havarikommissionen for Civil Luftfart og Jernbane) promptly issued their safety investigation report on 22 June 2021. They explain that the Norwegian operator had conducted HEMS operations in Norway since 1977 and in Denmark since 2011. The Danish operation comprised of four bases, each with one EC135. Onboard were…
…the commander (CDR) sitting in the right hand pilot seat, the HEMS technical crew member (TCM)/paramedic sitting in the left hand pilot seat and the medical doctor (MD) sitting in the right hand cabin seat.
Both the CDR and the TCM had completed the operator’s initial and recurrent Night Vision Imaging System (NVIS) training. The CDR had 13,170 of flight experience, 1,728 hours on type and 320 using Night Vision Googles (NVGs). The TCM had flow 1,766 hours on the EC135 and had 290 hours experience with NVGs.
They were working a 24-hour shift pattern. They had completed a tasking at Odense Hospital (EKOH) at 18:00. Because they had been on ‘active duty’ for more than the normal limit of 14 hours, they had requested a reserve crew be activated to take over at their home base at Ringsted (EKRS) on their return. Active duty is here defined from time of callout “until minimum one hour after block-on time”. If there were less than two hours between being on-block and the next callout, the entire time is counted as active duty.
The EKRS has an Automatic Weather Observation Station (AWOS) which the crew checked online.
At that time, the symbol presenting EKRS showed a grey square, which the flight crew interpreted as no weather information was available. The flight crew was not aware that if a grey square was tapped, available data for the location would be presented, alongside with slashed lines representing missing data.
In fact, a partial AWOS failure had occurred least two days prior. The only means to identify the failure and initiate a repair was the duty crew. However…
Due to fog and reduced visibility, the CDR was aware that the weather conditions at EKRK [Roskilde] were below VFR minima.
While en route back to EKRS they were asked…
…if they could respond to a medical emergency in the outskirts of Slagelse.
In accordance with the operator’s procedures…
….the flight crew had after an internal consultation accepted the extra HEMS mission and the subsequent flight to EKRS. [They] landed at 18:27 hrs at an industrial site in Slagelse, and attended the medical emergency.
After about 30 minutes on site the medical emergency was dealt with and the crew prepared to return to EKRS.
The flight crew used NVG during the departure from Slagelse, and the helicopter climbed to 1200 ft above mean sea level (amsl) towards EKRS. The flight crew went “NVG Off” (swung their helmet mounted NVG upwards to allow unaided vision)…
NVGs in the Up Position (Credit: DAIB)
En route to EKRS, the crew observed sporadic fog and fog patches close to the ground towards the south, while weather conditions were clear towards the north.
The TCM went “NVG On” approximately 10 nautical miles (nm) from EKRS. When the helicopter passed south of Ringsted city, halos and glare started developing around lights from cars and buildings. The flight crew noticed increasing ground fog but were fully capable of seeing through the fog and clearly identifying cars, lights, roads and buildings. They felt by no means uncomfortable with the weather conditions.

The helicopter approached EKRS from the west. There was a c 5 knot wind from the southwest.
As a part of the pre-landing check, the CDR performed a landing briefing. The landing briefing did not include any go-around criteria. It was the intention of the CDR to perform a shallow approach to obtain good references and to be able to see obstacles ahead instead of from above. This should lead to a vertical take-off and landing (VTOL) final let-down to the helipad with a landing decision point (LDP) at 120 ft radio height (RH). The radio height bug (audio alert) was set to 180 ft. The TCM set his moving map display to full screen size and selected the largest scale possible for optimum position reference.
Established on a left hand downwind for runway 23, with a ground speed (GS) of 75 knots (kt) and at an altitude of approximately 600 ft above ground level (agl), the flight crew saw unaided [when looking] ‘below’ the NVG, the aerodrome buildings, the hangars, the rotating beacon, the runway lights, the helipad lights, and the company base buildings with flashing beacon.
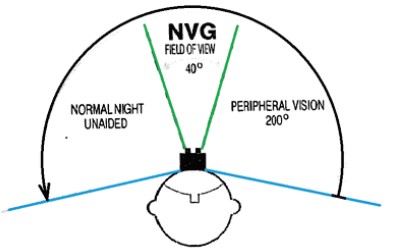
NVGs in the Down Position, Showing Direct Vision (Green) Through the NVGs and Peripheral Vision (Yellow) ‘Below’ the NVGs (Credit: DAIB Annotated by Aerossurance)
NVG Lateral Field of View (Credit: DAIB)
The perceived ground fog did not pose a risk for the flight crew concerning a VFR landing, because flight visibility was good and all runway lights, runway surroundings and the main road crossing the final approach track were visible through the ground fog.
