Deadly Delay: Catastrophic USAF Bell/Boeing CV-22B Osprey 10-0054 Gear Box Failure
On 29 November 2023 US Air Force (USAF) Bell/Boeing CV-22B Osprey tiltrotor 10-0054 (call sign Gundam 22) of the 21st Special Operations Squadron (21 SOS), impacted the water 1/2 mile off the coast of Yakushima Island, Japan, while on approach to Yakushima Airport. The aircraft was destroyed, and all 8 crewmembers sustained fatal injuries. After this accident the V-22 fleet was grounded until 8 March 2024.
The USAF Accident Investigation Board (AIB) issued its report on 1 August 2024.

Context of the Accident Flight
The report notes that 21 SOS was a small unit with a high operating tempo. The period before the accident was reportedly particularly intense because of Air Force Special Operations Command (AFSOC) directions on achieving flying training requirements and several aircraft being down for base maintenance. The unit were also suffering a shortage of flight engineers / rear crew.
The aircraft was part of a two-ship formation, with a third airborne spare aircraft, that departed Yokota Air Base, near Tokyo, at 10:43 local time for a exercise with other US military units. The Aircraft Commander (AC), a Major with 1363 total flying hours, 953 on type over c 7 years. He was the lead air integration planner for the exercise and also the Airborne Mission Commander (AMC), unusual according to the AIB but allowed within AFSOC procedures. He was also an advocate of the type on Reddit as UR_WRONG_ABOUT_V22. This exercise had been months in the planning and there had already been a rehearsal on 7 November 2023.
On the day it was decided the V-22s would depart 30 minutes earlier than planned due to forecast headwinds and changed plans to refuel at MCAS Iwakuni.
10-0054 had 19 deferred defects (‘Red Diagonal’ or ‘/‘ items in USAF parlance). These are not listed or elaborated upon in the AIB report however. The AAIB report discussed the last aircraft maintenance on 10-0054 but does not mention the Time Since New and Time Since Overhaul of the left-hand proprotor gearbox (PRGB), the key assembly involved in the accident.
The Accident Flight
On departure at 10:43 10-0054 had suffered a mission computer ‘warm-start‘, resulting in a “software glitch”. En route they had to complete a 29 step checklist procedure to address this.
They arrived at MCAS Iwakuni at 12:31 after a 348 NM flight.

While there the crew of 10-0054 also had to deal with a number of advisory messages and several equipment failures, including two further warm-starts. They then departed at 13:09 to rendezvous with a US Marine Corps (USMC) Lockheed Martin KC-130J Hercules for air-to-air refuelling, en route to Kadena AB.
While en route at 13:50 the crew received the first left-hand PRGB CHIP BURN visual advisory on the Control Display Unit (CDU). This indicated an automatic ‘fuzz burn’ had occurred on a PRCG magnetic chip detectors. The chip detector fuzz burn feature is designed to burn off minor metallic debris but not large chips. Repeated fuzz burns however could indicate a incipient failure. When a fuzz burn can’t remove more substantial debris, a chip caution is displayed.
Each PRGB transmits power from one of the V-22’s Rolls-Royce T406 engines to one of the V-22’s proprotors, reducing the speed by 38:1 while increasing the torque.
The AIB don’t directly state who manufactures the PRGB, but imply it is Bell, as they have responsibility for transmission components.


There was a second left-hand PRGB CHIP BURN visual advisory just 23 seconds later and a third at c14:03.

Per Air Force (AF) guidance, a third PRGB CHIP BURN advisory requires the crew to ‘Land as Soon as Practical’; however, the guidance also allows the aircraft commander (AC) discretion in continuing the mission, based on circumstances of the mission and operating environment.
Military.com, who claim to have seen unpublished logs of the cockpit voice recorder, transcript report that during the flight one of the pilots:
…recalled his experience of getting “100 and some chip burns in a space of like 15 minutes” but without any other detectable issues on a flight earlier in his career. Another crew member mentioned…that he’d encountered the issue “on training sorties at Cannon” Air Force Base in New Mexico. The warnings are sufficiently common that pilots often don’t view them as critical, according to the [other] pilots who spoke to Military.com.
