SAR AW101 Roll-Over: Entry Into Service Involved “Persistently Elevated and Confusing Operational Risk”
On 24 November 2017, Royal Norwegian Air Force (RNoAF) Leonardo AW101-612 Search and Rescue (SAR) helicopter 0268 rolled over during start-up at Sola for an engine drying run following a routine compressor wash. The two pilots and the adjacent ground personnel were uninjured, but the helicopter suffered extensive damage.

The helicopter was the first AW101 delivered to Norway, having arrived a week before, and had been operated by the military AW101 Operational Test and Evaluation (OT&E) unit for just three days.
The Norwegian Military Accident Investigation Board (Statens havarikommisjon for Forsvaret [SHF]) released their investigation report on 11 November 2019 (in Norwegian only). We recently re-visted this report as it was mentioned in a recent Norwegian Safety Investigation Authority (NSIA) report on a 2020 RNoAF C-130J Hercules serious incident, which we discussed in: A Second from Disaster: RNoAF C-130J Near CFIT. That report made recommendations on creating an independent military aviation regulator in Norway, enhance risk management and develop the Air Force safety culture.
The Ground Run
The investigators comment that often compressor washes are conducted before scheduled flights to eliminate the need for a drying run. In this case there was no flight envisaged, so a specific ground run was planned. This can be done by one pilot, but two were allocated, both for reasons of safety and to help build type experience. The pilots had only 13 and 26 hours on type, plus about 60 hours of simulator time each. The former was the Pilot Flying (PF) and planned & briefed the task but the other was Pilot Monitoring (PM) and Aircraft Commander. The PF had not previously started up the aircraft just to dry the compressors. The PM had only done it once before. The investigators note the preparations were through and unhurried. Furthermore Cockpit Voice Recordings indicated the crew were unstressed and task-focused.
There were 125 certified Flight Reference Cards (FRCs) for the AW101-612, which were the authorised procedures for flight operations.

The FRCs were written on the basis that start-up and shutdowns are memory drills. Due to their low time on type, the AW101 OT&E crews also used a locally developed checklist for such tasks, called the Kneeboard Checklist v19.
The two pilots started the helicopter’s three engines and set engines numbers 2 and 3 to accelerate the rotor. Surveillance video of the incident shows that the helicopter gradually lifting…for just over 15 seconds while the rotor accelerated. As the rotor reached full speed, the left-hand main wheel left the ground.
| Time (approx.) | Event | Note |
| PF starts engine 1, | The collective is initially approx. 53%. This is in it | |
| 2 and 3 in Ground Idle | high end of what is normal when the helicopter | |
| (idle) | has been standing still for a few hours. The collective comes down to | |
| 45% when the engines establish pressure in | ||
| the hydraulic system. | ||
| 00:00 | The rotor is started | The rotor accelerates to 30% with the three engines in |
| Ground Idle. | ||
| 00:30 | PF sets engine 2 to | This is to accelerate the rotor from 30% to 102%. |
| FLIGHT | ||
| 00:33 | Engine 2 achieves | During start-up, FADEC limits the engine power to |
| 80% torque | 80% torque. Normally this will be sufficient to | |
| rotor reaches full speed in approx. 10 seconds, | ||
| and the torque on motor 2 will then be reduced | ||
| automatically to approx. 50%. | ||
| 00:35 | PF sets engine 3 to | The rotor is still accelerating. |
| FLIGHT | ||
| 00:38 | Engine 3 achieves | If engine 2 has already accelerated the rotor, |
| 80% torque | engine 3 does not normally achieve 80% torque, as it normally | |
| establishes itself at approx. 25% together with engine 2. | ||
| The rotor accelerates | The rotor accelerates more slowly than normal. The pilots | |
| think it is due to water in the compressors, but it | ||
| due to the high position of the collective. | ||
| 00:46 | The rotor passes | At this rotor speed, FADEC stops limiting the max |
| about 96% speed | torque on the engines. | |
| Engine 2 and 3 increase | The automatics increase the torque as much as necessary | |
| to 91% torque | to achieve a rotor speed of 102%. The rotor | |
| accelerates abruptly faster due to higher torque. | ||
| 00:48 | The rotor passes | Engine power is automatically reduced to maintain |
| 100% speed | rotor speed of 102%. | |
| 00:49 | Rotor achieves 102 | Motor 2 and 3 pass 85% torque, descending. |
| % speed | ||
| 00:50 | Left main wheel | The helicopter thinks it’s in the air (weight on wheels |
| leaving the ground | switch goes to «air») and the pilots are notified that | |
| autopilot is off. | ||
| 00:51 | PM pushes | This attempt to correct for the role of the helicopter |
| cyclic stick | movement, has no noticeable effect. | |
| left | ||
| 00:51 | PF shuts down engine 3 | |
| 00:52 | PM shuts down engine 1 | |
| 00:52 | Rotor hits | |
| ground | ||
| 00:54 | PF shuts down engine2 | |
The marshaller tried to signal for the crew to lift off but the PF chose not to as the autopilot was off and only two engines were connected to the rotor. The crew were able to shut down two engines before the blades strike occurred. The ground personnel ran for cover as rotor debris flew across the ramp.