The TCM called out 500 (ft RH), 400 and 300 with corresponding airspeeds, while the helicopter crossed [the road]j, and turned onto a left hand base with a GS of 45 kt. During this period, the CDR went “NVG On” and everything was perfectly clear in the NVG. The helicopter continued on left base and onto a 35° offset final.
The ground below consisted of ploughed farm fields with short crops and a small group of trees of a height of no more than 50 ft.

The flight crew could see the runway lights, the helipad and lights from passing cars unaided.
The visibility started decreasing, but compared to previous experiences, it was not unusual, and the flight crew still felt comfortable with the situation. In their field of view below the NVG, both flight crew members saw the small group of trees, contours on the ground, and on-ground fog patches below the helicopter.
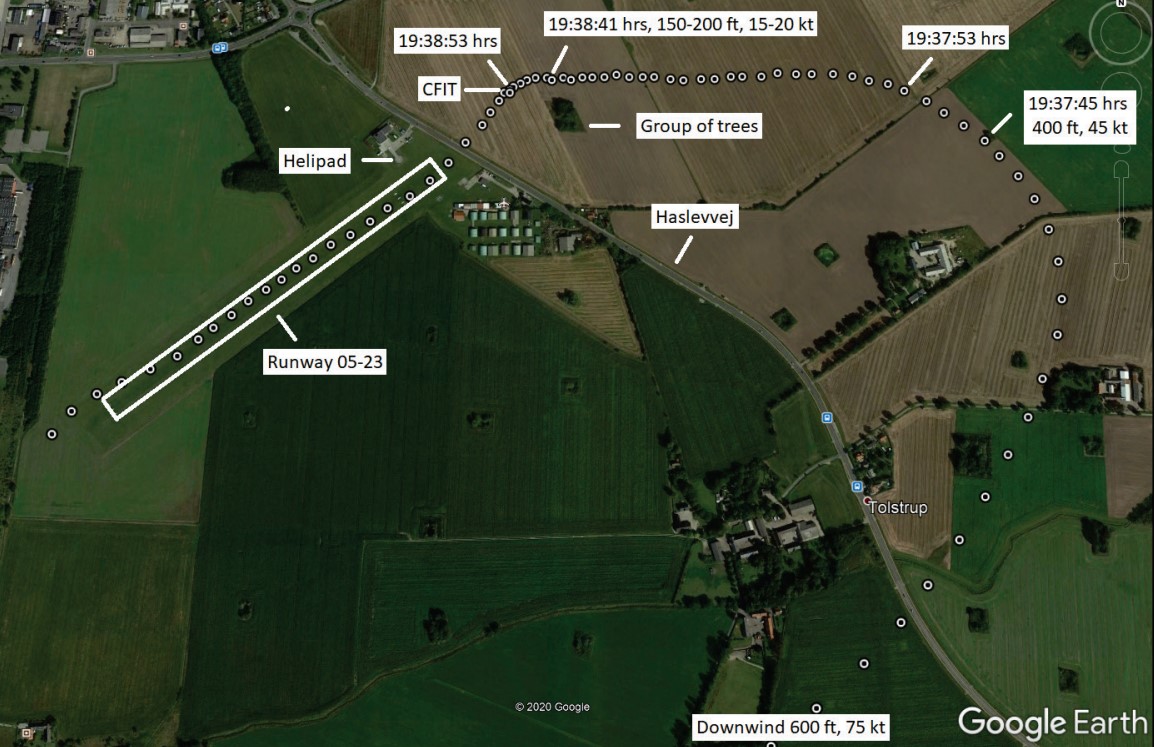
At 19:38:41 hrs, at a height of 150-200 ft agl and with a GS of 15-20 kt, the CDR aligned the helicopter with the extended centerline.
Flight Path of Norsk Luftambulanse Airbus Helicopters EC135P3 LN-OOZ – Speeds are Groundspeed and Heights are Above Ground Level (Credit: DAIB)
The CDR continued forward, while slowly reducing forward airspeed by lifting the nose of the helicopter. In succession, starting shortly before or about this time, the callouts 200 ([by the] TCM), Decision Height (auto-generated) and 100 (auto-generated) likely occurred.