At the time the aircraft was still close proximity to mainland Japan and only c 10 miles from the nearest suitable airfield. After a brief discussion the AC however decided to continue the c 300 NM overwater flight to Kadena AB. The crew looked for any secondary indications of a problem, such as PRGB temperature warnings, which would demand the aircraft ‘Land Immediately’ (which includes ditching if necessary), but saw none.
At 14:09 a fourth chip burn advisory was received, and a fifth at 14:18. The crew however continued with their plan.
At 14:21, approximately 71 minutes after departing MCAS Iwakuni and approximately 3 minutes after the fifth chip burn advisory, a L PRGB CHIPS caution posted in the cockpit. A PRGB CHIPS caution directs the crew to ‘Land as Soon as Possible’ and be prepared to ‘Land Immediately’ if necessary.
Only at this point did the aircraft divert, to Yakushima Airport, then c 60 miles away, having transferred AMC role to the Deputy AMC.

The crew did not however consider any other closer landing locations…
…such as islands with helipads, suitable landing terrain on other islands, or runways, such as the one located on Satsuma-loJima, approximately 36 NM away. Once the AC committed to diverting to Yakushima Airport, the dialogue amongst the crew did not indicate a sense of urgency commensurate with the increasing seriousness of the condition.
As the V-22 neared Yakushima, there was a commercial aircraft on the runway preparing to takeoff. While the crew confirmed their diversion was an emergency, they were requested to enter a holding pattern to await the traffic to depart. At this time a CHIP DETECTOR FAIL advisory appeared. This seems to have erroneously confirmed an assumption the the earlier fuzz burn advisories were false.
When the V-22 did conduct its final approach at just prior to 14:40, the left-hand PRGB catastrophically failed, causing instant asymmetric lift, making the aircraft roll twice before impacting the water. The visualisation below show time in UTC (9 hours behind local time):


 The Japan Coast Guard (JCG) were alerted just 7 minutes after impact. No survivors were found.
The Japan Coast Guard (JCG) were alerted just 7 minutes after impact. No survivors were found.
The Accident Investigation & Analysis: Technical
Over “a period of years” Naval Air Systems Command (NAVAIR) Program Management Authority (PMA) for the V-22, PMA-275, had…
… conducted several PRGB-related safety assessments [which] found the likelihood of PRGB internal component failure to be ‘remote’ or ‘improbable’, but also indicated that total loss of aircraft and crew were possible, should PRGB internal components fail.
However, the AIB imply a failure in the risk management process:
Some safety assessments resulted in PMA-275 implementing program-wide changes to obviate or sufficiently mitigate the risk of PRGB internal component failure. But program-wide changes, such as changes requiring conservative aircraft operations in certain circumstances, were not always implemented, or were implemented in a manner that did not stress the severity of the risk.
Additionally, aircrew training on how to react to PRGB indications was not modified.
The findings of PRGB safety assessments also were not always communicated to the military services, limiting opportunities for service-specific changes to documentary guidance and training based on each service’s assessment of risk.
The AIB determined that one of the two ‘causal’ factors was:
Failure of the left-hand PRGB high-speed planetary [or epicyclic] section was most likely initiated by a crack in one of the high-speed pinion [or planet] gears and fatigue cracking of the associated pinion gear’s bearing cage, which eventually fractured through the high-speed planetary carrier assembly.


The AIB were enable to determine the origin of the crack or its propagation due to secondary damage.
At least one piece of the failed high-speed planetary pinion wedged in the high-speed carrier assembly, grinding against the high-speed sun gear’s teeth until they were completely removed.

The removal of the gear teeth prevented torque being applied to the left-hand mast.
Removal of the high-speed sun gear teeth is consistent with the evidence of grinding and circumferential scuffing on the high-speed sun gear set at the surface where all the teeth were missing. Once the left-hand PRGB failed, an onset of rapidly cascading malfunctions occurred, to include low/lost left-hand PRGB oil pressure, ICDS [Interconnecting Drive System] failure, and right-hand PRGB over-torque — all occurring less than six seconds after failure.
Investigation confirmed the chip detection system had worked as expected.

The V-22 is fitted with a form of Health & Usage Monitoring Systems (HUMS) from Bell, known as VSLED (Vibration, Structural Life & Engine Diagnostics). Post-accident analysis only found a detectable rise in vibration in the final 5 minutes of the flight according to the AIB report. Military.com claim an unpublished USMC report says…
…this system detected a 10-fold jump in vibrations after the first chip burn light, and “it steadily persisted for the remainder of the mishap flight.”