Organisational and Project Background
The RNoAF AW101 fleet are actually owned by the Ministry of Justice and Emergency Preparedness (JD) who purchased them as part of the NAWSARH (Norwegian All Weather Search and Rescue Helicopter) project to replace the dated Westland Sea King. In 2011 RNoAF created the ‘Project 7661’ office to manage the NAWSARH introduction but almost immediately flagged a shortage of suitable competent personnel to support the project, especially with parralel procurements of F-35, P-8 and NH90. Sixteen AW101s were ordered by JD as part of a £1bn purchase and support contract awarded in December 2013. Operations would ultimately be conducted by 330 Squadron, with Leonardo conducting the maintenance.
The AW101 OT&E unit was created in March 2015 to, the investigators explain, “develop SAR guidelines, standards and procedures” for AW101 operation. It was also planned that this unit, once trained by Leonardo in the UK, would deliver training to the operational crews. Coupled with the apparent purpose in its title of test and evaluation, one might anticipate a high workload and conflicting priorities in this unit.
At the beginning of 2016, only 22 of 43 positions on the OT&E unit were filled however.
Although ground school training commenced in late 2016, programme delays meant the training of the initial crews was spread out over a year. The investigators comment that:
Although several aspects of the training were well received by the Norwegian personnel, there were a number of challenges, especially with regard to the delayed development of new systems for AW101-612 and associated documentation.
Additionally, the cockpit procedure trainer initially used was configured for the different Danish AW101 variant.
The OT&E unit had already been struggling to maintain its team’s helicopter currency in the years before the AW101 training commenced, relying on limited Sea King and Bell 412 simulator sessions. JD did fund two extra AW101 flights per student but for some reason the O&TE unit didn’t take advantage of that.
Ongoing changes in the helicopter’s configuration, documentation and delivery date were a constant source of additional work…
Employees at OT&E responded that so much of their time had to be spent reconfiguring existing, internal training programs rather than prepare the actual flight through standardization and self-training.
Although the AW101-612 was produced in the UK, it was type certificated for Norway by the Directorate for Air Armaments and Airworthiness (DAAA) of the Italian Ministry of Defence (the UK Military Aviation Authority‘s charter precludes their certification of export aircraft).
Sub-optimally, the Norwegian Chief of the Air Force is also the Norwegian Military Aviation Authority. The Air Operations Inspectorate (LOI) is the Chief of the Air Force’s body for exercising military aviation regulation. The AW101 OT&E unit however also reported to LOI, effectively further diminishing independent regulatory oversight. Further, “LOI had for much of the period too few personnel with relevant helicopter competence”.
Only two weeks before the first AW101 arrived at Sola, the OT&E unit submitted a number of applications for dispensations to extant regulations to the LOI.
The OT&E unit had a Safety Management System (SMS), with the manual issued at V1.0 only on 13 November 2017, days prior to the delivery of the first aircraft. The unit’s Flight Safety Officer (FSO) was one of the more junior pilots in the unit, despite RNoAF guidance that this should be a position held by a more experienced pilot.
The investigators note that “the lines of communication…[had]…not worked optimally. This has led to an extra burden on the OT&E unit and reduced overview and involvement by P7661 and LOI”.
Instead of P7661 acting as a buffer between NAWSARH and the department, as the management document suggests, OT&E was given a large part of the increasingly challenging task of balancing the external process with NAWSARH, and thereby Leonardo, with departmental tasks. At the same time, the management at OT&E was to act as aircraft commanders and instructors and review all courses and check-outs on AW101.