About 12 seconds later…
…suddenly and without warning, the CDR saw only bright light within his NVG. The CDR was startled, but noticed a RH indication of 50 ft on his Primary Flight Display (PFD) and tried to obtain outside visual references by looking below the NVG, but saw only darkness.
As the CDR initiated a go-around the helicopter contacted the ground in a field approximately 134 m northeast of the road and 210 m short of the helipad.

Impact Site: Norsk Luftambulanse Airbus Helicopters EC135P3 LN-OOZ (Credit: DAIB)
Both flight crew heard the aural indication for max power as the helicopter climbed away. The CDR regained normal visual references through his NVG. The crew entered a circuit for runway 23. Apart from a “small change” in vibrations, the crew detected no evidence of damage.
Initially, the flight crew thought that they had impacted within, or very close to the aerodrome area, because they perceived the position of the helicopter to be just before Haslevvej, when they lost NVG vision. Then and much to their surprise, the flight crew realized that the helicopter had been further away from the helipad and that the impact took place in the ploughed farm field. The flight crew decided to abort the landing to runway 23 and diverted to EKSE without any further occurrences.
Ground Impact Marks: Norsk Luftambulanse Airbus Helicopters EC135P3 LN-OOZ (Credit: DAIB)
The helicopter sustained damage to the tail bumper and the landing skid. Due to the impact, the aft crossbeam on the landing skid bent approximately 3 cm. According to the helicopter manufacturer, a vertical touchdown speed of 200 – 500 ft/minute would result in plastic deformation of the cross tubes but no damage to the fuselage.

The Main Gearbox (MGB) was replaced due to an overtorque.
The DAIB Safety Investigation
DAIB note that:
From 5-9-2019, EASA required all commercially operated helicopters (including HEMS) with a MTOM of 2,250 kg or more, and first issued with an individual certificate of airworthiness on or after 5-9-2022, to carry flight recorders.
However, neither a Flight Data Recorder (FDR) nor a Cockpit Voice Recorder (CVR) were fitted or required for LN-OOZ. Investigators were able to extract data from several avionics systems and did have access to Automatic Dependent Surveillance Broadcast (ADS-B) data.
When the helicopter started the base leg…
…the CDR went “NVG On” and everything was perfectly clear in the NVG. The impression of sudden improved visibility could have suppressed any clues to deteriorating flight visibility at lower altitude due to intensifying fog. However, both flight crew members saw the small group of trees below their NVG, and sporadic fog patches close to the ground. This indicates that even overhead the ploughed fields, where conditions for widespread fog were likely due to radiation heat loss, fog was most likely only present in patches.
From 19:37.53 hrs and until 19:38:41 hrs, the helicopter flew the 35° off-set final. This was overhead ploughed fields with no lights and sparsely ground contours, except for the group of trees, which at some point most likely disappeared from view due to the helicopter structure. The forward vision of the flight crew was through their NVG, and peripheral cues, especially from below, was likely limited, and probably perceived as dark. Despite a slight decrease in visibility, the flight crew still had [visual] references…
As the CDR raised the nose of the helicopter to lower forward speed, it caused the position of the runway lights and helipad to move down in the flight crews field of view. This change in angle might have given an impression of being closer to the helipad, and approaching the correct position for the LDP 120 point, roughly overhead [the road]. Possibly, due to the difficulties associated with depth perception when using NVG, in combination with a lack of peripheral cues, the flight crew did not realise they still were approximately 150-200 m short of the LDP position.
Other visual illusions might have influenced the situational awareness of the flight crew, like the black hole effect or the height illusion effect. It is also possible that the time spent on the off-set leg, tricked the flight crew into believing they were closer to the helipad.