Though they provide no further detail and a sudden step change followed by steady vibration isn’t consistent with the failure mode that occurred.
Commander of AFSOC, Lt Gen Michael Conley, briefed reporters that AFSOC…
…has changed its protocol to direct aircrews to land as soon as practical after a single chip warning and then as soon as possible after the second.
NAVAIR are reportedly looking for a technical mitigation, only expected in 2026.
Another design solution is required to a another topical issue, hard clutch engagements, linked to other V-22 accidents. Currently, the input quill assembly is consequently being replaced every 800 hours. The fleet also is limited to flying within 30 minutes of a diversionary airfield.
The Accident Investigation & Analysis: Operational (inc Human & Organisational Factors)
The AIB used the DoD Human Factors Analysis and Classification System (HFACS) guide to evaluate the relevant human factors. HFACS has four main categories or levels: Organizational Influences, Supervision, Preconditions, and Acts.
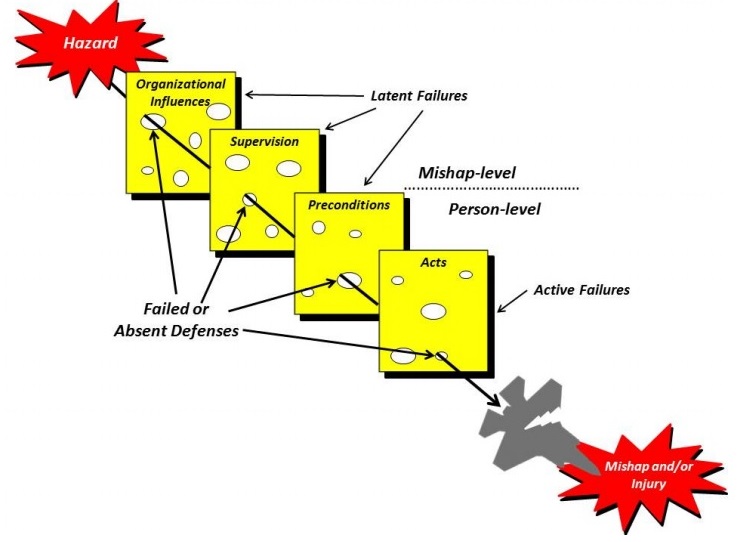
HFACS should encourage identifying factors beyond the ‘person level’ to consider wider, systemic organisational issues. Each level is further divided into multiple sub-categories:

While HFACS is a good taxonomy for classifying human factors and useful as an investigator’s aide mémoire during investigations, like MEDA, if it issued to guide and structure the actual investigation, can result in missing or downplaying other issues, especially non human factors related mechanical failures, and misdirecting the investigation.
The AIB coded the accident as follows (using the DoD HFACS V8 taxonomy). Seven factors were identified by the AIB, though they fail to directly link these to specific factual evidence:
- Organisational: Failure to Provide Adequate Information Resources
- Organisational: Purchasing or Providing Poorly Designed or Unsuitable Equipment
- Supervision: Authorized Unnecessary Risk
- Preconditions: Instrumentation and Warning Systems Issues
- Preconditions: Task/Mission In-Progress Re-Planning
- Preconditions: Ineffective Crew Resource Management
- Unsafe Acts: Inadequate Real-Time Risk Management
The second factor presumably links to the first, technical, ‘causal’ factor identified above. The other six are simplified into one further ‘causal’ factor (Pilot Decision Making) and two ‘substantially contributing’ factors (Inadequate Risk Management and Ineffective Crew Resource Management).
The AIB found Pilot Decision Making was causal:
These decisions caused a prolonged mishap sequence of events that removed any consideration of an earlier landing at a different landing location. Specifically, the AC’s decision to continue with the mission after the third chip burn advisory posted in the cockpit and the situation became Land as Soon as Practical; and AC’s decision to land at Yakushima Airport, instead of closer locations, after “L PRGB CHIPS” caution posted in the cockpit and the situation became a Land as Soon as Possible, were causal. The AC and crew did not plan for, deliberate, or even discuss closer suitable landing options after the “L PRGB CHIPS” caution posted.
The ‘substantially contributing’ Inadequate Risk Management’ factor consisted of three elements, the first involving NAVAIR:
(1) Program-Level Risk Management: The PRGB is a complex, critically important system, the failure of which can result in the total loss of aircraft and aircrew.