The lack of a station establishment at Sola or a parent wing also put more administrative burden on the OT&E unit than normal and meant less support (such as having a Station Senior FSO). The investigators observe that:
It is always more difficult to say stop when you yourself are directly involved in the operational delivery. The pressure experienced by OT&E was regularly reported to the Air Force’s management, without leading to changes in the process.

Safety Investigator’s Analysis
The investigators highlight two factors “that stand out as critical”, saying that together both were necessary for the occurrence:
- The collective’s unusually high position when accelerating the rotor
- That the rotor was accelerated with two engines, not just one
They go on to note that both are, “among other things, related to the design and use of the certified checklist and the locally developed checklist for start-up procedures”.
Each rotor blade has an elastomeric spherical bearing. After landing, the collective is put in Minimum Pitch On Ground (MPOG) before the engines are switched off. This puts a load on the elastomeric bearings. As long as the helicopter is on the ground without power on, the elastomeric bearings will gradually drift to a higher blade pitch and the collective will move correspondingly upwards. Investigators found only one pilot in the unit who was fully aware of this. The simulator did not replicate the phenomena either. It is therefore important that the collective is lowered to MPOG before the helicopter’s rotor is accelerated, to prevent the rotor from developing lift. This is normally done in connection with so-called flight controls full and free checks.
As the helicopter had not flown that day, the collective was therefore in a high position (53%) when the pilots boarded the helicopter. After the engines were started and the hydraulic system was pressurised, the collective stood at 45%, and the rotor blades had an angle of attack that was approximately 7º above the MPOG. Analysis showed that at 8º of attack angle (51% collective) the helicopter would lift off.
However, in this case the investigators explain that:
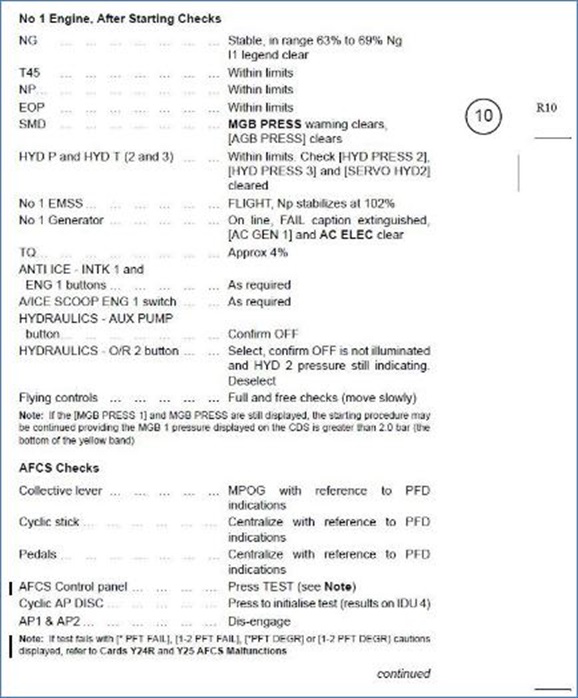
When PF came to the end of the No 1 Engine, After Starting Checks, PF told PM that they were not going to do the ‘Flight controls check’ or ‘AFCS test’. The PM had no objections to this.
Why the crew did not find it necessary or appropriate to carry out a complete start-up procedure is related to why the start-up was not a ‘strong situation’ for them.
The investigators then discuss the concepts of a ‘strong situation vs a weak situation’ in the context of the preparation for this ground run:
What in psychology is referred to as a strong situation is a situation where behaviour and actions are largely determined by clear frameworks. Checklists and repetition are factors that will create strong situations in some operational contexts; situations where there is no need for choices and assessments, but where actions can go on automatically and predetermined routines.
A start-up sequence will normally be a strong situation, as it does not change from time to time, and the procedure is set out in detail. During this start-up, however, there were several factors that made the pilots experience a weaker situation than one might expect:
Low experience: Both pilots had limited experience with launching the AW101. In addition…start-up training that should have been given before the training in full flight simulator (FFS) began, was not carried out… During the flight training in England, the program was also so hectic that on some trips they did a “hot swap…ie that they changed “student” in the helicopter without turning off the engines. This reduced the learning outcome with regard to start-up procedures and contributed to the start-up of AW101 still to a small extent being a routine operation for the crew.