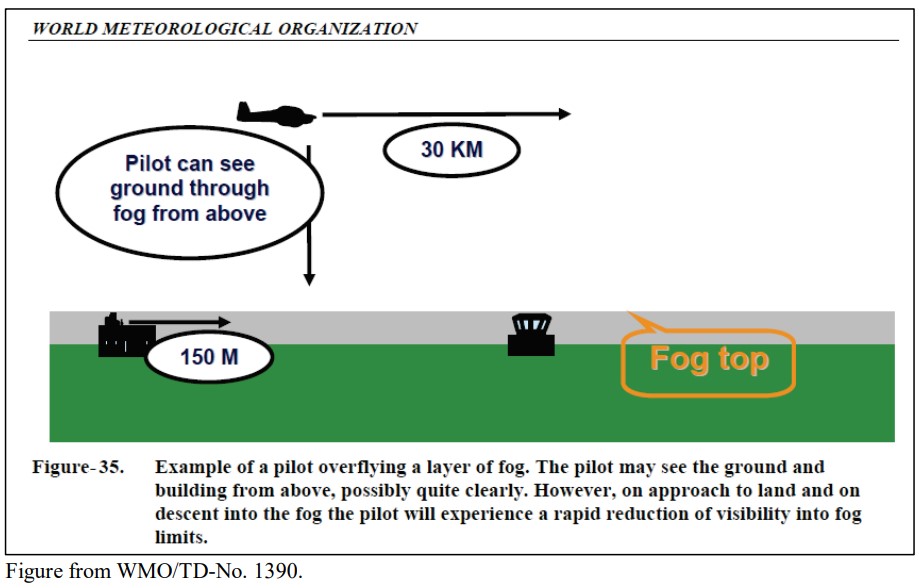
The helicopter then descended into fog, which the flight crew were unable to detect from above, causing a very bright image to appear in the CDR’s NVGs, which was perceived as a whiteout.
Because the whiteout came as a complete surprise to the CDR, his reaction time was likely longer than it would have been, if he were prepared for the possibility of a whiteout. An identification of possible criteria requiring a go-around might have removed or decreased the startling effect of the CDR. Descending through 50 ft RH, and without any outside visual references, the CDR initiated a go-around. Due to the helicopter descent rate, the power application came too late to prevent the helicopter from impacting the farm field.
However, the power application most likely reduced the descent rate and thereby the consequences of the impact. Because the impact seemingly happened with low forward speed and in a close to upright position, the spring effect of the undercarriage assisted in getting the helicopter airborne again.
The investigators note that:
Because NVG was only intended as an aid under VMC, training in flight under inadvertent IMC should focus on maintaining helicopter control and returning to flight under VMC. This was incorporated in the operator initial and recurrent NVIS training, and implemented in the operating procedures, providing flight crews the necessary prerequisites for safe operation.
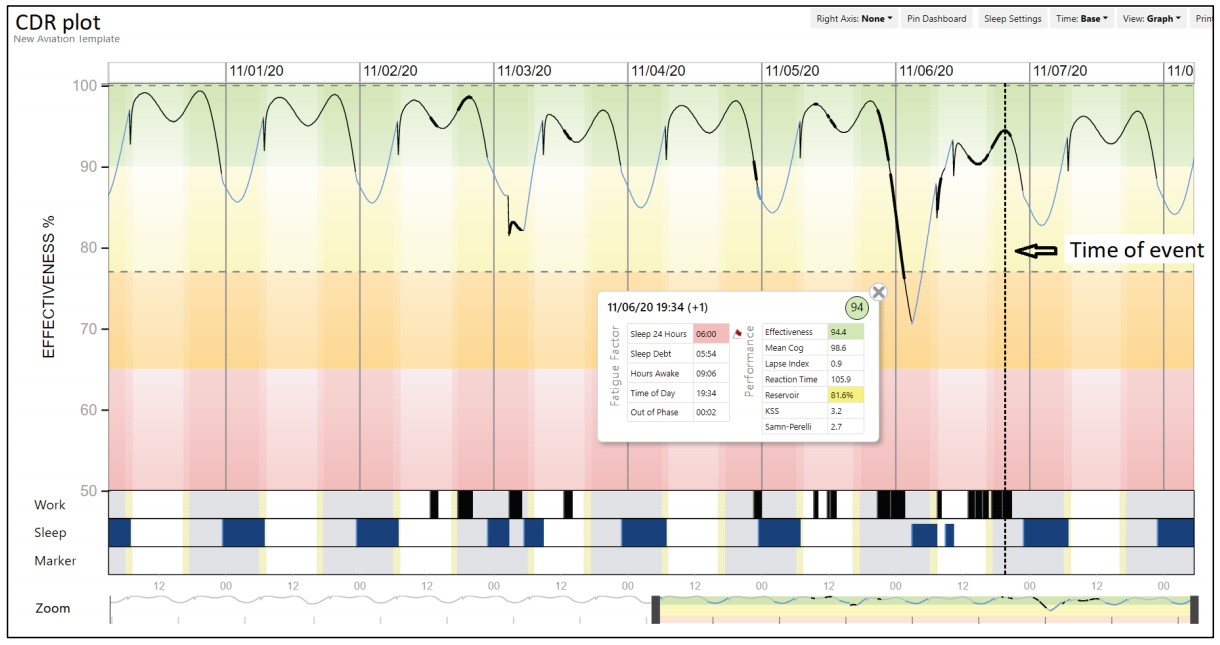
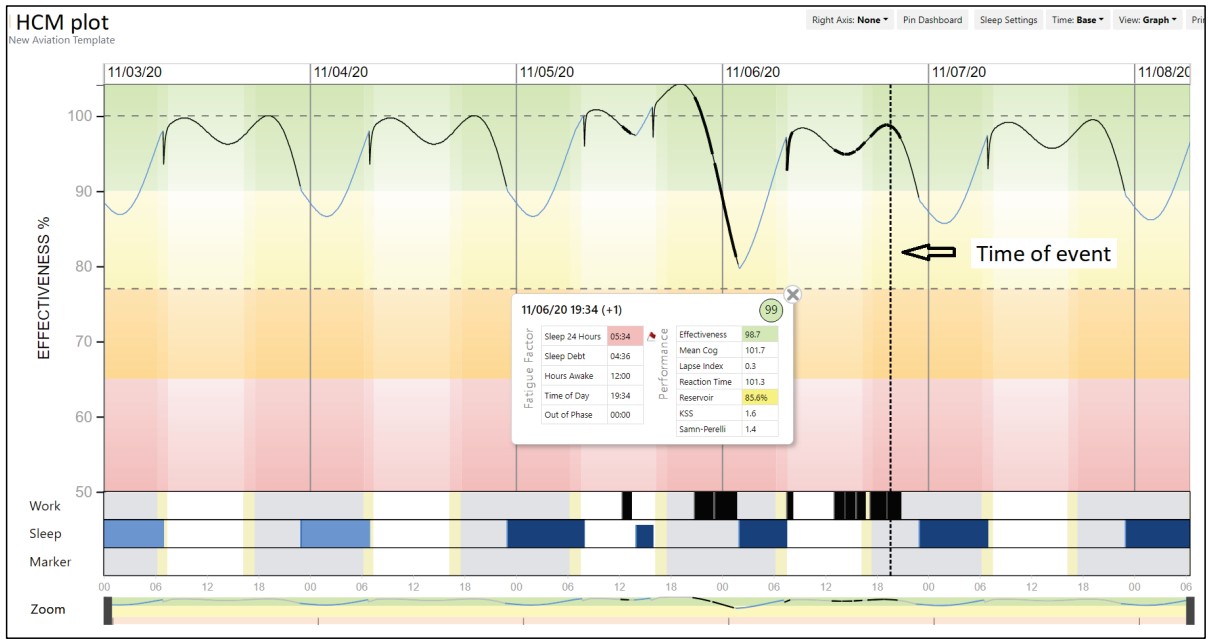