…safety assessments and their findings were given insufficient treatment at the program level and have been inadequately communicated to the military services, creating lack of comprehensive awareness of PRGB risks, and limiting opportunities to impose risk mitigation measures at the service or unit level.
Inadequate action at the program level and inadequate coordination between the program office and the services prevented comprehensive awareness of PRGB risks, and substantially contributed to the mishap.
This element of fleet management has strong echoes of the Haddon-Cave Nimrod report, though it still seems surprising that the V-22 community seems to have underestimated a type of failure mode that is a fundamental concern with rotorcraft transmission systems.
The other two elements were related to the conduct of the flight:
(2) Supervisory Risk Management: While using an AMC as a primary crewmember is permissible, the purpose of dedicating a crewmember to this duty is to allow the AMC to focus on the mission coordination and execution instead of operating the aircraft. Witness interviews during the AIB revealed that having a single person perform both AC and AMC duties was discussed during pre-mission planning. While acknowledged to be a non-standard practice, the mishap pilot was permitted to perform AC and AMC functions after determining mission complexity and environmental conditions were within acceptable risk limits (e.g., daylight, good weather).
The evidence highlights multiple times during the mishap sequence when the AC prioritized the exercise and coordination with other external participants involved in the exercise over internal coordination with the crew on safety of flight issues.
(3) Real-time Risk Management: When the crew received the third PRGB CHIP BURN advisory in the cockpit and had a Land as Soon as Practical condition, the crew was still very close to mainland Japan and several divert airfields. The AC made the decision to continue with the mission with very little discussion amongst the crew, no acknowledgment that there were divert options nearby, and no consideration given to the fact that continuing the mission would place the aircraft over open water for more than 300 miles before they reached Kadena AB.
The AC inadequately prioritized continuing the mission over considerations related to the risk of extended flight without redundancy in the left-hand PRGB.
The second and third element seem written with considerable hindsight bias and ignore the latent lack of “comprehensive awareness of PRGB risks” at least in part resulting from the first element. That latent lack of awareness is illustrated by Military.com:
“Before the crash, I didn’t think prop box chips were going to change into a lost rotor system as rapidly as it seems like it might have,” one airman told investigators after the crash, before adding that the investigation results would likely “change the calculus on how I handle a proprotor gearbox chip.”
The other ‘substantially contributing’ factor, Crew Resource Management (CRM) was described as follows:
Indications of ineffective CRM amongst the crew started to manifest while on the ground at MCAS Iwakuni and continued through the end of the mishap sequence. The crew failed to execute CRM duties at a level expected of a trained and qualified Air Force aircrew.
When the AIB say “manifest” they are likely to mean in retrospect to the investigators.
Most notably, the AC failed to leverage the diverse experience of the crew and seek inputs from the other crewmembers in the aircraft and in the formation. This would have enabled the AC to fully analyze the totality of the situation and discuss response options to the PRGB indications. The crew did not adequately address divert option, and the AC did not adequately re-orient the crew as the cockpit advisories and warnings progressed. The AC also failed to direct and/or delegate tasks appropriately as the situation progressed in complexity.
Once the AC decided to turn the aircraft towards Yakushima Airport, the crew did not adequately use the resources available to re-assess their location and explore other options. Other resources [available] included changing ForeFlight settings on the Electronic Flight Bag to more detailed aviation charts or changing chart scale on the Multi-Function Displays in the cockpit to search for other options. [Two rear crew members] were also available in the cabin to help alleviate cockpit workload and research potential Land as Soon as Possible options, but neither were tasked by the AC to support.
The AIB comment that:
The Co-Pilot made multiple passive attempts to prompt the AC to reconsider his response posture to the PRGB CHIP BURN advisories, but never made an assertive statement about his uneasiness with the evolving issues. The {rear crew] remained inappropriately focused on getting the Intelligence Broadcast Receiver operational, instead of backing up the ACP with the ongoing emergency procedure.
Though this needs to be seen in the light of the poor awareness of PRGB risks we discussed earlier.
This dynamic, unplanned sequence of events required the crew to work as a team to prioritize tasks, appropriately delegate the workload, and assertively offer professional opinions, even if the opinions differed from the MP. I find, by the preponderance of the evidence, the MC’s ineffective CRM prolonged the sequence of events and significantly contributed to the mishap.