New situation: PF had not previously started up the machine just to dry the compressors. PM had only done it once before. The department had not established a standard approach to this procedure.
That last statement is odd considering the earlier mention of Kneeboard Checklist v19.
Flexible framework: The documentation did not provide guidance on whether all the usual checks were necessary for such a start-up. That there are no separate procedure descriptions for [drying runs]. However, it occurs on some aircraft types in the Air Force that certain checklists are not performed…when the aircraft is not to fly, and this practice is not necessarily written down or approved. That the pilots have experienced this…most likely influenced their propensity to make their own adjustments.
Learned helplessness – little confidence in the framework: The pilots’ limited experience was that following the checks as they stood did not lead to success. The AFCS test failed routinely, which made it more natural to omit the check.
Flexible framework: During the conversion flight in England, some of the instructors, according to the pilots at OT&E, had had a “flexible” relationship with the use of checklists. Specifically, for some checklists there was variation in the order in which the individual checkpoints were made.
Little confidence in the framework: Earlier versions of the checklist from LH were perceived by pilots at OT&E as unfinished and unsuitable for much of the purpose.
None of these conditions indicated that the checklist should not be followed, but together they would have made it more natural for the crew to adapt their actions to their own assessments. If the procedures had been more incorporated / automated and had consistently given the desired results, this would have put stronger guidelines on the pilots’ actions in the situation.
The investigators concluded “it is easy to explain and understand that the AFCS test was omitted” but the omission of the full and free checks was “not as obvious”:
Even if the helicopter was not to fly, the rotor was to be accelerated. A rotor that rotates at full speed, makes the helicopter exposed to, for example, strong gusts and turbulence. It is therefore important that the flight controls are available and have normal results, and this is ensured through full and free checks.
Presumably, a mental link between full and free checks and the AFCS test has had some impact on PF’s decision. The way the checklist is designed, full and free checks can be experienced as a way to prepare for the AFCS test, as one checklist leads straight into the next; when you check after full and free checks that the controls are centered, you are already inside AFCS checks. The decision to omit AFCS checks has probably lowered the threshold for omitting full and free checks.
The investigators also consider that “the low perceived risk” of a drying run “contributed to the pilots not thinking much about possible changes in risk by omitting flight controls full and free checks”. Furthermore, surprisingly the unit “did not yet have a standardised understanding of how the Pilot Monitoring should assist Pilot Flying… A clear clarification of roles and tasks is the most effective way to avoid diffusion of responsibilities”. In the opinion of the investigators:
The fact that the pilots accelerated the rotor with both engines 2 and 3 was a result of incorrect and inconsistent training, lack of system knowledge and imprecise documentation.
If OT&E had had the time and opportunity to carry out a good internal standardisation process before the start of aircraft operations, it is possible that this could have highlighted the differences in procedures and made it possible to still clarify the correct procedure.
The investigators also comment that a third factor emerged as the situation developed, namely “if the crew had recognized the situation earlier and reacted by pushing the collective down, it is possible that the rollover could have been averted”. However, they postulate “sensory impressions also gave the pilots the illusion that the problem was a collapse of the right main landing gear. Thus, the pilots did not understand what was about to happen until it was too late”.

Safety Investigation Conclusions
The AW101-612 helicopter 0268 overturned because the rotor was accelerated by two engines while the collective was in a higher position than the minimum pitch on ground.
Lack of system knowledge and experience on the helicopter type, contributed to the pilots not discovering that the collective was high. Very poor continuity in flying over several years, and little systematic focus on risk in ground operations, contributed to low risk awareness among pilots in the situation. Together with little trust in documentation and procedures, this contributed to the pilots choosing to omit some items in the checklist. If all items in the checklist had been followed, the overturning would not have occurred. Errors in the training and imprecise documentation were crucial for the rotor being accelerated with two engines instead of one. Had the pilots always learned to accelerate the rotor with one engine, the overturning would not have happened. If the pilots had had better continuity, and if the organization and training had had more focus on risk in ground operations.
The training at Leonardo was characterized by ongoing, delayed development of helicopters, aids and documentation. The fact that the training was nevertheless accepted by Norway, albeit with reservations, contributed to uncertainty and a lack of faith in the personnel at AW101 OT&E unit. The delays also meant that the training for the first groups of personnel was extended over more than a year, and that the training that was to compensate for identified deficiencies in the training (delta training) was still not completed when the helicopter overturned. In addition, some of the personnel sent by the department, including the crew at this incident, did not have the background or continuity of the conversion program. These factors led to known and unknown gaps in the personnel’s competence, the consequences of which were difficult to know.