Based on the crew’s recent duty and rest the investigators concluded it was unlikely that the flight crew were suffering from fatigue at the beginning of their 24-hour duty period. As the crew were operating beyond the normal limit of 14 hours of active duty the investigators prudently used Fatigue Avoidance Scheduling Tool (FAST) software objectively determine if flight crew fatigue could have contributed to the sequence of events.
Except being a bit hungry, no crew members…expressed fatigue or unfitness for flight. The flight crew perceived state of fitness for flight seems realistic, considering the calculated FAST crew performance effectiveness above 90 % for both flight crew members.
Even though the flight crew reported quality and quantity of sleep during the preceding 24 hours to be less than optimum, the event occurred during a period of natural circadian high. This most likely reduced the perceived effect of prolonged active time on the crew performance effectiveness and possibly shaded any effects of flight crew acute/transient fatigue.
The investigators concluded that…
…flight crew fatigue was likely not a causal factor. However, it might have contributed to the sequence of events.
Both flight crew members individually stated that if either had felt unfit, they would have parked the helicopter at the industrial site in Slagelse, and that the operator had procedures in place to handle such an event. To the AIB, this suggests that the operational pressure for returning to EKRS was limited, especially taking the short distance between the industrial site in Slagelse to EKRS into consideration (approximately 25 minutes driving time by car). However, it must be acknowledged that a subconscious desire to return to the nearby home base possibly could have influenced the flight crew decision making process (get-home-itis syndrome).