Our Observations
There has been criticism of the AIB report primarily focusing on crew actions during the flight. A USAF AIB is however not a safety investigation to identify improvements but a…
…legal investigation to inquire into all the facts and circumstances surrounding this Air Force aerospace accident, prepare a publicly releasable report, and obtain and preserve all available evidence for use in litigation, claims, disciplinary action, and adverse administrative action.
In contrast, safety investigation reports, the ones that identify improvements, are not publicly released by USAF. However, this AIB report does give extensive detail to better understand this accident.
The depth of the technical investigation is limited, perhaps because design or productions failures occurred in industry, outside the scope of the AIB, and perhaps because the technical members of the AIB were maintenance NCOs.
We are not convinced the USAF AIB’s human factors analysis resulted in a proper understanding of why the crew made the decisions they made. It certainly underplays the likely self-induced pressure to complete the flight and plan continuation bias. This illustrates the danger of investigations that by design, or due to subversion, end up focusing on judging specific individuals rather than systemic improvement.
UPDATE 22 August 2024: “Flaw in Osprey Gears Was Known a Decade Prior to Deadly Japan Crash, Internal Report Shows”
…internal Safety Investigation Board report — which has not been made public — showed that…the high-speed gear that failed on Gundam 22 because of a single crack was “similar to those [failures] seen on seven previous…low-speed planetary pinion gears.”
[F]ive of those prior failures, which go back to 2013, were caused by “non-metallic inclusions” — a defect in the metal alloy from which the gears were made.
Investigators say that Gundam 22’s failures “most likely due to non-metallic material inclusion.”
In 2014, the Joint Program Office…was sent a formal risk assessment titled “Gear Metal Raw Material Impurities” by Bell Textron and Boeing… But, according to the Air Force internal investigation, the notice “did not adequately assess risk of high-speed gear failure.”
There was also no supporting test data gathered.
NAVAIR implemented contractual financial withholds in hope the contractor [Universal Stainless] would correct deficiencies in the [X-53 alloy] processing that had resulted in previous gear failures.
However, failures continued , indicating this approach was ineffective.
UPDATE 23 August 2024: The Air Current has also published a major article by Elan Head on the latest developments. In particular this article starts to expand the story beyond the narrower more crew-centric focus of the AIB report to consider the deeper airworthiness issues.
UPDATE 23 October 2024: A Hunterbrook expose on quality & culture at Universal Stainless. Universal Stainless is set to be acquired by Aperam in early 2025.
UPDATE 9 December 2024: Navy, Marine V-22 Ospreys Under ’Operational Pause’ After AFSOC Incident:
While performing a local training mission, a CV-22 Osprey from Cannon AFB, New Mexico. made a precautionary landing Nov 20, 2024. There were four personnel on board and no injuries were reported nor known damage to the aircraft because of the landing.
UPDATE 20 December 2024: NAVAIR Issues New V-22 Flight Restrictions Over Gear Box Concerns
“NAVAIR issued a fleet bulletin directing the inspection of V-22 Osprey to verify the flight hours on each Proprotor Gearbox prior to an aircraft’s next flight,” reads the Friday statement.
“Aircraft with PRGBs that currently meets or exceeds a predetermined flight-hour threshold will resume flights in accordance with controls instituted in the March 2024 interim flight clearance.“The metallurgical weakness within the V-22 transmission is thought to manifest itself relatively early in the component’s lifespan, meaning PRGBs with flight hours above the threshold have been deemed safe,” reads a Friday report from Flight Global.
UPDATE 2 January 2025: Elan Head of The Air Current reports that V-22 Ospreys will face ‘serious’ risks from flawed gears for foreseeable future. There are 41 V-22 gears made of X-53 alloy. It is now claimed that 20 V-22 gears of various part numbers had suffered degradations due to inclusions in 800,000 flying hours. While some resulted in chips being released and detected, in addition to the fatal accident in Japan, there were two “near misses” involving input idler helical gears had ” the potential to be catastrophic”.
One of these was the November incident at Cannon AFB, which occurred shortly before touchdown but resulted in a non-recoverable in-flight engine shutdown and proprotor gearbox case rupture.
The other occurred during a post-assembly rig test at the factory. This test was repeated after disassembly following a fire at the Bell Drives System Center at Grand Prairie, Texas in 2020.