The organisation of AW101 OT&E unit as well as the lack of relevant and sufficient capacity at the professional authority, both contributed to the department receiving less support and professional follow-up than desired, including quality assurance of acquired competence.
The project organisation tried to compensate for delays and deviations at the supplier by adapting the timelines on the Norwegian side. Challenges with communication and cooperation between different parts of the project organization, led to increased strain and frustration and distorted the task of finding agreed solutions. Over time, ambitious progress plans, lack of personnel resources and delayed helicopter deliveries with deviating specifications have created a situation of persistent high time pressure for all parties in the project. The fact that all players nevertheless tried to be loyal to the current timeline affected quality assurance and risk management. It is the investigations assessment that the incident occurred during a period of persistently elevated and confusing operational risk.
Twelve safety recommendations were made.
Footnote
Coincidentally, on 4 June 2021 the Norwegian Council of State appointed Brigadier Rolf Folland as the new RNoAF chief (a 2 star post). Folland is currently commander of LOI at Rygge Air Base. He will start his new job on 11 August 2021. A helicopter pilot, Folland said:
Risk management is central to everything we do, and it requires awareness and active actions. Good procedures and clear frameworks are important, active leadership throughout the line is still crucial for the result.
Safety Resources
The European Safety Promotion Network Rotorcraft (ESPN-R) has a helicopter safety discussion group on LinkedIn. You may also find these Aerossurance articles of interest too:
- Military SAR H225M Caracal Double Hoist Fatality Accident
- A Second from Disaster: RNoAF C-130J Near CFIT
- Fatal Fall From B429 During Helicopter Hoist Training
- Hoist Assembly Errors: SAR Personnel Dropped Into Sea A UH-60M accident in Taiwan during a SAR exercise.
- USAF Helicopter Hoist Training Accident: equipment snagged on obstacle
- Fall From Stretcher During Taiwanese SAR Mission (NASC AS365N2 NA-104)
- Fatal Taiwanese Night SAR Hoist Mission (NASC AS365N3 NA-106)
- Fatal Powerline Human External Cargo Flight
- SAR Helicopter Loss of Control at Night: ATSB Report
- SAR AW139 Dropped Object: Attachment of New Hook Weight
- Human Factors of a Mali Mid Air Collision
- Loss of Control, Twice, by Offshore Helicopter off Nova Scotia
- Firefighting AW139 Loss of Control and Tree Impact
- Loss of RAF Nimrod MR2 XV230 and the Haddon-Cave Review
- Culture and CFIT in Côte d’Ivoire
- RCAF Production Pressures Compromised Culture
- Investigation into F-22A Take Off Accident Highlights a Cultural Issue
- ‘Procedural Drift’: Lynx CFIT in Afghanistan
- All Aboard CFIT: Alaskan Sightseeing Fatal Flight and Safety Culture
- MC-12W Loss of Control Orbiting Over Afghanistan: Lessons in Training and Urgent Operational Requirements
- C-130J Control Restriction Accident, Jalalabad
- AC-130J Prototype Written-Off After Flight Test LOC-I Overstress
- UPDATE 3 October 2021: French Cougar Crashed After Entering VRS When Coming into Hover
- UPDATE 27 November 2021: TCM’s Fall from SAR AW139 Doorway While Commencing Night Hoist Training
- UPDATE 5 March 2022: Taxiing AW139 Blade Strike on Maintenance Stand
- UPDATE 9 April 2022: SAR Seat Slip Smash (RCAF CH149 Leonardo Cormorant LOC-I)
- UPDATE 22 April 2023: Swinging Snorkel Sikorsky Smash: Structural Stress Slip-up
- UPDATE 8 July 2023: BK117 Offshore Medevac CFIT & Survivability Issues
- UPDATE 16 July 2023: SAR AW139 LOC-I During Positioning Flight
- UPDATE 13 July 2024: Fatal USCG SAR Training Flight: Inadvertent IMC
- UPDATE 25 May 2025: CHC Sikorsky S-92A Seat Slide Surprise(s)
Aerossurance is sponsoring OGUK‘s 2021 aviation seminar, this year a free webinar spread across 30 June and 1 July.