DAIB Conclusions
The DAIB determined that the following causal factors led to this Controlled Flight Into Terrain (CFIT) serious incident:
- A less than optimum pre-flight weather briefing.
- An action plan on flying a shallow approach under VFR conditions with low fog and fog patches.
- Difficulties in assessing height and depth while using NVG.
- Loss of situational awareness due to visual illusions.
- NVG whiteout at low altitude.
Safety Resources
The European Safety Promotion Network Rotorcraft (ESPN-R) has a helicopter safety discussion group on LinkedIn. You may also find these Aerossurance articles of interest:
- Low Recce of HEMS Landing Site Skipped – Rotor Blade Strikes Cable Cutter at Small, Sloped Site
- BK117B2 Air Ambulance Flameout: Fuel Transfer Pumps OFF, Caution Lights Invisible in NVG Modified Cockpit
- Norwegian HEMS Landing Wirestrike
- Air Ambulance B407 Hospital Helipad Deck Edge Tail Strike During Shallow Approach
- Sécurité Civile EC145 Mountain Rescue Main Rotor Blade Strike Leads to Tail Strike
- NTSB on LA A109S Rooftop Hospital Helipad Landing Accident
- Air Ambulance Helicopter Fell From Kathmandu Hospital Helipad (Video)
- US Air Ambulance Near Miss with Zip Wire and High ROD Impact at High Density Altitude
- Hanging on the Telephone… HEMS Wirestrike
- Air Ambulance Helicopter Downed by Fencing FOD
- Ambulance / Air Ambulance Collision
- Beware Last Minute Changes in Plan
- Air Methods AS350B3 Night CFIT in Snow
- A Short Flight to Disaster: A109 Mountain CFIT in Marginal Weather
- US Fatal Night HEMS Accident: Self-Induced Pressure & Inadequate Oversight
- HEMS A109S Night Loss of Control Inflight (N91NM)
- Air Ambulance A109S Spatial Disorientation in Night IMC (N11NM)
- US HEMS EC135P1 Dual Engine Failure: 7 July 2018
- Misassembled Anti-Torque Pedals Cause EC135 Accident.
- Taiwan NASC UH-60M Night Medevac Helicopter Take Off Accident
- Fatal Fatigue: US Night Air Ambulance Helicopter LOC-I Accident
- Deadly Dusk Air Ambulance Bird Strike
- HEMS Black Hole Accident: “Organisational, Regulatory and Oversight Deficiencies”
- HEMS S-76C Night Approach LOC-I Incident
- Life Flight 6 – US HEMS Post Accident Review
- US HEMS “Delays & Oversight Challenges” – IG Report
- US HEMS Accident Rates 2006-2015
- More US Night HEMS Accidents
- That Others May Live – Inadvertent IMC & The Value of Flight Data Monitoring
- Fatal US Helicopter Air Ambulance Accident: One Engine was Failing but Serviceable Engine Shutdown
- Wire Strike on Unfamiliar Approach Direction to a Familiar Site
- Loss of Bell 412 off Brazil Remains Unexplained
- Plan Continuation Bias & IIMC in Kenyan Police AW119 Accident
- S-76A++ Rotor Brake Fire
- Firefighting AW139 Loss of Control and Tree Impact
- Sécurité Civile EC145 Mountain Rescue Blade Strike
- Sécurité Civile EC145 SAR Wirestrike
- UPDATE 7 November 2021: Italian Alps AW139 Mountain Rescue Hoisting Blade Strike
- UPDATE 20 November 2021: NVIS Autorotation Training Hard Landing: Changed Albedo
- UPDATE 15 January 2022: Air Ambulance Helicopter Struck Ground During Go-Around after NVIS Inadvertent IMC Entry
- UPDATE 7 January 2023: Blinded by Light, Spanish Customs AS365 Crashed During Night-time Hot Pursuit
- UPDATE 10 June 2023: EC135 Air Ambulance CFIT when Pilot Distracted Correcting Tech Log Error
- UPDATE 13 July 2024: Fatal USCG SAR Training Flight: Inadvertent IMC
- UPDATE 20 July 2024: Night CHC HEMS BK117 Loss of Control
Recent Comments