“It is by happenstance that this gear was not installed on aircraft following its first successful green run,” the safety assessment states. “Had it been installed, a catastrophic gear failure could have occurred on-wing, potentially resulting in loss of personnel/aircraft.”
Moving to a triple melt process for future production is expected to result in an 85% overall reduction in inclusions.
While significant, this would not be sufficient to reduce the expected failure rate below one in a million flight hours.
Our Final Word
As we note above, the AIB report is tinged with hindsight bias. A public inquiry chaired by Anthony Hidden QC investigated 1988 Clapham Junction rail accident. In the report of the investigation, known as the Hidden Report, he commented:
There is almost no human action or decision that cannot be made to look flawed and less sensible in the misleading light of hindsight. It is essential that the critic should keep himself constantly aware of that fact.
Safety Resources
The European Safety Promotion Network Rotorcraft (ESPN-R) has a helicopter safety discussion group on LinkedIn. You may also find these Aerossurance articles of interest:
- AAR Bell 214ST Accident in Afghanistan in 2012: NTSB Report
- EC135 Main Rotor Actuator Tie-Bar Failure
- S-61N Damaged During Take Off When Swashplate Seized Due to Corrosion
- 2009 Newfoundland S-92A C-GZCH Accident: A Failure of Design and Certification
- AAIB Report on the Ditchings of EC225 G-REDW 10 May 2012 & G-CHCN 22 Oct 2012
- EC225 LN-OJF Norway Accident Investigation Timeline
- EC225 Main Rotor Head and Main Gear Box Design
- In-Flight Flying Control Failure: Indonesian Sikorsky S-76C+ PK-FUP
- Ungreased Japanese AS332L Tail Rotor Fatally Failed
- Canadian B212 Crash: A Defective Production Process
- Airworthiness Directive after Two Fatal Bell 430 Accidents: Main Rotor – Pitch Link Clevis Fractures Angola and South Africa
- Main Rotor Blade Certification Anomaly in Fatal Canadian Accident
- Swinging Snorkel Sikorsky Smash: Structural Stress Slip-up
- Missing Cotter Pin Causes Fatal S-61N Accident
- Inadequate Maintenance, An Engine Failure and Mishandling: Crash of a USAF WC-130H
- Investigation into F-22A Take Off Accident Highlights a Cultural Issue
- USAF Engine Shop in “Disarray” with a “Method of the Madness”: F-16CM Engine Fire
- ‘Crazy’ KC-10 Boom Loss: Informal Maintenance Shift Handovers and Skipped Tasks
- MC-12W Loss of Control Orbiting Over Afghanistan: Lessons in Training and Urgent Operational Requirements
- USAF RC-135V Rivet Joint Oxygen Fire
- Contaminated Oxygen on ‘Air Force One’
- USAF Parachutist Fatally Extracted Through Ventilation Door
- USAF T-38C Downed by Bird Strike
- USAF T-6A Texan II Lost in Inverted Stall
- When Red Bull Gives You More Than Wings…
- AC-130J Prototype Written-Off After Flight Test LOC-I Overstress
- C-130J Control Restriction Accident, Jalalabad
- USMC CH-53E Readiness Crisis and Mid Air Collision Catastrophe
- Fatal USCG SAR Training Flight: Inadvertent IMC
- Culture and CFIT in Côte d’Ivoire
- RCAF Production Pressures Compromised Culture
- SAR Seat Slip Smash (RCAF CH149 Leonardo Cormorant LOC-I)
- Loss of RAF Nimrod MR2 XV230 and the Haddon-Cave Review
- The Loss of RAF F-35B ZM152: An Organisational Accident
- C-130 Fireball Due to Modification Error
- Lessons from an AS365N3+ Gear Up Landing
- Second from Disaster: RNoAF C-130J Near CFIT
- SAR AW101 Roll-Over: Entry Into Service Involved “Persistently Elevated and Confusing Operational Risk”
- French Cougar Crashed After Entering VRS When Coming into Hover
- What Lies Beneath: The Scope of Safety Investigations
- How To Develop Your Organisation’s Safety Culture
- James Reason’s 12 Principles of Error Management
- Psychology of Blame
- UPDATE 2 January 2025: Startled Shutdown: Fatal USAF E-11A Global Express PSM+ICR Accident